Astute triage leads to an evidence-based treatment plan
- Traumatic hyphema, primarily caused by recreational injuries, require emergent evaluation to prevent vision loss.
- Patients frequently present with vision loss, eye pain, photophobia, nausea, or vomiting.
Brian Wright*, a 34-year-old man with a history of essential hypertension, is struck in the right temple with a bat during a softball game. Mr. Wright’s teammates drive him to the emergency department (ED) for evaluation. They wait 3 hours to be seen.
History and assessment
Jane*, an experienced ED nurse, completes the triage for Mr. Wright, who says he felt dizzy and nauseous immediately after being hit by the bat. Mr. Wright says he also experienced right eye pain (10/10), photophobia, and blurred vision.
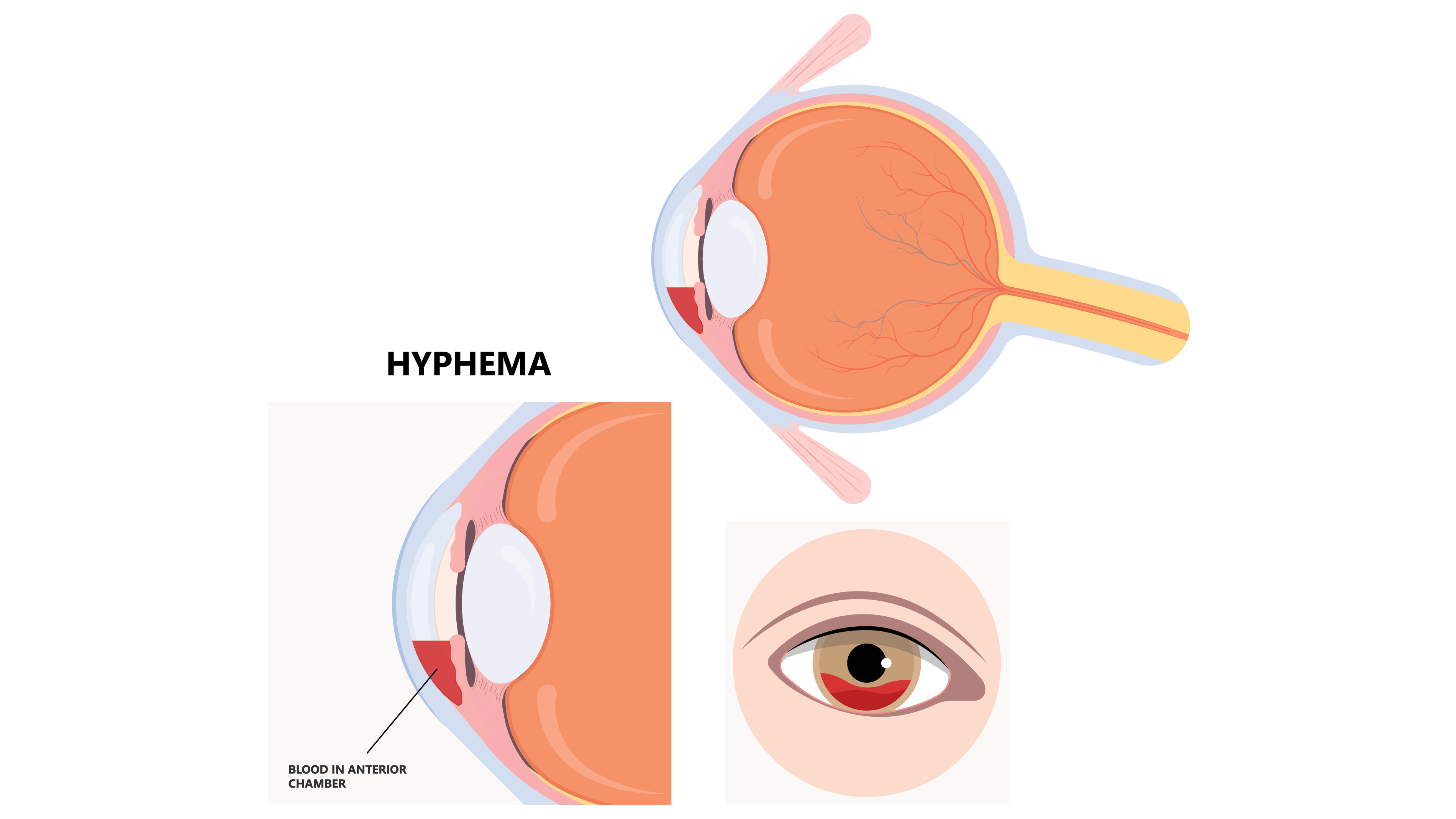
Mr. Wright’s vital signs are temperature 97.5° F (36.4° C), HR 106 BPM, RR 18 breaths per minute, BP 142/78 mmHg, and Sao2 98% on room air. While obtaining Mr. Wright’s vital signs, Jane begins her triage assessment. She notes the presence of blood in the anterior chamber of his right eye and assigns an emergency severity index score of 2 (out of 5) and takes Mr. Wright directly to the trauma treatment area for immediate evaluation.
