BACKGROUND
PATIENT TRANSFER BETWEEN facilities is a complex process that can lead to errors (Rosenthal, Doiron, Haynes, Daniels, & Li, 2018). errors can occur within health systems when patients are transferred internally from one location to another. The Joint Commission lists eight steps to an effective handoff: 1. Determining critical information to share, 2. Utilizing standardized tools, 3. Not relying on electronic or paper communication only, 4. Combining and communicating all sources of information, 5. Ensuring minimum information is received, 6. Staying focused during hand-offs, 7. Including all team members, 8. Utilizing resources of the electronic health record (2017). An initial problem identified prior to moving through the transfer and handoff process was the appropriate selection of patients eligible for transfer. This concern led to the formation of an interdisciplinary performance improvement team to find solutions to improve the processes used to transfer patients between facilities within a large academic health system, MU Health Care.
PROJECT OVERVIEW
In July of 2022, a nurse led interdisciplinary team comprised of nursing leaders, physician leaders, performance improvement specialists, emergency medical services leaders, and a data scientist was formed. The problem statement established by the team was: The process of identifying appropriate patients to transfer from University Hospital (UH) to the Missouri Orthopedic Institute (MOI) is inconsistent and inefficient. This ultimately leads to patient and staff dissatisfaction, heightens the risk to patient safety, and creates a potential for multiple transfers between facilities.
From that, a specific aim was identified to increase the total number of appropriate patient transfers from UH to MOI. By working on the process, we can expect to increase MOI medicine team bed utilization, increase bed capacity at UH, decrease patient safety risks, and increase staff satisfaction. The established project outcome was to see a decrease in patient return transfers from MOI back to UH. The team met biweekly and reported to executive leadership bi-monthly as it progressed through building a solution to help identify patients appropriate for an intra-facility transfer. University of Missouri Internal Review Board certified the project as a quality improvement project through the human subjects research determination form.
