
Evaluating adherence in pediatric units
- Using dose error reduction software (DERS) when programming I.V. medications into smart infusion pumps can help reduce errors and patient safety risks.
- Nurse continue to face challenges adhering to DERS use.
- This quality improvement project used manual audits and tailored education to increase adherence with programming important information into smart infusion pumps.
The Institute for Safe Medication Practices (ISMP) emphasizes the importance of using smart infusion pumps with DERS for patient safety. Schnock and colleagues found that 10% of medication administration errors result when nurses use DERS inappropriately and override its safeguards. To reduce the risk of avoidable medication errors, DERS provides preset limits on medication dosage and rates appropriate for specific clinical contexts and patient populations (for example, neonatal ICU or medical/surgical unit).
Understanding infusion pump technology
Smart pumps, smart management, safe patients
Smart infusion pumps with DERS have been on the market for 15 years, and most U.S. hospitals have them; however, medication errors that can potentially cause patient harm persist because of low adherence among nurses. To improve documentation and safety parameters, many healthcare systems have smart infusion pumps that communicate with the electronic health record. To further improve safety, nurses can program the patient’s medical record number (MRN) into the pump. This step helps leaders within the hospital investigate safety events related to the infusion pump.
Pediatric patients face particular risk for poor outcomes associated with infusion errors, as many medications require administration based on weight. Reducing this risk requires that nurses use DERS appropriately.
In our hospital, DERS adherence and MRN programming ranged from 59% to 73% among eight pediatric units; the hospital had set a goal of 95%. The Joint Commission recommends a systems approach to overcome barriers to proper DERS technology use. To improve adherence and decrease patient safety risks, we conducted a quality improvement (QI) project.
Learning more
Although the literature supports the use of smart infusion pumps with DERS technology to reduce the risk of medication errors, nonadherence among nurses continues. Reasons include lack of interoperability of DERS medication libraries (unavailability of certain medications in the library or difficulty finding them) and alert/alarm fatigue (high exposure to alerts/alarms results in desensitization and delayed responses).
Schnock and colleagues found that nurses didn’t use DERS for 8% of administered medications; most were maintenance fluids and no harm was acknowledged. Although many may find this omission acceptable in some clinical contexts, DERS technology use is recommended for all I.V. infusions to improve patient safety. In a retrospective review by Shah and colleagues, one community hospital successfully increased DERS adherence from 3% to 98% over 3 years through education, compliance auditing, and drug library refinement.
Dunford and colleagues found that overrides and workarounds with smart infusion pumps occurred due to poor perceptions of smart pumps among nurses. These perceptions frequently result from organizational culture. Retrospective data from a study by Lehr and colleagues revealed that nurses bypassed DERS for secondary infusions 34% of the time because they perceived these infusions to be low risk for error and the infusion limits too restrictive. In addition, nurses felt that bypassing DERS would minimize alert fatigue, which indicated a knowledge deficit regarding the importance and purpose of the technology. Understanding nurses’ knowledge, practices, and perceptions of DERS technology can help tailor educational interventions.
Designing the project
Our QI project aimed to increase DERS adherence within an eight-unit pediatric division at a large academic health system over 15 weeks. Specifically, we wanted to increase nurse adherence with DERS technology and evaluate medication overrides, increase nurse adherence with programming patient MRNs into smart infusion pumps, and evaluate nurses’ knowledge, practices, and perceptions regarding DERS use.
We used a pre/post-intervention design for this project. Collectively, the pediatric division has 176 beds and cares for complex patients. This QI project included approximately 630 direct care RNs. The healthcare system’s institutional review board deemed the project as exempt (not human subjects research).
Implementing the intervention
As part of a larger hospital-wide effort to evaluate DERS use, we sent an anonymous online survey to all hospital nurses via email in March 2022. We extracted survey responses from those working on pediatric units; we used only pre-survey data from these nurses in our analysis.
