
Empowered professionals enhance patient safety.
Pressure injuries (PIs) occur in 3% to 34% of hospitalized patients worldwide and result in increased length of stay, morbidity, and human suffering. PIs can range from erythema on the surface of the skin to deep, complex wounds that extend beyond the skin surface to underlying tissue.
Ten percent of all PIs are device related. The National Pressure Ulcer Advisory Panel (NPUAP) defines device-related injuries as those “that result from the use of a device designed and applied for diagnostic or therapeutic purposes.” Device-related PIs are especially challenging for nurses because device need is often in direct competition with nursing care plans that include preventing pressure-related skin injury.
Patients who require noninvasive ventilation (NIV) for acute and chronic impaired gas exchange are at risk for device-related PIs to the face. Risk factors are secondary to continuous mask and strap pressure, friction and shear injury from mask movement, and fragile skin caused by chronic steroid use in respiratory illnesses. Delmore and Ayello found that 51% of device-related PIs occurred on the face, head, or neck.
A 1,018-bed academic hospital with Magnet® recognition reduced hospital-acquired PIs (HAPIs) associated with NIV oxygen masks with the implementation of a protocol and algorithm created by an interprofessional team.
Problem identified
Despite the hospital’s efforts to prevent PIs, 41 NIV-related HAPIs occurred between July 2014 and September 2016. Nursing care to prevent these injuries was consistent with evidence-based, standard practices, including skin care, nutrition, and foam dressings on the skin surface beneath the mask. However, NIV management practices were inconsistent, fragmented, and without clear parameters for NIV weaning and liberation endpoints.
Interventions implemented
In 2016, an interprofessional work group (including clinical nurses, respiratory therapists, providers, a nurse wound specialist, nurse managers, and educators) was formed to develop a clinical management protocol that included a systematic approach to NIV management with defined clinical endpoints. The group met every other week and began their work by looking at the evidence and completing a root cause analysis of NIV-related HAPIs within the organization.
Evidence review
The evidence review revealed three key elements for consideration: protocol use, protective skin barrier application, and alternating nasal-oral face mask/full-face mask use.
In a study by Khilnani and Jain, weaning governed by a protocol resulted in a 1.8-day reduction in the time patients received NIV and decreased intensive care unit length of stay by 2.3 days. Less time receiving NIV decreases exposure to mask pressure and PI risk. Reduced NIV use also is associated with decreased costs and risks of other hospital-acquired conditions, such as infections.
Skin barriers must be easy to remove and reapply to allow for skin inspection and assessment. The NPUAP 2014 international guidelines recommend inspecting skin under the medical devices at least twice daily. If edema is present, assessment frequency should be increased.
Compared to a nasal-oral mask, a full-face mask redistributes pressure over a larger skin surface area, decreasing PI risk. In a study by Schallom and colleagues, 20% of patients who wore a nasal-oral mask developed PIs, compared to 2% of patients with a full-face mask. In addition, the time to PI development for a nasal-oral mask was 28.4 hours versus 61.37 hours for a full-face mask. These findings prompted the investigators to recommend alternating between a nasal-oral mask and a full-face mask for NIV.
Root cause analysis
Simultaneous to the evidence review, work group members examined findings from root cause analyses completed by the organization’s interprofessional peer review committee. Of significance was failure to have well-defined NIV clinical endpoints, leading to inconsistent management by nurses and respiratory therapists. These bedside clinicians were unsure when to wean or terminate therapy, resulting in prolonged use.
Root cause analyses also found that the skin barrier being used wasn’t specifically designed for NIV application; it wasn’t easy to apply, and it didn’t remain in place. The NIV mask was difficult to fit and remove and the facial cushion seal had rigid edges. In addition, the NIV titration parameter wasn’t standardized, leading to parameter delay for care de-escalation and escalation.
NIV protocol development
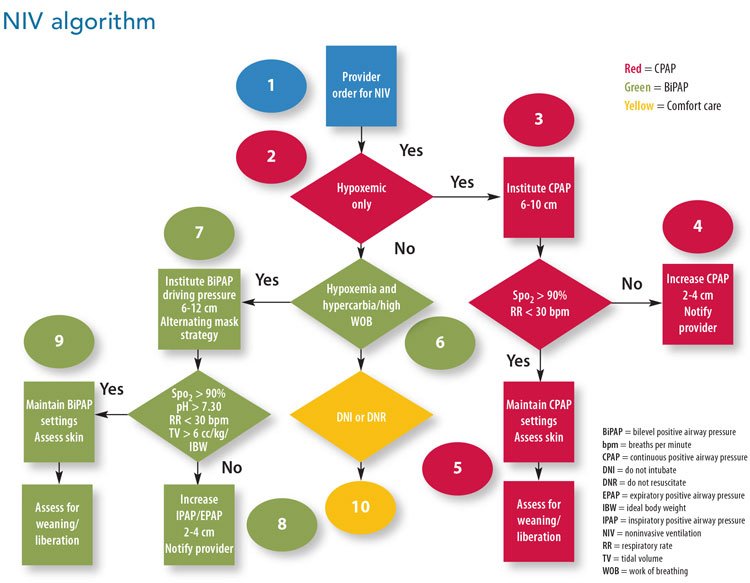
The evidence, root cause analysis, and expert clinical knowledge of interprofessional team members drove development of a new protocol that includes five key items: therapy initiation and weaning guidelines, termination endpoints, a new mask, skin assessment, and an enhanced skin barrier. The team developed an algorithm that outlines a sequential process for NIV escalation and weaning. (See NIV algorithm.) In addition to the algorithm, the protocol also includes when NIV therapy should be terminated secondary to clinical stabilization and target endpoints for peripheral oxygen saturation (SpO2), respiratory and heart rates, and arterial pH.