INTERVENTION
The intervention the group developed and implemented was a tool that used an established set of criteria to screen patients at UH for appropriate transfer criteria to MOI. The electronic medical record (EMR) screening tool utilized the exclusion criteria of upcoming procedure needs, bed assignments, primary team assignments, treatment needs, and patient age. The EMR tool displayed patients ranked from most appropriate for intra-facility transfer to least appropriate for intra-facility transfer. The dashboard provided MOI nursing leadership and the MOI medicine team with a list of patients to further evaluate for intra-facility transfer from UH to MOI.
EVALUATION
Upon implementation of the patient screening tool the team evaluated two metrics. The first was the appropriateness of patients transferred from UH to MOI. Evaluation was completed through multidisciplinary (nursing and physician) chart reviews for patients who required transfer back to UH. The goal was to increase the number of appropriate initial transfers to MOI and decrease the return transfers. Upon evaluation, it was found that with the use of the screening tool, 100% (n=117) of patients transferred to MOI appropriately fit criteria at the time of initial transfer.
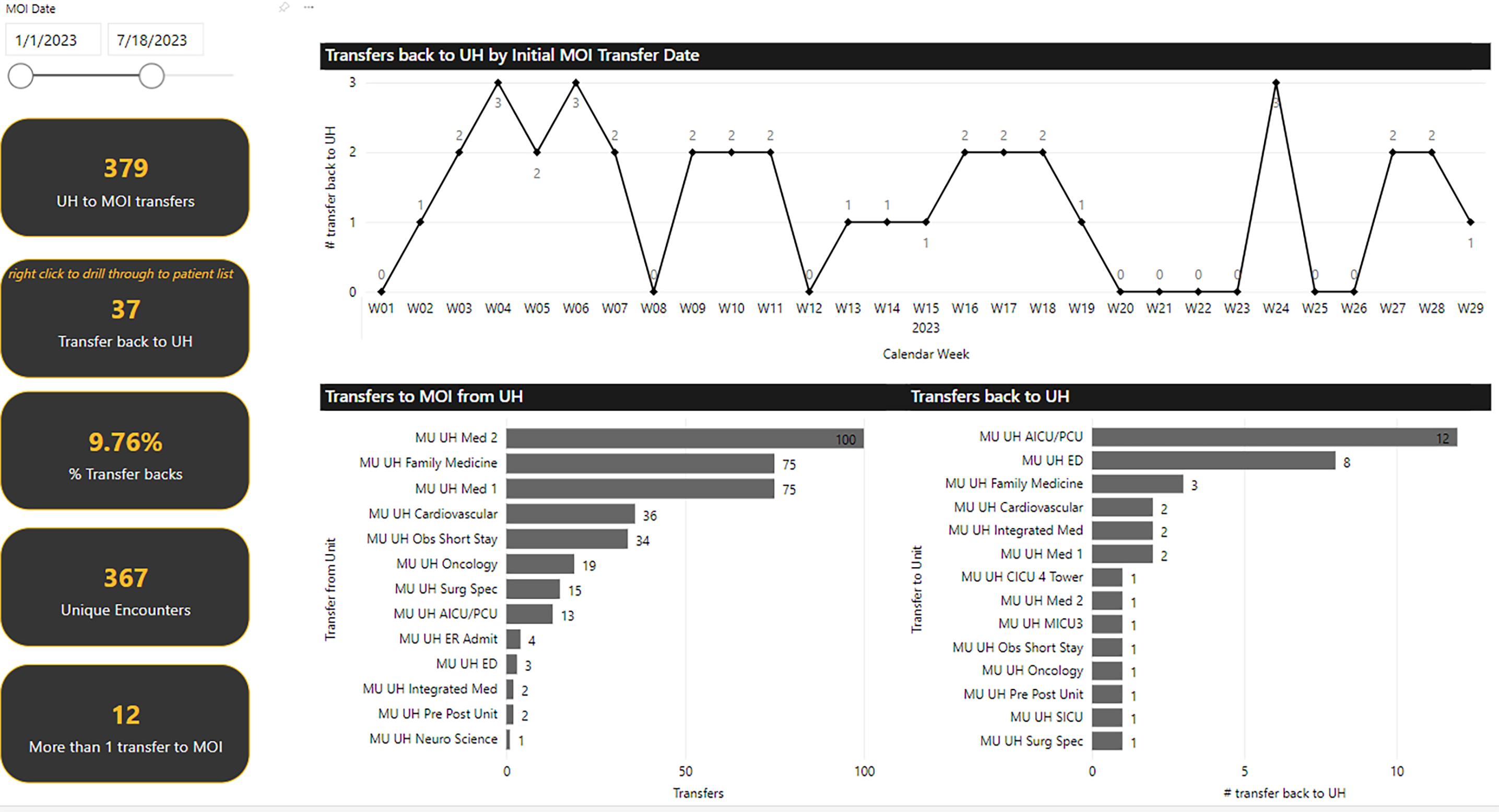
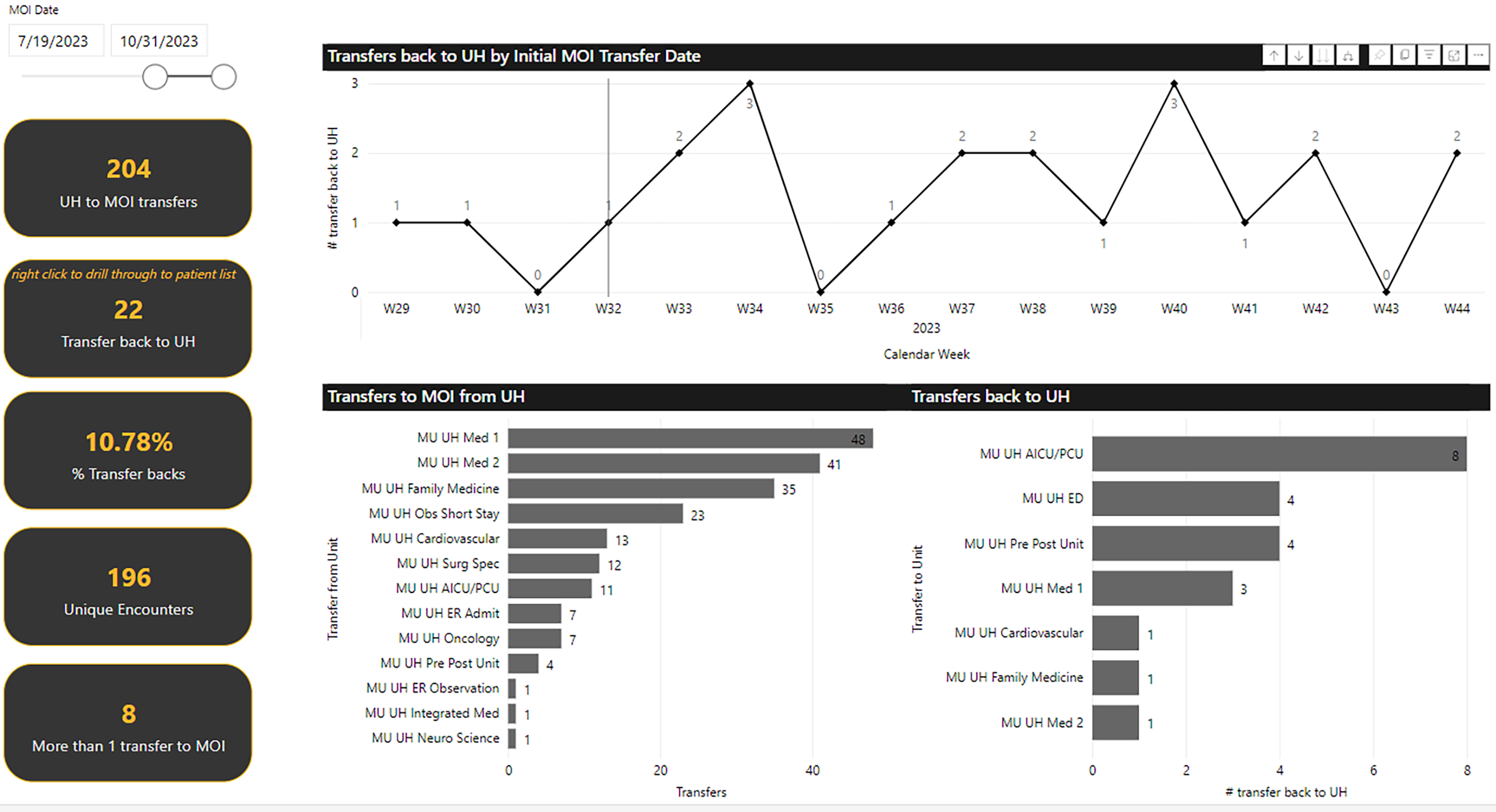
The second evaluation was the number of repeat transfers between UH to MOI. The repeat transfers were monitored through the patient’s admitted location and reported through an accessible dashboard. The goal was to reduce the number of repeat transfers between UH and MOI by utilizing the screening tool. Upon review an increase in the number of repeat transfers from UH to MOI was seen. Prior to use of the screening tool, a repeat transfer rate was 9.8% (n=379) After the screening tool