

MYTHS ABOUT BIPOLAR DISORDER (BD) can stand in the way of providing appropriate care for persons who have this condition. One myth—that those with BD should be able to control it by will alone—may prevent sufferers from adhering to therapy or from seeking care in the first place. This article helps you improve patient outcomes by explaining what BD is, how it manifests, and how it’s managed.
The sixth leading cause of disability in the world, BD is an episodic, chronic illness affecting approximately 5.7 million adult Americans. It’s marked by extreme changes in mood, thought, behavior, and energy level. Mood swings can vary in intensity, length, and the degree to which they interfere with functioning. Severe mood swings can last weeks or months and may severely disrupt the person’s life.
BD occurs in all races, ethnic groups, and social classes. Although it affects males and females equally, males tend to have an earlier onset. BD reduces life expectancy by 9.2 years, with up to 33% of sufferers attempting suicide and 15% completing it.
About 69% of persons with BD are misdiagnosed, delaying proper treatment 5 to 10 years. The most common misdiagnosis is major depressive disorder—probably because most people with BD seek help when they’re so depressed they can’t function, not when they’re having a manic episode and believe they can accomplish anything.
Causes
Research shows that in persons with BD, neuropathologic changes occur in the amygdala, a structure deep within the brain’s temporal lobes that plays a key role in memory and processing of emotions. Studies also reveal abnormal levels of the neurotransmitters norepinephrine, serotonin, dopamine, glutamate, and gamma-aminobutyric acid (GABA) in this area. Norepinephrine plays a role in mood regulation, arousal, and memory; dopamine acts as the brain’s natural reward system. Serotonin is involved in mood regulation, anxiety, pain perception, appetite, sleep, sexual behavior, and impulsive behavior. Glutamate is the primary excitatory neurotransmitter; GABA, the primary inhibitory transmitter. Evidence suggests that levels of norepinephrine, serotonin, and dopamine are decreased in people with depression. Increasing GABA levels and decreasing glutamate levels can improve or stabilize mood.
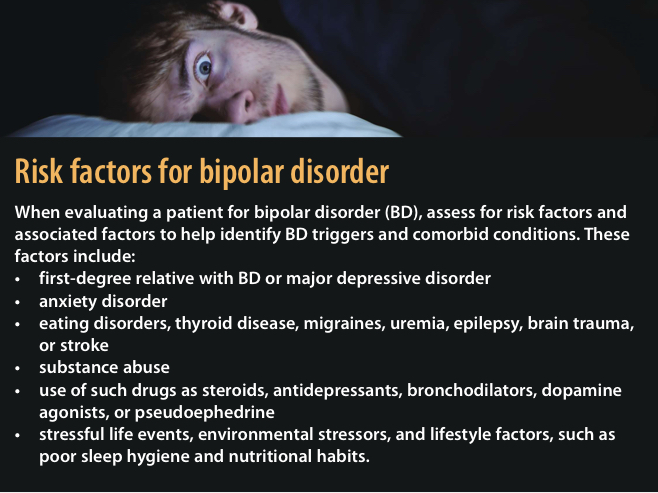
Research with twins suggests BD is inheritable: When one twin has BD, the other is at high risk for developing it. Also, more than 66% of people with BD have a first-degree relative who suffers from BD or a major depressive disorder.(See Risk factors for bipolar disorder)
Signs and symptoms
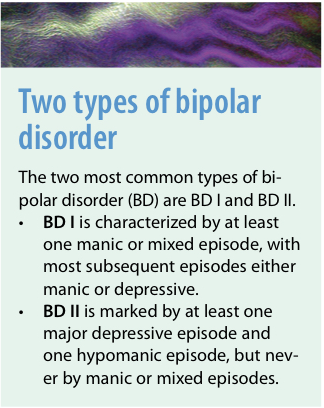
People with BD frequently report experiencing highs (mania) and lows (depression). Men with BD are more likely to present with a manic episode, whereas women are more likely to present with a depressive episode. (See Two types of bipolar disorder )
 A manic episode is a distinct period of abnormally elevated, expansive, euphoric, or irritable and agitated mood that lasts at least a week and severely impairs the ability to function. During this time, the person may think he or she is functioning exceptionally well. According to criteria from the Diagnostic and Statistical Manual of Mental Disorders (4th edition, text revision; DSM-IV-TR), at least three of the following must be present to qualify as a manic episode:
A manic episode is a distinct period of abnormally elevated, expansive, euphoric, or irritable and agitated mood that lasts at least a week and severely impairs the ability to function. During this time, the person may think he or she is functioning exceptionally well. According to criteria from the Diagnostic and Statistical Manual of Mental Disorders (4th edition, text revision; DSM-IV-TR), at least three of the following must be present to qualify as a manic episode:
