
There are many causes of medical complexity and technology dependence in children. Traumatic brain injuries are the leading cause of pediatric morbidity, although prematurity, genetic diseases, and other health issues may contribute to the need for assistive health technologies (Agostiniani et al., 2014; Erlick et al., 2021). Over the last two decades, advancements in clinical care and treatments have significantly reduced the mortality of children with complex illnesses, also contributing to an increase in the need for health technologies such as ventilators and feeding pumps (Agostiniani et al., 2014; Cohen et al., 2018). This has changed the landscape of care at home (Acorda et al., 2022).
While there are still more nurses and healthcare professionals who can learn about the experiences of families who have a child with medical technology dependence, we do know that they experience significant challenges (Nakarada-Kordic et al., 2017; Page et al., 2020). The daily family experience changes after a child receives a tracheostomy. After tracheostomy, families must monitor, assess, and interpret their child’s health responses, make clinical decisions, and provide physical and emotional care. Acorda et al. (2022) highlighted the challenges parents encounter, specifically around discharge. During the transition process parents reported high levels of fear, stress, and significantly lower quality of life compared to parents of healthy children (Acorda et al., 2022; Nakarada-Kordic et al., 2017). Additional research has demonstrated opportunities to reduce the burden on families through education, planning, and supportive care (Acorda et al., 2022; Akangire et al., 2020; Fernandes et al., 2023; Nakarada-Kordic et al., 2017; Vo et al., 2023). A significant amount of information and skills must be taught to the family members at such an emotional period in the family’s life. Nurses are uniquely positioned to help families grow in competence and confidence as they teach them the skills necessary to go home safely.
This article will highlight an innovative program implemented at Nemours Children’s Hospital in Delaware to support the challenging transition for parents with a medically complex child needing a tracheostomy.
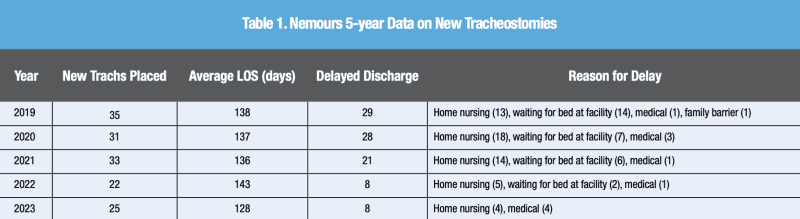
The process of preparing parents to manage a child’s tracheostomy outside the hospital typically takes six to eight weeks to complete. One of the most frequently encountered delays during this time is establishing nursing care in the home, and this process is therefore initiated early. Table 1 outlines data surrounding the volume, length of stay, and potential discharge delays associated with new tracheostomies placed over the last five years (2019-2023).
 At Nemours, each family is assigned a primary care team which includes doctors, social workers, nurses, and a primary respiratory therapist (RT). This team will lead and support the patient and caregivers throughout their training to provide continuity of care. Each family is provided with a training manual and training tracking binder. The primary team rounds daily with the family to discuss the child’s medical care and meets monthly (more frequently if needed) to provide a more in-depth conversational environment for the family to ask questions, voice concerns, and discuss their child’s progress toward discharge.
At Nemours, each family is assigned a primary care team which includes doctors, social workers, nurses, and a primary respiratory therapist (RT). This team will lead and support the patient and caregivers throughout their training to provide continuity of care. Each family is provided with a training manual and training tracking binder. The primary team rounds daily with the family to discuss the child’s medical care and meets monthly (more frequently if needed) to provide a more in-depth conversational environment for the family to ask questions, voice concerns, and discuss their child’s progress toward discharge.
Two adult caregivers must complete training for a ventilator-assisted child. Having two trained caregivers allows ongoing safety and flexibility in the care of the child at home. The training consists of two major components: tracheostomy care and respiratory equipment education. Nurses provide daily tracheostomy education and support, while the primary RT provides education on respiratory equipment. Nurses and RTs work together to ensure all aspects of care are covered, and parent’s questions are addressed. Families are provided formal opportunities to receive education 2-3 times a week and are encouraged to practice their new skills whenever they are at the bedside. As training progresses, the care team works to ensure the caregivers demonstrate competency in the essential care of their child’s airway and technology. Specifically, the care team ensures caregivers can safely suction their child’s airway, change the tracheostomy tube, and perform cardiopulmonary resuscitation (CPR). These learned skills include assessment of the child’s respiratory status and training caregivers to respond to their child’s respiratory needs appropriately. Once all training is complete, caregivers must successfully complete Supervised Family Care (SFC). The SFC is a 24-hour period when the two caregivers assume full care for their child in the hospital room. The SFC provides the opportunity for parents to take full care of their child within the safety of the hospital. Finally, upon discharge, home care nursing is organized through the family’s insurance to reduce the burden on families in the provision of 24-hour care. Optimal home nursing provides 24-hour nursing for the first three weeks, transitioning to 16 hours per day after that, but this can depend on the insurance coverage of each family.
