

While relaxing at home at about 4 PM, Alan Sarangelo, a retired 62-year-old respiratory therapist, feels the left side of his face growing numb. His wife, a nurse, suspects he may be having a stroke and immediately calls 911.
At 4:25 PM, Mr. Sarangelo is emergently transported to the emergency department (ED) of a Joint Commission-accredited primary stroke center. There, clinicians note his slurred speech, left-sided facial drooping, and difficulty holding his left arm up for more than a few seconds. His vital signs are blood pressure (BP) 189/112 mm Hg; pulse, 112 beats/minute; respiratory rate (RR), 23 breaths/minute; and oxygen saturation 96% on room air. Mr. Sarangelo’s wife tells them he has a history of type 2 diabetes, hypertension, and hyperlipidemia.
For stroke patients who meet certain criteria, thrombolytic therapy to break down blood clots is the primary treatment option. Tissue plasminogen activator (tPA), the most frequently used thrombolytic, is a protein that catalyzes the conversion of plasminogen to plasmin, the major enzyme that breaks down clots. To be eligible for tPA, the patient must reach a certified stroke center as soon as possible after symptom onset. By some estimates, only 3% to 5% of stroke patients get to thehospital in time to receive tPA.
Despite campaigns to educate the public to seek immediate help for symptoms of a suspected stroke, many people wait hours before doing so. Or instead of calling 911, they take the family car. Obviously, they don’t realize that minutes lost mean brain tissue lost or that stroke is a life-threatening emergency that warrants an immediate 911 call. (See How prevalent is stroke?)
As a nurse, your assessment of the patient’s signs and symptoms and your knowledge of stroke treatment are vital. All nurses should know the warning signs of stroke, teach patients and families about these key clues, and spread the word about the importance of getting immediate help. Early assessment and rapid treatment are critical to saving brain cells—and lives.
Stroke pathophysiology
Stroke occurs in two main types—ischemic (caused by a clot) and hemorrhagic (caused by bleeding in the brain). Both types deprive brain tissue of oxygen, leading to cell death and permanent brain injury.
Approximately 87% of strokes are ischemic. Hemorrhagic strokes account for only about 13% of strokes but are more lethal than ischemic strokes, causing roughly 40% of all stroke deaths. (See Facts about hemorrhagic stroke.) An ischemic stroke can be thrombotic or embolic.
• A thrombotic stroke occurs when a thrombus (clot) forms in a cerebral artery.
• An embolic stroke occurs when a thrombus migrates to the brain from elsewhere in the body, typically the heart or a carotid artery.
Ischemic stroke potentially can be treated with thrombolytic therapy if the patient meets strict administration criteria. Transient ischemic attacks (sometimes called ministrokes) are a type of ischemic stroke. (See Spotlight on TIAs.)
Stroke risk factors
Nearly half (49%) of Americans have at least one of the three major risk factors for stroke—high blood pressure, high cholesterol, or smoking. These risk factors can be modified by behavioral changes. Other modifiable risk factors include physical inactivity, obesity, and diabetes type 2.
Also, stroke is strongly linked to atrial fibrillation (AF): About 15% of persons who have strokes have AF, an arrhythmia in which blood may pool in the heart and form a clot that travels to the brain to cause a stroke. Proper AF management with anticoagulants can help prevent a stroke.
Nonmodifiable risk factors for stroke include the following:
• Age: For each decade after age 55, the odds of having a stroke approximately double.
• Personal history of stroke, TIA, or myocardial infarction (MI): Stroke risk increases greatly for people who’ve already had a stroke or MI. TIAs are strong predictors of future stroke.
• Family history: Having a first-degree relative who has had a stroke increases your stroke risk.
• Race: African-Americans have almost double the risk of first-ever strokes compared to whites. They also have higher stroke death rates.
• Gender: Women have more strokes than men and are more likely to die from them. Their increased risk stems partly from use of oral contraceptives and postmenopausal hormone replacement therapy.
Assessing patients for stroke
Stroke or suspected stroke is an emergency that calls for an immediate response. If you suspect your patient is having a stroke, activate a stroke alert, notify the physician, or call 911 (depending on your location).