- inflated self-esteem, extreme optimism and self-confidence, excessive irritability, or aggressive behavior
- decreased need for sleep
- increased talkativeness or pressure to keep talking
- flight of ideas or racing thoughts
- distractibility
- increased goal-directed activity or psychomotor agitation
- excessive involvement in pleasurable activities likely to cause negative consequences, such as spending sprees and sexual indiscretions.
Untreated, a manic episode can last 3 to 6 months. Psychotic signs and symptoms, including hallucinations and delusions, may occur and require hospitalization.
Hypomanic episodes
A hypomanic episode is an abnormally elevated, expansive, or irritable mood lasting at least 4 days that doesn’t severely impair the ability to function. It’s marked by three or more of the features listed above for manic episodes. During this time, the person may appear extremely happy and believe he or she is functioning well, with high productivity and creativity. No psychotic features are present and hospitalization rarely is required.
Diagnosis
Diagnosis rests on a thorough history and exclusion of other conditions. Depending on symptom severity, the patient’s perceptions may be incomplete or inaccurate. You may need to interview family members or significant others to obtain a clearer picture of the patient’s signs and symptoms, medical history (including previous bipolar episodes), and family history.
Many clinicians administer the Mood Disorder Questionnaire, a short self-report instrument, to screen for BD and augment a complete mental status assessment. This tool asks whether the patient has experienced symptoms, if multiple symptoms have occurred during the same time period, and how much of a problem the symptoms have caused. The patient’s responses help guide treatment.
Pharmacologic treatment
Acute treatment focuses on decreasing symptoms and restoring the patient’s coping and functioning ability. After stabilization, the goal is to prevent relapse and limit symptom duration and severity. The odds of a relapse are 85% to 95%, with medication noncompliance a major cause.
Mood-stabilizing drugs are the mainstay of treatment. Algorithms developed from randomized controlled drug trials and expert opinion guide treatment. Severe manic or mixed states typically call for either lithium (an antimanic agent) or valproate (an anticonvulsant), plus an antipsychotic. For less severe manic episodes, lithium, valproate, or an antipsychotic may be used alone.
Anticonvulsants
Anticonvulsants, such as valproate, carbamazepine, and lamotrigine, are first-line drugs used alone or in combination with each other or second-generation antipsychotics, because of their mood-regulating efficacy (especially in mania). Valproate and carbamazepine are recommended for mania; both require regular monitoring of plasma drug levels and liver function. Carbamazepine must be used cautiously because it can cause agranulocytosis and anemia; oxcarbazepine can be substituted if needed.
Benzodiazepines are used to manage BD in patients with severe anxiety or insomnia. Some experts recommend clonazepam for its anticonvulsant and GABA-enhancing effects.
Lithium
Lithium is still recommended for BD, although it’s less commonly used today than in the past because of its extensive adverse effects, such as polydipsia, polyuria, weight gain, hypothyroidism, acne, and toxicity risk.
Drug therapy for BD with depression
Although not used as often, lithium remains a first-line treatment for BD with major depressive episodes. Lamotrigine is also a first-line drug in this situation. When used alone, antidepressants can trigger a manic episode and aren’t recommended unless a mood regulator also is prescribed.