This survey included 11 questions related to the nurses’ knowledge, practices, and perceptions of DERS technology, which served as baseline data for our project. In April 2023, we distributed the same survey (via email) after the intervention to nurses in all pediatric units. To help increase survey completion, we also distributed QR codes to the survey.
Over 6 weeks, after the pre-survey, we collected baseline data on pediatric division nurse adherence to DERS use and medication overrides, as well as their adherence with programming patient MRNs. We then audited a random sample of five to ten patients on each unit each week.
The project intervention, which began after collecting baseline data, included bi-weekly educational rounding and flyers. Rounding consisted of short verbal reminders of DERS functionality, explanations of the importance of using the technology to decrease medication error risk, and discussions of the health system’s smart infusion pump policy and how to find it on the intranet. We posted an educational flyer with similar information in nurses’ break rooms. After the intervention, over the course of 9 weeks, we collected post-intervention data.
Analyzing the data
Using manual audits, we retrieved data related to adherence with DERS use and MRN programming and analyzed it using descriptive statistics and run charts. We analyzed run charts using standard quality improvement methods presented by the Institute for Healthcare Improvement, with improvements noted as a shift (six or more data points above the median) or a trend (five or more data points all going in the same direction). The survey questions had a mix of 4-point Likert scale ratings (1=never to 4=always; 1=strongly disagree to 4=strongly agree). We evaluated nurses’ knowledge, practices, and perceptions of DERS via pre/post-intervention surveys, independent t-tests (for Likert scale ratings) or chi-square tests (for categorical variables), and descriptive statistics.
Results
After completing 1,259 audits (428 pre-intervention and 831 post-intervention) on the pediatric units, we found high DERS adherence before the intervention (mean=99.1%) and an increase to 100% after the intervention. All DERS manual overrides related to exceeding the established high-dose limitation for bumetanide. (See MRN adherence.)
MRN adherence
Adherence with entering the patient’s medical record number (MRN) into the smart infusion pump on pediatric units increased over the course of the quality improvement project.
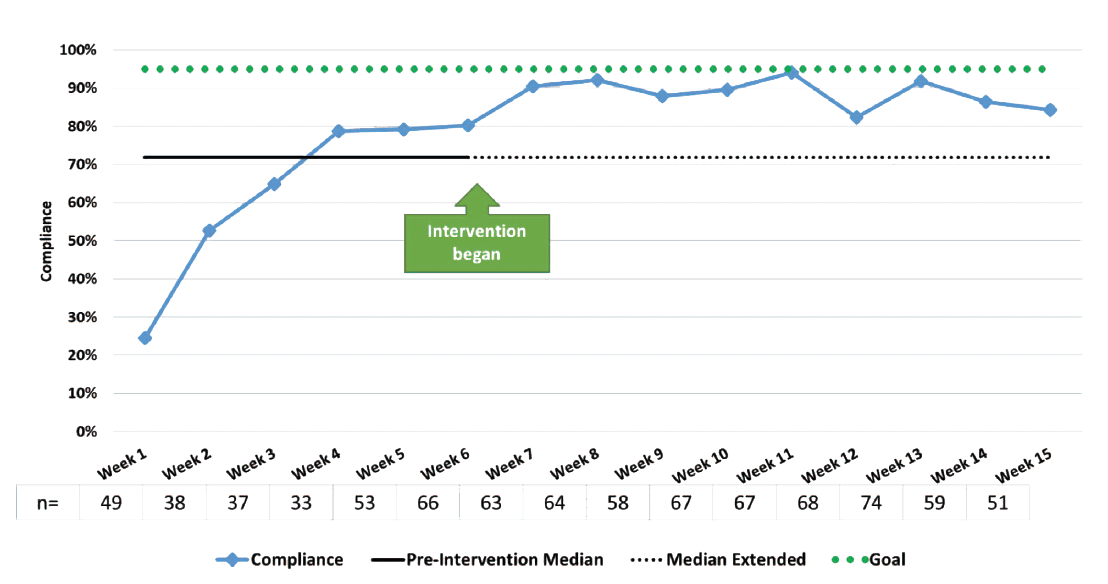
We completed 847 audits to assess adherence with programming patient MRNs into the smart infusion pump (276 pre-intervention and 571 post-intervention). Pre-intervention, median adherence was 71.83% with an increase to 89.55% over 9 weeks post-intervention. Per standard run chart rules, we found signals of improvement in nurses’ adherence with entering MRNs with all data points above the median after the intervention. With regard to pre- and post-survey results, improvement occurred across several items; however, these findings weren’t statistically significant. (See Survey results.)