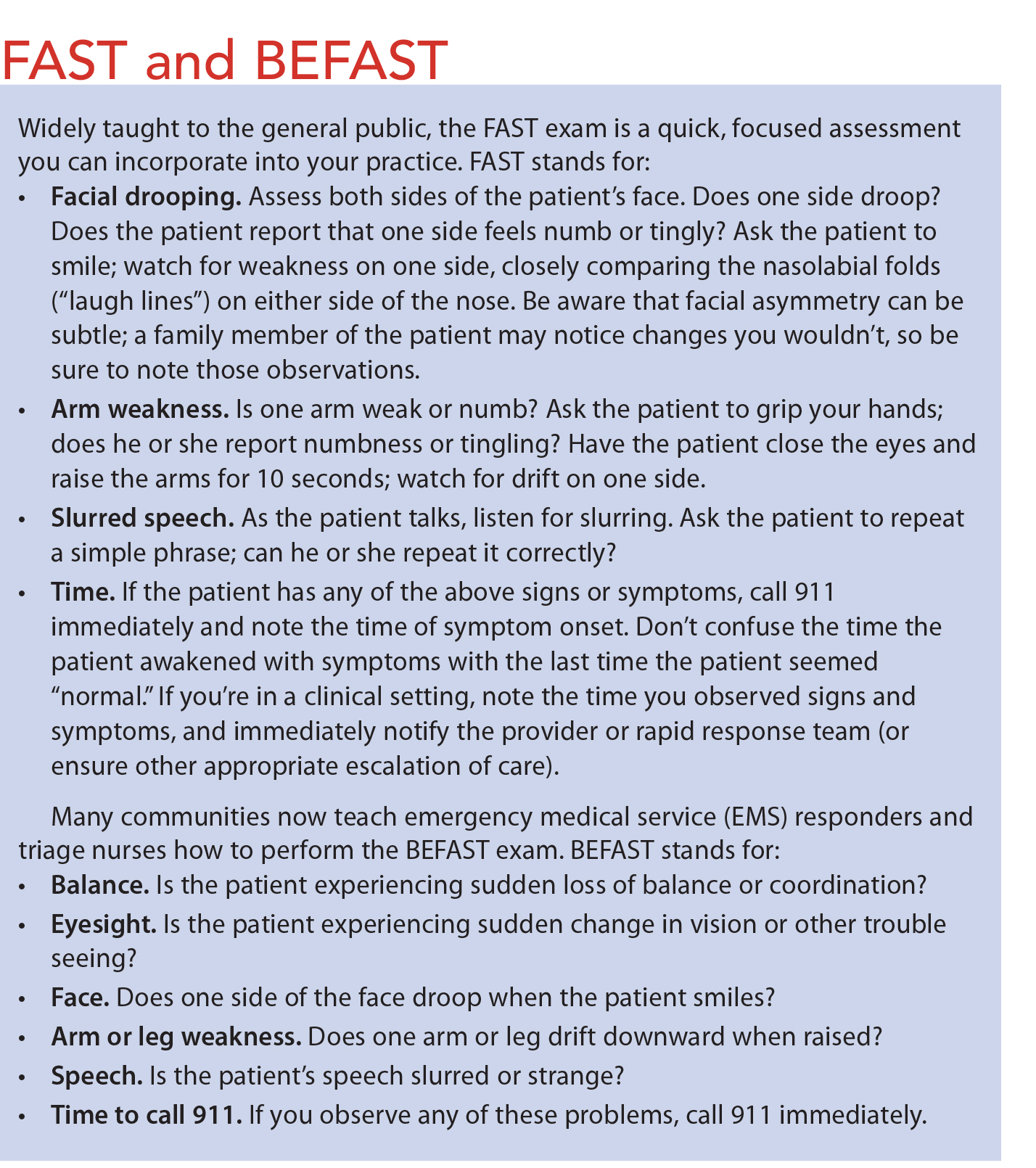
To detect stroke quickly, first responders and other frontline providers use several well-known stroke scales, including the Cincinnati Stroke Scale and the Los Angeles Prehospital Stroke Scale. These scales share many similar elements, some of which are part of the FAST exam. (See FAST and BEFAST.)
The National Institute of Neurological Disorders and Stroke describes these major signs and symptoms of stroke:
• sudden numbness or weakness of the face, arms, or legs
• sudden confusion or trouble speaking or understanding others
• sudden trouble seeing in one or both eyes
• sudden trouble walking, dizziness, or loss of balance or coordination
• sudden severe headache with no known cause.
NIHSS and mNIHSS tools
Nurses who manage patients with acute stroke should develop expertise in administering the National Institutes of Health Stroke Scale (NIHSS), a tool that objectively quantifies a patient’s stroke impairment. The NIHSS consists of 11 items that rate the patient’s neurologic functioning, including level of consciousness, best gaze, visual fields, facial palsy, motor function, limb ataxia, sensory function, language, articulation, and inattention. The lower the score, the better the patient’s prognosis. The modified NIHSS (mNIHSS), a short version of the NIHSS, is less widely used but has better inter-rater reliability than the older NIHSS.