Patients with BD plus depression and psychotic symptoms typically receive antipsychotics. Because lithium and anticonvulsants take longer than 1 week to treat mania, antipsychotics typically are given to manage acute mania symptoms until mood regulators reach effective plasma levels. The second-generation antipsychotics olanzapine, risperidone, quetiapine, ziprasidone, and aripiprazole are approved as monotherapy for BD in patients with hallucinations and delusions. But some clinicians regard several atypical antipsychotics (especially olanzapine) as second-line choices because of the risk of weight gain, dyslipidemia, and diabetes mellitus type 2.
Electroconvulsive therapy
Research shows electroconvulsive therapy (ECT), which causes seizures that affect mood regulation, is effective for patients with treatment-resistant BD. Typically, the patient receives 6 to 10 treatments over several weeks. ECT is considered safe and effective today because it’s done with anesthesia in a controlled setting. Adverse effects, such as headache and memory loss, subside once treatment ends.
Nonpharmacologic treatment
Although many BD patients take multiple medications, they should receive nonpharmacologic treatments simultaneously for optimal stabilization and relapse prevention. BD patients can benefit from:
- psychosocial therapy and psychotherapy addressing illness management
- early relapse detection
- reinforcement of medication adherence
- lifestyle changes that enhance coping ability through realistic expectations and modifying behaviors
- support group work or individual counseling.
Adequate sleep is important to stabilization; so are realistic expectations. The clinician should create an action plan to use when early relapse symptoms occur.
Cognitive-behavioral therapy, interpersonal relationship therapy, psychodynamic therapy, family therapy, and group therapy (including psychoeducational therapy) may be used alone or in combination. Cognitivebehavioral therapies focus on changing negative thought processes. Psycho-educational therapy is a type of group therapy that combines support and self-help strategies. The most common type of group facilitated by nurses, psycho-educational therapy starts in the acute setting and continues during maintenance. Priorities for this therapy include:
- establishing a stable sleep pattern
- developing a regular activity pattern
- avoiding alcohol and other substances
- asking for and using support from family and friends
- decreasing stress at work and at home
- identifying early warning signs
- developing problem-solving and emotional tolerance and regulation skills.
Patient needs, cost, and the expected duration of therapy influence the type of therapy selected. Factors that may increase treatment success include a good patient-provider relationship, a supportive environment, medication adherence, and the patient’s willingness to explore and try new coping strategies.
Nursing management
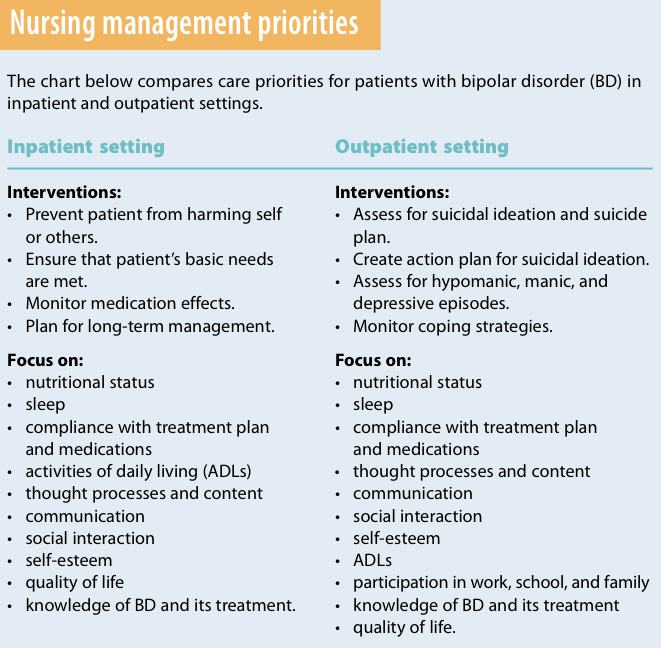
BD can be managed in both inpatient and community settings. Acute short-term treatment goals differ from long-term maintenance goals. For acute short-term treatment, the goals are stabilization and safety; for long-term maintenance, goals include preventing relapse and limiting the duration and severity of manic or depressive episodes. To ensure continuity of care, make sure you understand treatment priorities and goals in both settings. (See Nursing management priorities)
For inpatient treatment, signs and symptoms of depression or mania determine the goals and focus of management. Safety is the first priority. Patients with depression are at high risk for self-harm. Those admitted with a manic episode may show signs and symptoms of irritability, delusions, impulsivity, and anger; they also are at risk for harming themselves or others. Medications help stabilize the patient, allowing effective implementation of other treatments.
