In the late 1990s, public health departments around the globe celebrated the prospect of eradicating syphilis. However, by the early 2000s, this sexually transmitted infection (STI) changed course and climbed over 400% between 2012 and 2022. Now, for the first time in 20 years, the Centers for Disease Control and Prevention (CDC) is reporting a slight improvement in the number of cases. However, the cases being identified are more dangerous: late-stage diagnoses, a shift to persons of reproductive age, and increasing cases of congenital syphilis.
Syphilis: The Great Imitator
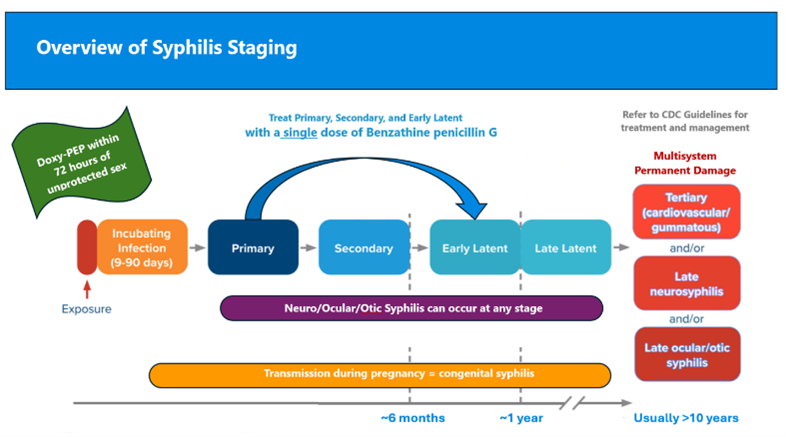
Syphilis is known as the “Great Imitator,” and providers aren’t able to diagnose it by symptoms alone. Screening tests are critical, but some providers don’t include syphilis in routine STI testing. Many patients are only offered syphilis screening after other STIs are identified first.
In the initial stages, syphilis is easily treatable with penicillin. But once the infection progresses, the risk of permanent damage to the heart, brain, eyes, and ears increases. At later stages, antibiotics can kill the infection, but the damage incurred can’t be reversed.
People of reproductive age and congenital syphilis
Before 2020, women, including those of childbearing age, were diagnosed with syphilis less frequently than men. However, 2023 CDC statistics show a single year increase of 8.6% in syphilis diagnoses in women; out of 64,795 women diagnosed, 55,407 were between the ages of 15 and 44. They were diagnosed with syphilis when they might be trying to conceive or were pregnant already.
There’s been a 10-fold increase in the number of congenital syphilis cases over the past decade, with 3,882 cases including 279 congenital syphilis-related stillbirths and neonatal or infant deaths in 2023. Specialty physicians such as neurologists, gastroenterologists, and cardiologists are seeing more patients whose syphilis infections have gone undiagnosed until complications arise. Anecdotally, a 22-year-old male presented to the emergency department with chest pain and a generalized rash. In usual fashion, cardiology was consulted for further evaluation. Eventually, the patient was found to have syphilis and laboratory studies gave evidence of liver and heart involvement. He acknowledged having multiple sex partners and had been tested for some STIs but not syphilis by his primary care provider. The bottom line? Both the patient and the provider didn’t perceive a substantial risk for syphilis.
Doxy-PEP and syphilis prevention
Amid this troubling landscape, a promising prevention tool is gaining attention: Doxy-PEP (doxycycline post-exposure prophylaxis). Doxy-PEP harnesses the power of the antibiotic doxycycline to stop chlamydia, gonorrhea, and syphilis if self-administered within 72 hours of sex. It’s an empowering option for patients and easy for providers to prescribe. This doesn’t replace appropriate screening or condom use, but it does add an extra layer of protection, which could turn the tide in the fight against syphilis.
Where do we go from here?
We’re asking providers to take the lead in educating patients and communities about the need for routine syphilis screening, prevention, and treatment options. The statistics are clear, and the risk is apparent; as nurses, as members of the global community, we can’t afford to put this off any longer.
Julianne Puckett, FNP-BC is a nurse practitioner at Denver Health and Hospital Authority, Denver, Col. and Shy’na Foster, FNP-BC is a cardiology nurse practitioner at Nuvance Health, Poughkeepsie, NY