was implemented, the repeat transfer rate was 10.78% (n=204). The majority of post-intervention transfers back were to higher levels of care, 55%. With the increase in transfers back while utilizing the screening tool, the team set benchmark measures to ensure that appropriate initial transfers were still taking place. The result illustrates how patients can wax and wane from anticipated treatment pathways and may require additional resources.
In addition, subjective information that illustrated the success of the project was collected from team members. From nursing leadership, it was found that the amount of time to find appropriate patients was reduced from one hour to 20 minutes and that staff confusion and frustration from the transfer process had been reduced. From physician leadership, it was found that the process was more transparent, and the amount of time screening patients was reduced. EMS leadership identified that the time to investigate serial transfers was significantly lower. These subjective findings allowed the team to reinforce the value of screening tool utilization.
CONCLUSIONS
With the complexity and risk of errors for patient transfers, it is important to ensure appropriate patient selection to meet the Joint Commission’s recommendations for effective patient hand-offs. Employing EMR resources along with an easily accessible dashboard to prescreen patients can serve as an effective tool to expedite processes and ensure that patients are in the right place at the right time to receive the right care.
Reference
Rosenthal JL, Doiron R, Haynes SC, Daniels B, Li ST. The Effectiveness of Standardized Handoff Tool Interventions During Inter- and Intra-facility Care Transitions on Patient-Related Outcomes: A Systematic Review. Am J Med Qual. 2018 Mar/Apr;33(2):193-206. doi: 10.1177/1062860617708244. Epub 2017 May 3. PMID: 28467104.
The Joint Commission. Inadequate hand-off communication. Sentinel Event Alert 58, September 12, 2012. https://www.jointcommission.org/-/media/tjc/documents/resources/patient-safety-topics/sentinel-event/sea_58_hand_off_comms_9_6_17_final_(1).pdf