Your role in thrombolytic therapy and stroke alert activation
Your initial evaluation of a patient with a suspected stroke should include airway, breathing, and circulation, followed by neurologic assessment using either the NIHSS or the mNIHSS, per facility policy. If you suspect a stroke, immediately notify the attending physician, who will call for a stroke alert or code stroke.
A stroke alert or code stroke should run as efficiently as a code blue. Nurses should have preassigned roles that include drawing blood for lab work, maintaining communication with the patient’s family, and communicating with physicians and computed tomography (CT) staff.
Connect the patient to the cardiac monitor to track heart rhythm and use an oximeter to monitor oxygenation status. Implement aspiration and seizure precautions. Be aware that controversy exists over whether to elevate the head of the bed because this can increase intracranial pressure; however, increased aspiration risk (from not elevating the head of the bed) must be considered. Be sure to followfacility policy and procedure.
Stroke alert team protocol
The following steps constitute a typical stroke alert team protocol with the goal of obtaining a CT scan within 25 minutes of the patient’s hospital arrival.
Blood pressure monitoring
If the patient is a tPA candidate, maintain systolic BP below 185 mm Hg and diastolic BP below 110 mm Hg. Expect the physician to order labetalol or nicardipine to lower BP to goal pressures. If BP can’t be maintained below these goals, the patient is not a tPA candidate. Caution: Rapidly lowering BP is contraindicated because it may reduce perfusion to ischemic brain tissue.
CT: The gold standard
A noncontrast CT scan of the brain is the diagnostic test of choice to rule out hemorrhagic stroke in an emergency. Time is critical, as studies show that delays in administering tPA correlate with poorer patient outcomes. The patient should undergo a CT scan within 25 minutes of arrival at a stroke center. The radiologist should read the CT scan within 45 minutes of patient arrival. A hemorrhagic stroke “lights up” the scan image with hyperdense areas of bleeding, making the patient ineligible for tPA. The scan also can detect a brain tumor, which also rules out tPA. A nurse, physician, or both must accompany the patient (who should be on a monitor) to the CT scan.