Survey results
The QI project survey results noted improvement across various items related to the use of smart infusion pump dose-error-reduction software (DERS); however, they’re not statistically significant.
Note. +Independent samples t-tests; aScale: 1=Never to 4=Always; bScale: 1=Strongly disagree to 4=Strongly agree; cScale: 1=Never to 4=Always; *Chi square tests
Understanding the results
Although low DERS adherence served as the impetus for this QI project, we found high adherence pre-intervention. This may have resulted from awareness of the upcoming project. In addition, analyses of pre- and post-intervention surveys showed statistically insignificant improvement in nurses’ knowledge, practices, and perceptions. Although the metrics yielded productive and conclusive adherence, the project underscores maintenance priorities.
To help sustain adherence, we recommend an interprofessional team (including pharmacists, nurses, and physicians) review of the smart infusion pump and medications in the DERS library and at least a biannual update. Consistent adherence can prove challenging; however, several strategies can help. For example, a continuous collaborative process can keep drug doses and concentrations current. In the case of the bumetanide overrides, the soft max limit was set at 0.035mg/kg/hr. Of the 474 alerts during the first quarter of 2023, 98% were for a value of 0.04mg/kg/hr. Hospital pharmacy leadership reviewed this dose and found it clinically appropriate. As a result, the soft max limit was increased to 0.04mg/kg/hr, which eliminated 98% of the bumetanide alerts.
Prior studies have shown that infusion pump technology education and training can improve adherence. Healthcare systems may consider including smart infusion pump DERS technology professional development sessions during annual nurse competencies to include teach-back and attestation for the use of all DERS medications.
In addition, if issues or concerns arise, leadership should instruct nurses to complete a safety incident report within internal error reporting systems. Booth and colleagues noted that these systems can help identify medication errors; however, some organizations may over-rely on voluntary reporting to assess medication safety. Additional strategies, such as checklists and independent double-checks, can aid safety monitoring.
This project stresses the significance of entering patient MRNs into smart infusion pumps to trace individualized care. This information can help leadership follow up with potential system barriers to using DERS and develop targeted QI activities.
Strengths and limitations
The high number of audits we conducted for this project complemented the overall elevated DERS adherence rate recognized during pre-intervention data collection. This may have resulted from early notification of the project.
Although we audited and surveyed eight large pediatric units, only one division at one hospital was included. The number of beds (about 1,000) would have been too challenging. In addition, the pediatric units had the lowest overall pre-project adherence rates compared to all other units, providing them with the biggest opportunity for improvement. As a result, the findings aren’t generalizable. Also, we achieved a low response rate for the pre- and post-implementation surveys. In addition, we didn’t include DERS related to arterial lines, central venous catheters, and I.V. flushes, which may be another reason for failing to capture total nonadherence.
Identified need
This project began with a high DERS adherence rate despite an identified gap in adherence noted months earlier. Nonetheless, the project helped us identify the need for continued and sustained DERS adherence and MRN programming. In tandem, these actions mitigate medication administration errors. Other healthcare systems may consider conducting regular audits and surveys to ensure the appropriate use of DERS technology. We recommend also reviewing both medication and I.V. flushes for DERS adherence.