(Visit American Nurse Today to view the full NIV protocol.)
A “hard stop” was placed in the electronic health record (EHR) order set that requires providers to define target endpoints before initiating NIV. The algorithm allows nurses and respiratory therapists to autonomously adjust therapy within the identified parameters.
Several masks were trialed and evaluated to find one that’s easy to apply and remove and that reduces skin shear forces. The selected mask is made of silicone, is easy to apply, and reduces skin pressure. In accordance with the NPUAP guidelines, an alternating mask is used to further minimize continuous skin pressure. Every 4 hours, the full-face mask is alternated with the new nasal-oral mask; the mask position is changed every 2 hours. Skin assessments occur with mask and position changes.
Because the current skin barrier wasn’t designed for use with an NIV mask, a new gel-based skin barrier specifically intended to be placed under the NIV mask was introduced.
Education
A mandatory electronic self-directed educational learning module was developed for all providers, clinical nurses, and respiratory therapists who care for patients receiving NIV. Content includes a description of the NIV protocol, mask types and use, skin barrier gel application, and documentation requirements. (The module is now part of orientation for nurses and respiratory therapists.) In addition, the nurse and respiratory therapy clinical educators provided hands-on training for the new mask and skin barrier product.
When the protocol was first implemented, a report of all patients receiving NIV was generated each morning from the EHR; daily rounds to these patients were completed by the nurse and respiratory therapist educators. The intent was to ensure that the protocol was being used and implemented correctly and to allow staff to ask questions. Staff also demonstrated mask and skin barrier application.
Outcomes assessed
Clinicians who identify a PI document it in an electronic patient safety report. Education about the new NIV protocol occurred during September 2016, with formal implementation October 1, 2016. Since that time, two NIV-related injuries have been recorded, the first during the first month after implementation.
Nursing practice implications
Developing and implementing a protocol to prevent PIs during NIV reinforced to all interprofessional staff, but especially bedside clinicians, the importance of using evidence, root cause analysis, and expert clinical knowledge to drive practice improvements. This effort also demonstrated the value of data transparency to advance clinical practice. Having the data available and as close-to-possible real-time review allowed the work group to identify the problem and confirm that the interventions successfully addressed it.
Interprofessional collaboration, including bedside clinicians, was essential to this effort’s success. Each discipline involved in NIV participated in defining the problem and associated improvement strategies. Including an algorithm for clinical nurses and respiratory therapists to autonomously adjust NIV within identified parameters empowers these professionals to work within their full scope of practice to achieve the Magnet model component of exemplary professional practice.
The authors work at Lehigh Valley Health Network in Allentown, Pennsylvania. Lucy Cascioli and Stacy Davis are patient care specialists, Kenneth Miller is an educator, and Munawer Kermalli is a quality analyst.
Selected References
Black J, Alves P, Brindle CT, et al. Use of wound dressings to enhance prevention of pressure ulcers caused by medical devices. Int Wound J. 2015;12(3):322-7.
Delmore BA, Ayello EA. Pressure injuries caused by medical devices and other objects: A clinical update. Am J Nurs. 2017;117(12):36-45.
Kayser, SA, VanGilder CA, Ayello EA, Lachenbruch C. Prevalence and analysis of medical device-related pressure injuries: Results from the International Pressure Ulcer Prevalence Survey. Adv Skin Wound Care. 2018;31(6):276-85.
Khilnani GC, Jain N. Do we need a protocol for weaning patients from noninvasive ventilation? Indian J Crit Care Med. 2014;18(12):775-7.
National Pressure Ulcer Advisory Panel, European Pressure Ulcer Advisory Panel, Pan Pacific Pressure Injury Alliance. Prevention and Treatment of Pressure Ulcers: Quick Reference Guide. 2014. internationalguideline.com/static/pdfs/NPUAP-EPUAP-PPPIA-PUQuickReferenceGuide-2016update.pdf
Schallom M, Cracchiolo L, Falker A, et al. Pressure ulcer incidence in patients wearing nasal-oral versus full-face noninvasive ventilation masks. Am J Crit Care. 2015;24(4):349-56.

