Inclusion and exclusion criteria for tPA
For patients with ischemic stroke, the goal is to rapidly restore brain perfusion to save ischemic but viable brain cells. Patients who receive tPA have a 30% higher chance of a good outcome at 3 months after the stroke.
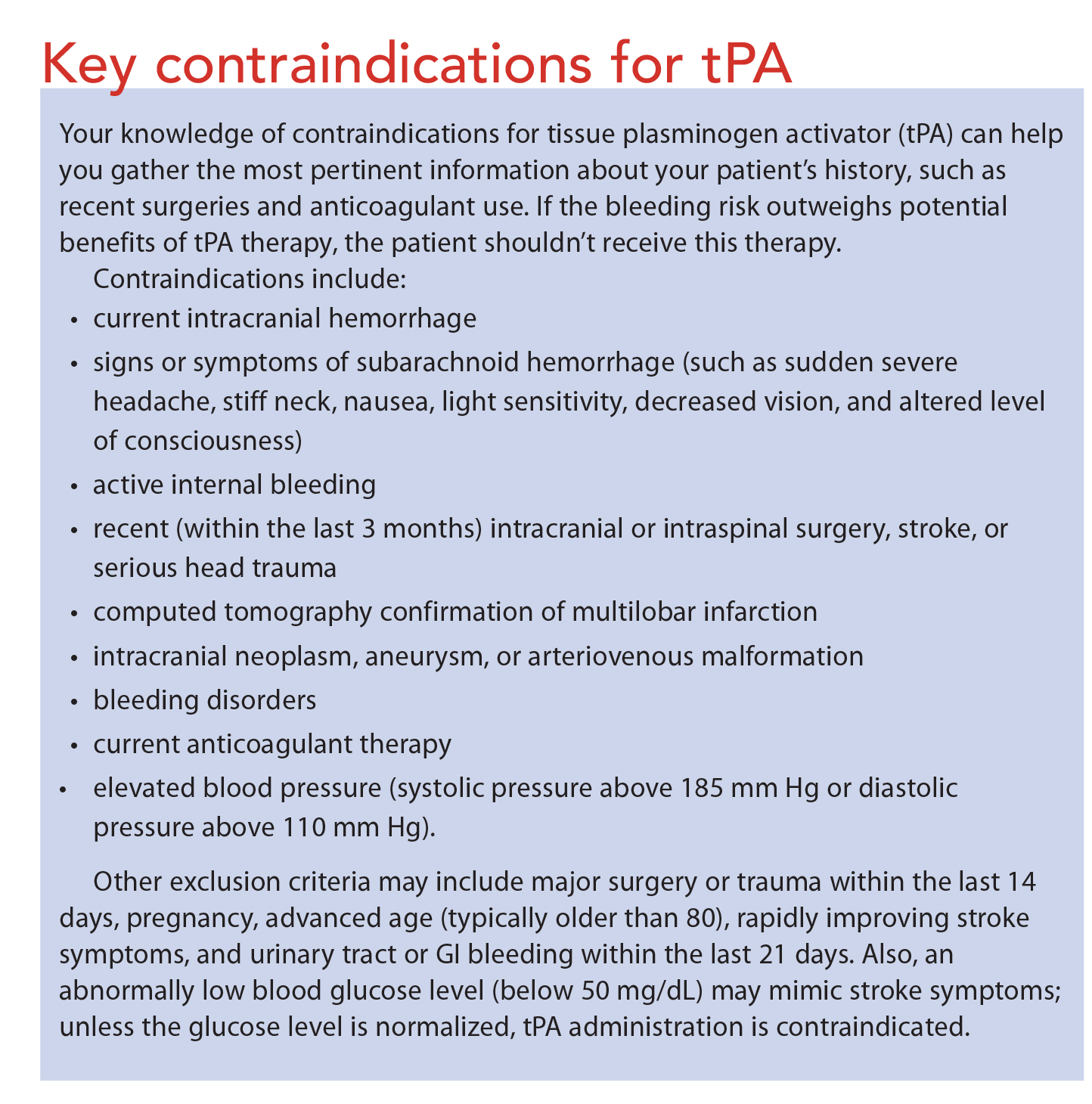
To qualify for tPA, patients must meet strict inclusion criteria; those age 18 or older with a CT-confirmed ischemic stroke may meet these criteria. However, the physician must consider many important exclusion criteria. (See Key contraindications for tPA.)
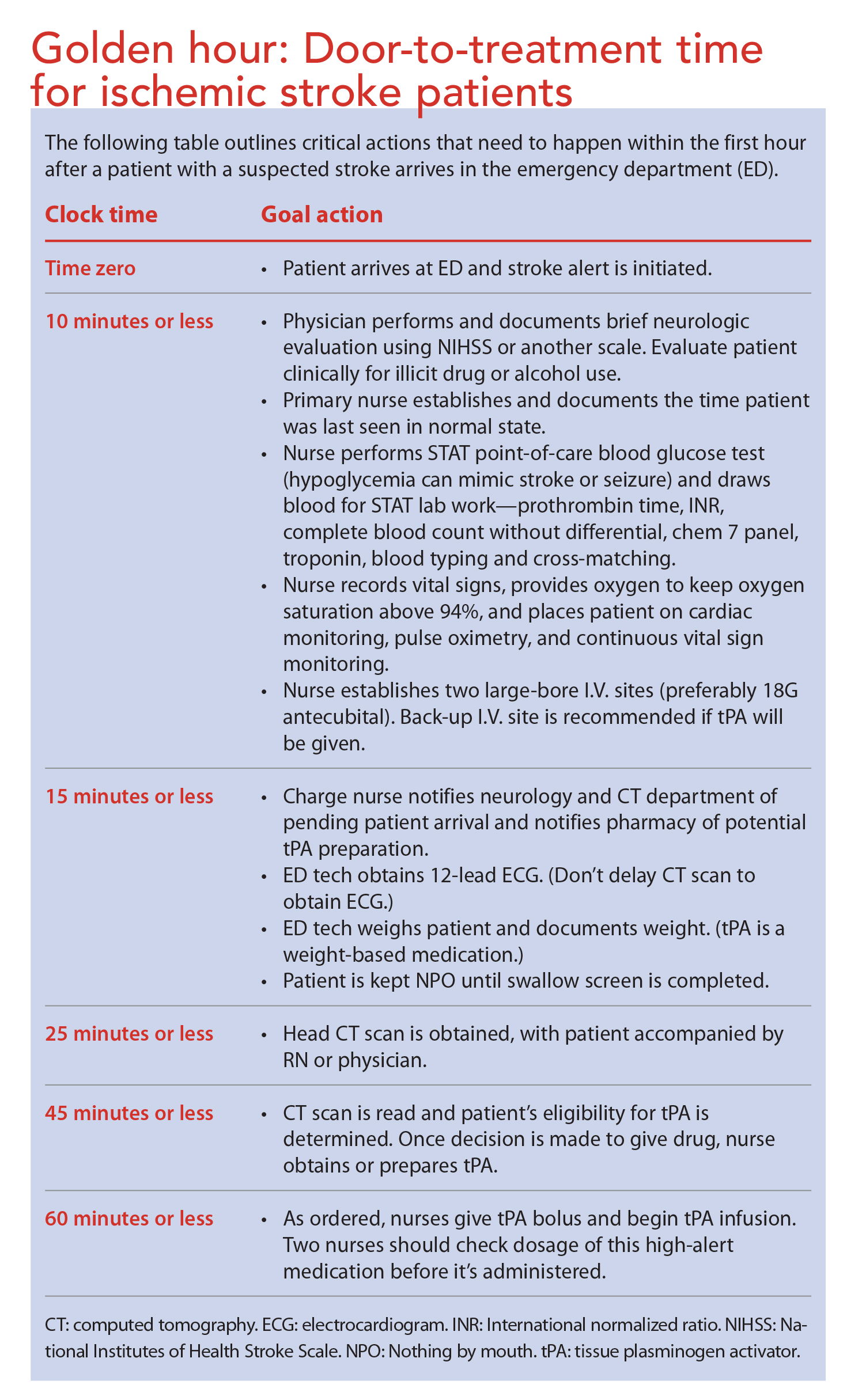
A successful response to tPA requires careful adherence to the administration protocol. This therapy should begin as soon as possible— within 3 hours (or in some cases, 4.5 hours) of symptom onset. If the drug is given beyond this administration window, the risk of intracranial hemorrhage from tPA increases. (See Golden hour: Door-to-treatment time for ischemic stroke patients.)
To help determine your patient’s tPA eligibility, conduct a thorough history and perform an assessment, including vital signs and point-ofcare blood glucose level. If a family member is present, ask this person if he or she knows what time the patient’s symptoms began. Use your assessment time wisely. Keeping tPA exclusion criteria in mind, gather as much pertinent information as possible about the patient’s history.
The decision to initiate tPA treatment must be carefully considered after consultation between the physician and the patient or patient’s spokesperson. The patient or spokesperson must consent to the procedure after being fully advised of risks and benefits. Risks include bleeding in the brain, internal bleeding (other than in the brain), and allergic reactions. The most common allergic reaction is angioedema, which occurs in 1% to 2% of patients. Stay alert for hives and lip or other perioral swelling; notify the physician immediately if these occur.
