

Think Tank offers detailed strategies with short-term implementation timelines
Nurse staffing challenges remain one of the defining issues of the COVID-19 pandemic. However, many factors contributing to these challenges were bedeviling the healthcare system well beforehand. With the pandemic amping up old problems and surfacing new ones, Partners for Nurse Staffing—a consortium of five major organizations including the American Nurses Association (ANA)—convened a Nurse Staffing Think Tank. In May 2022, this body of experts produced a significant work product, which identifies practical approaches for dealing with today’s staffing woes.
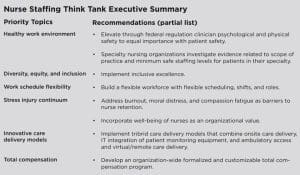
The Think Tank issued a list of priority topics and actionable strategies that healthcare organizations and other stakeholders can implement within 12 to 18 months. The 26-page document provides detailed definitions, measurable outcomes, action steps, and supporting research for each of six drivers in the nurse staffing debate, including healthy work environment, diversity, equity and inclusion, work schedule flexibility, stress injury continuum, innovative care delivery models, and total compensation (See Executive Summary).
Full report available at https://bit.ly/3R2z4gT.
 For example, the Think Tank defined work schedule flexibility as an approach that encompasses accommodation in work options, policies, and schedules, with nurses cross-trained to various units. The goal is to support nurse well-being and incorporate time for professional development and leadership engagement such as shared governance. Recommended actions include establishing single entity or multihospital system float pools, creating seasonal or surge float pools, and developing interdisciplinary care teams to complete shift-based tasks like admissions and discharges.
For example, the Think Tank defined work schedule flexibility as an approach that encompasses accommodation in work options, policies, and schedules, with nurses cross-trained to various units. The goal is to support nurse well-being and incorporate time for professional development and leadership engagement such as shared governance. Recommended actions include establishing single entity or multihospital system float pools, creating seasonal or surge float pools, and developing interdisciplinary care teams to complete shift-based tasks like admissions and discharges.
Setting up a system of work schedule flexibility could enhance patient care quality and safety and staff satisfaction while containing costs. Nursing, finance, and human resources representatives as well as leaders at an organization would be accountable for this approach, which could be established within 6 to 12 months depending on how many entities are involved. The effect of these changes could be measured via outcomes such as frontline employee engagement, patient experiences, and reductions in agency overtime and vacancy and turnover rates.
A turning point

Taken as a whole, the Think Tank recommendations might be a turning point for the nursing profession and U.S. healthcare system, comparable to 2000’s To Err is Human report, which brought significant attention to medical errors and sparked a revolution in patient safety, according to Think Tank member Sherry B. Perkins, PhD, RN, FAAN, president of Luminis Health Anne Arundel Medical Center, an American Nurses Credentialing Center Magnet®-recognized organization in Annapolis, Maryland. “I was a young leader [at that time] and I was so inspired for our industry and how [the report] really began to change our collective thinking about what patient safety was. It was bold,” she recalled. “We can do that on this topic of safe staffing. We can be bold. We can redefine what it means to have safe acute care staffing in U.S. hospitals. This can be that moment.”

Perkins isn’t alone in her assessment of the potential impact of the Think Tank’s recommendations. “Staffing is this huge albatross that we haven’t been able to fix up to this point and it feels like this work is starting to move the needle toward meaningful change,” said Think Tank member Kiersten Henry, DNP, ACNP-BC, CCNS, CCRN-CMC, chief advanced practice clinician and a nurse practitioner in critical care at MedStar Montgomery Medical Center in Olney, Maryland. Both Henry and Perkins are Maryland Nurses Association members.
Diverse perspectives
What makes this effort different and more impactful than other tilts at the nurse staffing windmill is the broad, cross-professions perspective and consensus captured in the document, according to Think Tank participants. The 19 members of the group hail from California, New York, and points in between. They also represent a wide range of positions with an interest in improving nurse staffing. At least four practice frontline nursing, while five others have expertise in fields such as scheduling and predictive modeling, professional development, human resources, and workforce issues. A travel nurse served on the Think Tank, as did a staffing agency executive. Senior healthcare executives also participated, along with a patient advocate, a quality and safety specialist, and a school of nursing dean. All of these perspectives came to bear in six focused meetings concentrated over 3 months. With the guidance of an expert facilitator, the Think Tank expediently developed consensus on the six priority topics and fleshed out the supporting details for each.

“We had this group of highly motivated people of all different backgrounds, which really brought the diversity of thought to the table,” recalled Melinda S. Hancock, CPA, senior vice president and chief administrative officer for Sentara Healthcare in Norfolk, Virginia, which operates nine hospitals that have achieved Magnet Recognition Program®designation. “This was such an important group to come together because everyone’s grappling with staffing. The Think Tank was an opportunity to start tackling this as an industry instead of everybody trying to figure it out on their own.”
Thank Tank members—Hancock included—whole-heartedly embraced the charge to identify solutions that stakeholders could implement in the near term, within 18 months at the extreme. If some actions might take longer—like the suggestion for the Centers for Medicare and Medicaid Services to implement a Condition of Participation about the health of the work environment—momentum now toward those goals matters.
 “In being bold [with our ideas] we realized we wouldn’t be able to check the boxes on some things in 18 months. But it was important to start those conversations because it could take another 2 to 3 years to enact something,” Hancock said.
“In being bold [with our ideas] we realized we wouldn’t be able to check the boxes on some things in 18 months. But it was important to start those conversations because it could take another 2 to 3 years to enact something,” Hancock said.
In addition to ANA, Partners for Nurse Staffing includes the American Association of Critical-Care Nurses, American Organization for Nursing Leadership, Healthcare Financial Management Association, and Institute for Healthcare Improvement.
In May, the consortium also launched a Nurse Staffing Task Force to tackle longer-term and structural issues that contribute to staffing challenges. This group will continue meeting through the balance of 2022 (nursingworld.org/practice-policy/nurse-staffing/nurse-staffing-task-force).
Emphasis on practical