Sunny Carrington-Hahn is a nurse consultant with the Defense Health Agency-Naval Hospital at Camp Pendleton in California. Tracy Gosselin is senior vice president and chief nursing executive at Memorial Sloan Kettering Cancer Center in New York City, New York. Evan Frasure III is director of controlled substance diversion prevention at Duke University Health System in Durham, North Carolina. Staci S. Reynolds is a clinical professor at Duke University School of Nursing.
American Nurse Journal. 2025; 20(1). Doi: 10.51256/ANJ012533
References
Bacon O, Hoffman L. System-level patient safety practices that aim to reduce medication errors associated with infusion pumps: An evidence review. J Patient Saf. 2020;16(3S Suppl 1):S42-7. doi:10.1097/PTS.0000000000000722
Booth JP, Hartman AD. Developing a comprehensive framework of safeguarding strategies to address anticipated errors with organizational high-alert medications. Hosp Pharm. 2024;59(1):47-55. doi: 10.1177/00185787231185871
Dunford BB, Perrigino M, Tucker SJ, et al. Organizational, cultural, and psychological determinants of smart infusion pump work arounds: A study of 3 U.S. health systems. J Patient Saf. 2017;13(3):162-8. doi:10.1097/PTS.0000000000000137
Ibarra-Pérez R, Puértolas-Balint F, Lozano-Cruz E, Zamora-Gómez SE, Castro-Pastrana LI. Intravenous administration errors intercepted by smart infusion technology in an adult intensive care unit. J Patient Saf. 2021;17(6):430-6. doi:10.1097/PTS.0000000000000374
Institute for Healthcare Improvement. Run chart rules reference sheet. 2019. ihi.org/education/IHIOpenSchool/Courses/Documents/11_RunChartRulesReferenceSheet.pdf
Institute for Safe Medication Practices. Guidelines for optimizing safe implementation and use of smart infusion pump. February 10, 2020. ismp.org/guidelines/safe-implementation-and-use-smart-pumps
Institute for Safe Medication Practices. Smart pumps in practice: Survey results reveal widespread use, but optimization is challenging. April 5, 2018. ismp.org/resources/smart-pumps-practice-survey-results-reveal-widespread-use-optimization-challenging
Jani YH, Chumbley GM, Furniss D, Blandford A, Franklin B. The potential role of smart infusion devices in preventing or contributing to medication administration errors: A descriptive study of 2 data sets. J Patient Safe. 2021;17(8):e1894-1900. doi:10.1097/PTS.0000000000000751
The Joint Commission. Sentinel Event Alert 63: Optimizing smart infusion pump safety with DERS. Jt Comm J Qual Patient Saf. 2021;47(6):394-7. doi:10.1016/j.jcjq.2021.03.013
Kuitunen S, Kärkkäinen K, Linden-Lahti C, Schepel L, Holmstrom AR. Dose error reduction software in medication safety risk management—Optimising the smart infusion pump dosing limits in neonatal intensive care unit prior to implementation. BMC Pediatr. 2022;22(1):118. doi:10.1186/s12887-022-03183-8
Lehr J, Vitoux RR, Evanovich Zavotsky K, Pontieri-Lewis V, Colineri L. Achieving outcomes with innovative smart pump technology: Partnership, planning, and quality improvement. J Nurse Care Qual. 2019;34(1):9-15. doi:10.1097/NCQ.0000000000000326
Schnock KO, Dykes PC, Albert J, et al. The frequency of intravenous medication administration errors related to smart infusion pumps: A multihospital observational study. BMJ Qual Saf. 2017;26(2):131-40. doi:10.1136/bmjqs-2015-004465
Shah PK, Irizarry J, O’Neill S. Strategies for managing smart pump alarm and alert fatigue: A narrative review. Pharmacotherapy. 2018;38(8):842-50. doi:10.1002/phar.2153
Key words: patient safety, medication safety, quality improvement

