Critical care monitoring
To evaluate for neurologic deterioration, patients receiving tPA must undergo neurologic assessment every 15 minutes with the NIHSS or mNIHSS (depending on facility protocol) during the 1-hour infusion and the first hour after the infusion ends. Neurologic checks should be repeated every 30 minutes for the next 6 hours and then hourly until 24 hours after the infusion. Expect the physician to order a follow-up CT or magnetic resonance imaging scan at the 24-hour mark.
Continue to monitor and control BP as needed every 15 minutes for the first hour after the infusion ends, every 30 minutes for the next 6 hours, and then hourly from the eighth post-infusion hour until hour 24. Withhold oral intake until a swallow evaluation is completed and documented. Nurses working in stroke centers receive education in performing a bedside swallow screen using a validated tool. The swallow evaluation is a priority for stroke patients, who are at high risk for aspiration pneumonia—a serious complication that accounts for 15% to 20% of stroke-related deaths.
Stent clot retrieval devices for acute ischemic stroke
In addition to tPA, 2015 updated guidelines from the American Heart Association/American Stroke Association endorse use of stent clot retrieval devices (similar to those used to open clogged coronary arteries) for carefully screened patients with acute ischemic largevessel strokes. This endovascular treatment, done by a neurointerventionalist, can greatly reduce the risk of permanent disability.
Stent clot retrievers are fine wire mesh tubes that trap the blood clot and allow it to be pulled from the brain. Done with the patient under sedation or general anesthesia, the procedure resembles cardiac catheterization. It’s offered to patients who’ve received tPA and must be initiated within 6 hours of stroke onset and completed by hour 8.