Research has shown that it is imperative that nurses listen to caregiver’s input and concerns with regard to their child’s care during this time (Acorda et al., 2022). Families gain strength when nurses recognize, acknowledge, and appreciate that their lives will never go back to the way it was before (Acorda et al., 2022; Nakarada-Kordic et al., 2017; Rennick et al., 2019). As caregivers adjust to a ‘new normal,’ nurses need to understand parents’ emotional state and guide their teaching accordingly. This does not mean going slowly but guiding the parents with patience and instilling confidence. Working as a team and providing complimentary and consistent teaching are instrumental in preparing the patient and family to transition from the hospital to their home.
References
Acorda, D. E., Jackson, A., Lam, A. K., & Molchen, W. (2022). Overwhelmed to ownership: The lived experience of parents learning to become caregivers of children with tracheostomies. Int J Pediatr Otorhinolaryngol, 163, 111364. https://doi.org/10.1016/j.ijporl.2022.111364
Agostiniani, R., Nanni, L., & Langiano, T. (2014). Children with medical complexity: the change in the pediatric epidemiology. Journal of Pediatric and Neonatal Individualized Medicine (JPNIM), 3(2), e030230. https://doi.org/10.7363/030230
Akangire, G., Taylor, J. B., McAnany, S., Noel-MacDonnell, J., Lachica, C., Sampath, V., & Manimtim, W. (2020). Respiratory, growth, and survival outcomes of infants with tracheostomy and ventilator dependence. Pediatric Research, 90(2), 381-389. https://doi.org/10.1038/s41390-020-01183-x
Cohen, E., Berry, J. G., Sanders, L., Schor, E. L., & Wise, P. H. (2018). Status Complexicus? The Emergence of Pediatric Complex Care. Pediatrics, 141(Supplement_3), S202-S211. https://doi.org/10.1542/peds.2017-1284E
Erlick, M. R., Vavilala, M. S., Jaffe, K. M., Blayney, C. B., & Moore, M. (2021). Provider perspectives on early psychosocial interventions after pediatric severe traumatic braininjury: An implementation framework. J Neurotrauma, 38(4), 513-518. https://doi.org/10.1089/neu.2020.7323
Fernandes, M., Rathinam, C., & Topping, A. E. (2023). Parents’ experience of children with acquired brain injury undergoing neuro-rehabilitation: thematic synthesis protocol. BMJ Open, 13(4). https://doi.org/10.1136/bmjopen-2022-066254
Nakarada-Kordic, I., Patterson, N., Wrapson, J., & Reay, S. D. (2017). A systematic review of patient and caregiver experiences with a tracheostomy. The Patient. 11(2), 175-191. https://doi.org/10.1007/s40271-017-0277-1
Page, B. F., Hinton, L., Harrop, E., & Vincent, C. (2020). The challenges of caring for children who require complex medical care at home: ‘The go between for everyone is the parent and as the parent that’s an awful lot of responsibility’. Health Expectations, 23(5), 1144-1154. https://pubmed.ncbi.nlm.nih.gov/32542954/
Rennick, J. E., St-Sauveur, I., Knox, A. M., & Ruddy, M. (2019). Exploring the experiences of parent caregivers of children with chronic medical complexity during pediatric intensive care unit hospitalization: an interpretive descriptive study. BMC Pediatrics, 19(1). https://doi.org/10.1186/s12887-019-1634-0
Vo, H. H., Wilfond, B. S., Vo, H. H., Mercer, A. H., Wilfond, B. S., Jabre, N. A., Henderson, C. M., Henderson, C. M., Boss, R. D., & Boss, R. D. (2023). Parent perspectives on the child experience of pediatric home ventilation via tracheostomy. Hospital Pediatrics, 13(12), 1124-1133. https://doi.org/10.1542/hpeds.2023-007217





