Taking action
Jane assesses Mr. Wright’s visual acuity (left eye 20/30, right eye 20/200, and both eyes 20/40). Before notifying the attending ED physician about this traumatic injury, Jane elevates the head of the stretcher to 45 degrees, applies a right eye shield, dims the examination room lights, and instructs Mr. Wright to remain on the stretcher.
The ED physician affirms the presence of a hyphema and consults with ophthalmology. She orders an I.V. and 4 mg of morphine sulfate and 4 mg of ondansetron before transporting Mr. Wright for a computed tomography scan of the orbits and maxillofacial bones to rule out fracture and globe rupture.
Outcome
Fortunately, Mr. Wright didn’t sustain any maxillofacial or globe ruptures. He’s evaluated by ophthalmology in the ED with slit-lamp examination of the anterior segment and fluorescein staining. Aside from a Grade II hyphema, the ophthalmologic examination is unremarkable with intraocular pressures 16 mmHg on the left and 19 mmHg on the right.
The ophthalmologist prescribes prednisolone acetate 1% ophthalmic drops four times per day, for 7 days, and oxycodone, 5 mg every 6 hours as needed, for severe pain. Mr. Wright is discharged home with daily outpatient ophthalmology follow-up and instructions to limit strenuous physical activity and to wear his right eye shield at all times.
Education and follow up
Traumatic hyphema is most common in men and children with an incidence of 12/100,000 individuals. Penetrating or blunt ocular trauma, which typically occurs as a result of athletic or recreational injuries, requires emergent evaluation to prevent vision loss. Patients frequently experience vision loss, eye pain, photophobia, nausea, or vomiting. Sickle cell disease, anticoagulant use, and clotting disorders increase complications associated with hyphema. Diagnosis is primarily clinical, although globe rupture must be ruled out.
Traumatic hyphema requires prompt identification and ophthalmology evaluation. Individuals with a Grade II hyphema (less than 50% of the anterior chamber occupied by blood) can be managed as outpatients, with daily ophthalmology evaluations to assess intraocular pressures, administration of ocular glucocorticoids to prevent rebleeding and control inflammation, limited physical activity, and eye shielding. Grade II hyphema typically resolves within 7 days. In Mr. Wright’s case, Jane’s astute triage assessment facilitated timely implementation of an evidence-based treatment plan.
*Names are fictitious.
Aaron M. Sebach is dean of the College of Health Professions and Natural Sciences at Wilmington University, in New Castle, Delaware, and a nurse practitioner at TidalHealth Peninsula Regional, in Salisbury, Maryland.
American Nurse Journal. 2024; 19(1). Doi: 10.51256/ANJ012435
References
Galvis V, Pedraza-Concha A, Tello A, Lina Plata M, Luis Escaf C, Ruben Berrospi D. Clinical features, management and visual outcomes on patients with traumatic hyphema in a reference opthalmological clinic in Colombia. Rom J Opthalmol. 2020;64(1):28-34.
Gharaibeh A, Savage HI, Scherer RW, Goldberg MF, Lindsley K. Medical interventions for traumatic hyphema. Cochrane Database Syst Rev. 2019;1:CD005431. doi:10.1002/14651858.CD005431.pub4
Gragg J, Blair K, Baker MB. Hyphema. StatPearls. December 26, 2022. ncbi.nlm.nih.gov/books/NBK507802
Oldham GW. Hyphema. EyeWiki. October 18, 2023. eyewiki.aao.org/Hyphema
Key words: hyphema, traumatic hyphema, ocular trauma



















2 Comments. Leave new
This is helpful to uplift our knowledge as nurses….specially addressing current trends is essential as most are not in the field and not in thefield of continues professional development ….thanks again
I think she really did the best for the patient