This procedure has certain risks. Also, only a limited number of comprehensive stroke centers offer it, although the number is increasing. Fortunately, rapid critical care transport to a comprehensive stroke center is a growing reality, even from rural locations. (Note: Primary stroke centers are certified to take care of most patients with ischemic stroke. Comprehensive stroke centers offer care for all types of stroke patients, offering minimally invasive procedures for clot retrieval and neurosurgery for complex procedures, such as brain aneurysm clipping.)
Nursing care: A critical difference for stroke patients
Mr. Sarangelo responds well to two I.V. pushes of 10 mg labetalol to lower his systolic pressure below 185 mm Hg and diastolic pressure below 110 mm Hg. After clinicians determine he’s a good candidate for tPA, he receives the infusion.
Eventually, Mr. Sarangelo recovers fully from his stroke with no residual deficits. A month later, he returns to the stroke center to thank the nursing staff. Luckily for him, his wife recognized the warning signs of a stroke and called 911 right away. Otherwise, he might have been ineligible for the brain-saving thrombolytic therapy he received.
Even if you don’t work in a stroke center, your knowledge of stroke assessment and the timeline for emergent care of ischemic stroke can help minimize the devastating effects of stroke and even save your patient’s life. Teach patients about signs and symptoms of stroke. Provide education on the major modifiable risk factors for stroke and encourage patients to make lifestyle changes to lower their stroke risk. Most importantly, urge them to call 911 if they or a loved one exhibits stroke signs and symptoms.
Dorothy Moore is a staff nurse at Kaiser Permanente Emergency Department, in Oakland, California, and an adjunct lecturer at California State University in Hayward.
Selected references
Broderick JP, Jauch EC, Derdeyn CP. American Stroke Association Stroke Council Update: sea change for stroke and the American Stroke Association. Stroke. 2015;46(6): e145-6.
Centers for Disease Control and Prevention. Stroke Facts. Updated March 24, 2015.
Davis SM, Donnan GA. 4.5 hours: the new time window for tissue plasminogen activator in stroke. Stroke. 2009;40(6):2266-7.
Jauch EC, Saver JL, Adams HP, et al; American Heart Association Stroke Council; Council on Cardiovascular Nursing; Council on Peripheral Vascular Disease; Council on Clinical Cardiology. Guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/ American Stroke Association. Stroke. 2013; 44(3):870-947.
Lansberg MG, Bluhmki E, Thijs VN. Efficacy and safety of tissue plasminogen activator 3 to 4.5 hours after acute ischemic stroke: a metaanalysis. Stroke. 2009;40(7):2438-41.
McDavid JC, Bellamy LM, Thompson CJ. Abstract NS12: Is online NIHSS certification enough training. Stroke. 2015;46(Suppl 1).
Meyer BC, Lyden PD. The modified National Institutes of Health Stroke Scale: its time has come. Int J Stroke. 2009;4(4):267-73.
Powers WJ, Derdeyn CP, Biller J, et al.; on behalf of the American Heart Association Stroke Council. 2015 AHA/ASA Focused Update of the 2013 Guidelines for the Early Management of Patients with Acute Ischemic Stroke Regarding Endovascular Treatment: A Guideline for Healthcare Professionals from the American Heart Association/American Stroke Association. Stroke. 2015;46(10):3020-35.
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
4 Comments.
very useful article, unfortunately some may think this is all it is to stroke. it is important documenting ourselves but sometimes it can come to our detriment not trusting the professionals in charge of the care of our loved ones.
to the comments above: guidance advices critical care monitoring for the first 72 hours within a specialized centre in critical cases, but when there’s not such a thing nearby + ‘Time is Brain’, the ambulance services will direct you to the best choice available. Not every person suffering a stroke will evolve in the same way/pattern, won’t suffer the same disabilities nor need the same intensity of care. PLUS each person has their on risk factors, for ex coagulation defect or HRT are some uncommon ones.
trust the doctors and nurses, they know what they are doing. Being emotionally available and supportive of the loved one who suffered a stroke goes a looong way in their rehab and road to recovery.
I found it interesting that you state that patients who are in post-stroke care need constant critical care monitoring. My brother had a stroke last night and we are looking for a good place to have him stay during recovery. I will keep this in mind and look for an urgent care center that he can go to.
I didn’t know high cholesterol could contribute as a stroke risk factor. One of my mom’s friend who’s relatively young had a stroke a few years ago and it was frustrating to see because she didn’t smoke or have high blood pressure. As my parents get older, I’ll have to watch their cholesterol levels.
Nice piece of information