For outpatient management, goals include reestablishing the patient’s previous functioning level, identifying triggers, preventing relapse or reducing its severity, and limiting the duration of future episodes. In community settings, monitor the patient’s treatment responses over time.
Patient teaching
Provide education about BD to the patient and family members, emphasizing the need for medication adherence and effective coping and lifestyle changes. If your patient is taking lamotrigine, be aware that a serious rash, such as Stevens-Johnson syndrome (indicated by involvement of at least one mucous membrane), can occur at low dosages and may arise early in treatment. Widespread rashes involving the mucous membranes—especially with fever or sore throat—demand intervention. Teach patients to contact their healthcare provider if such a rash develops.
Rising to the challenge
BD patients experience a wide range of signs and symptoms that affect their daily functioning. Healthcare providers must understand the disorder, patient and family perceptions, and management options. Providing supportive, holistic nursing care helps dispel myths and enhances patients’ quality of life.
Selected references
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th ed., text revision. Washington, D.C.: American Psychiatric Association; 2000.
Depression and Bipolar Support Alliance. Bipolar disorder. Updated February 5, 2009. http://www.dbsalliance.org/site/PageServer?pagename=education_bipolar. Accessed June 6, 2011.
Hirschfeld R. Guideline watch: Practice guidelines for the treatment of patients with bipolar disorder. In: American Psychiatric Association Practice Guidelines for the Treatment of Psychiatric Disorders: Compendium 2006. Washington, DC: American Psychiatric Association; 2006:841-906.
National Alliance on Mental Illness. Bipolar disorder. www.nami.org/Template.cfm?Section
=By_Illness&Template=/TaggedPage/TaggedPageDisplay.cfm&TPLID=54&ContentID=23037. Accessed June 6, 2011.
The authors teach at Ball State University School of Nursing in Muncie, Indiana. Ann Wieseke and Diana Bantz are associate professors. At the time this article was written, Deborah May was an assistant professor at Ball State University School of Nursing.

















5 Comments.
I was diagnosed with BD when I was 21, and I am now 46 yrs old. I have been dealing with it all my life and I can tell you it most definitely is real. When I do all that I can to stay in balance including taking medication, I love my life. When I get sloppy or think that there is some other way to handle it, I learn the same painful lesson over again. This is great information on this site and a great reminder to how careful we all need to be to enjoy all that life has to offer.
Bi Polar is real. Ive been diagnosed the last 7 years. People like Dana down at the bottom do not help the situation any. The stigma is ugly. You say we aren’t being responsible but I say worry about your own trolling addiction. I’ll keep taking my medications and how about you try to stop discouraging real sufferers and their loved ones from seeking help. Get Help it exists and to a lot of people mental health treatments can be free or very cheap. It wont hurt to try.
BD is a real disorder. I seen it with my mom, my self and now my daughter and we were all raised in different enviornments.
I am greatful for the information posted above. My husband was treated for many years for depression and things were still not right. We finally have a Nurse Practitioner that listened to all of the symptoms and diagnosed him with BD. My husband is now on the right treatment. He is a better husband and father thanks to the correct diagnosis and treatment.
Bipolar disease is overdiagnosed and often a cop-out for people who just don’t want to be responsible for their lives and their behavior