If a few Think Tank recommendations have a more distant implementation timeline, most offer specific, practical steps that stakeholders could deploy within 18 months or sooner. For example, under Total Compensation, the Think Tank suggested a 6-month timeline for instituting compensation-added value intangibles for nurses. One intangible involves creating a system for rewarding nurses who maintain a direct care role, making it attractive for nurses in nonclinical skilled departments to provide direct care with appropriate compensation. Another entails reinstating maintaining, and implementing meaningful pay policies to support nurses for precepting, mentoring, and clinical advancement.
Given the extremis of the staffing situation nationally, Think Tank member Carol Boston-Fleischhauer, JD, MS, BSN, suggested the onus would be on healthcare leaders to demonstrate why their organizations shouldn’t implement recommended strategies. “For chief nurse executives faced with such severe shortages, the bigger challenge is determining sequence and resources needed for implementation,” she said. “For example, why wouldn’t I design flexible schedules for RNs looking for that option? I understand it would require changes in operational processes and potentially play havoc with our automated scheduling system, but we can’t use degree of difficulty as a reason to not consider any staffing solution.”
 Boston-Fleischhauer, chief nursing officer and managing director at the Advisory Board, a market analysis and strategic guidance consultancy in Washington, DC, added that the Think Tank’s emphasis on bold ideas married with action mirrors the outlook of senior executives across the country. “I’m seeing a lot of healthcare leaders collaborating with other stakeholders and being aggressive in terms of state, regional, and national advocacy,” she observed. “This call to action may be louder than ever before but we can’t sit tight for another 3 years and try to figure out this different kind of shortage that requires different kinds of solutions.”
Boston-Fleischhauer, chief nursing officer and managing director at the Advisory Board, a market analysis and strategic guidance consultancy in Washington, DC, added that the Think Tank’s emphasis on bold ideas married with action mirrors the outlook of senior executives across the country. “I’m seeing a lot of healthcare leaders collaborating with other stakeholders and being aggressive in terms of state, regional, and national advocacy,” she observed. “This call to action may be louder than ever before but we can’t sit tight for another 3 years and try to figure out this different kind of shortage that requires different kinds of solutions.”
Involving frontline nurses
Think Tank members were quick to emphasize that their recommendations also offer opportunities for frontline nurses to effect change. “This work gives hope to nurses at the bedside that there are people advocating for a change in the workplace,” Henry said. “For the nurse at the bedside, it’s a pathway towards a better future state as compared to what we’ve been dealing with for decades, but even more over the past couple of years.”
She suggested that staff nurses could play a role in disseminating the recommendations and in using them to reset their organizations’ staffing solutions. “The healthy work environment is a standard that can be socialized to say, here’s what’s been established by this work group of key stakeholders and here are actionable items that we can undertake,” Henry elaborated.
The Think Tank’s concept of a healthy work environment contemplates both physical and psychological safety, and among other outcomes encourages health systems to collect unit-level data on safety, using these data to drive needed change.
Boston-Fleischhauer also underscored that the Think Tank’s recommendations speak to both frontline nurses as well as healthcare executives and other stakeholders. “Our recommendations are not for leaders to work on in isolation of the staff in their organizations. It has to be a collaborative venture,” she said. “Registered nurses know the work of nursing more than anyone else, and now, more than ever, their voices have to be heard. The mandate for leaders to partner with frontline RNs in developing timely and meaningful solutions is essential.”
—Genna Rollinsis writer/editor at ANA












2 Comments. Leave new
There are some great ideas in this report, but there are some critical pieces missing.
We need data, tools, and education for leaders on how to more effectively manage our available workforce. Having a staffing & scheduling system doesn’t necessarily mean that you’re getting this information or have the right tools.
We also have an issue with a flawed nursing budget process being used by many facilities that produces a 2-4% shortfall in the expected FTEs and increases the risk of understaffing. Some of the organizations involved with this report are promoting/teaching this flawed methodology to nurse managers.
I’ve confirmed that one of the largest health systems in the US is using this budget process. As a result of the flawed calculation, they need hundreds more nurses than they realize in order to meet their budget assumptions.
We need a more holistic view of the nursing budget process and a greater understanding of the importance of replacement/non-productive time and how it supports nursing care delivery, the mental health of our caregivers (via time off), and the education needed to ensure the competency of our workforce.
Interesting article. One of the points made was diversity, yet the three profiles highlighted in this article did not include a person of color or a man. If our profession wants to grow and recruit it’s important that the leaders featured are a representation of the message being promoted. I have been a nurse for 30 years and I keep seeing the “same faces” that are nurse leaders. The old adage is true, “sometimes it’s not the message, but the messager.”