
Misidentification can result in negative care and reimbursement outcomes.
- Moisture associated skin damage (MASD) occurs when skin is subjected to repeated moisture.
- MASD is not a hospital-acquired pressure injury (HAPI).
- HAPI and MASD identification occurs in the clinical documentation
- Steroid medication has an impact of skin integrity and may be connected to MASD.
The prevalence of hospital-acquired pressure injuries (HAPI) in patients over age 65 exceeds 15% nationally and 12% globally. Despite advanced technology and tools for early risk identification, HAPI prevalence and incidence haven’t shown sustained decreases. However, clinicians frequently mistake moisture-associated skin damage (MASD) for early-stage HAPI. Location of the skin damage is the most common cause of misidentification.
Typically, MASD (more specifically, intertriginous dermatitis [ITD]) occurs in the folds of the skin in the axilla, inguinal, and peri-anal areas. MASD and PI require distinctly different treatments, which makes accurate identification crucial. In addition, the Centers for Medicare & Medicaid Services requires acute care hospitals to report HAPI to the public. Misidentifying MASD as a HAPI negatively affects reimbursement. (See MASD types.)
Skin failure: A historical perspective
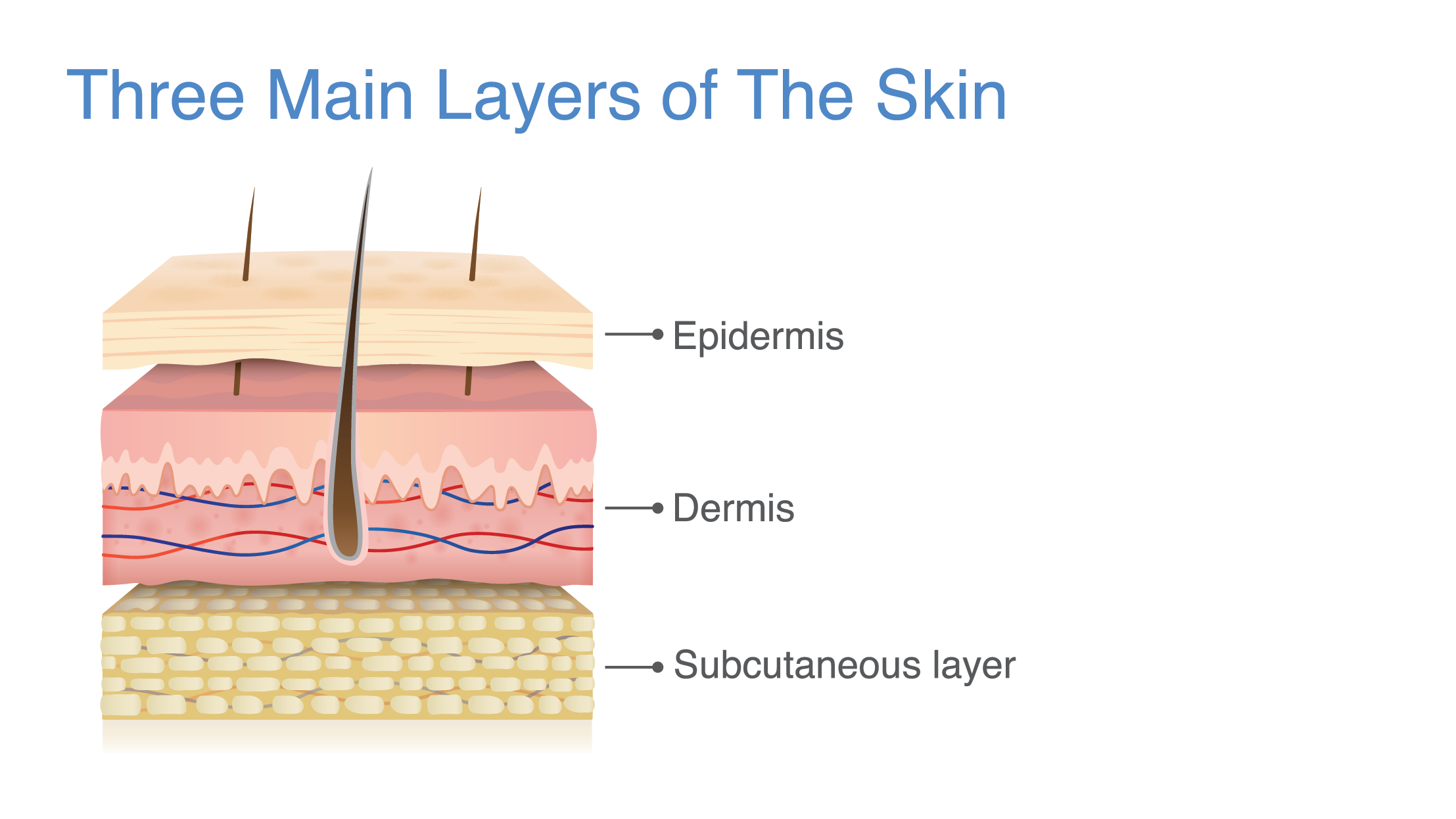
Moisture-associated skin damage: The basics
MASD types
Types of moisture-associated skin damage (MASD)—inflammation that occurs between skin folds—include the following:
- Intertriginous dermatitis
- Incontinence-associated dermatitis
- Peri-wound moisture-associated skin damage
- Peristomal moisture-associated skin damage
Causes include friction, heat, moisture, and lack of exposure to air. An infectious process (most commonly from Candida) also may occur. This increased risk of infection can lead to sepsis. To prevent infection, keep the area clean, dry, and protected from incontinence.
The impetus for our project arose during a monthly bedside nurse project meeting. During one nurse’s presentation of her work on PI prevention, another nurse mentioned observing several patients with MASD receiving steroid medications. This comment sparked discussion, which led to the idea of investigating the literature to explore whether a relationship exists between skin integrity and steroid medications.
Refining our objective
We found little available literature on the prevalence of general skin integrity issues or MASD and steroid use. However, we did find research focused on identifying and treating MASD vs HAPI, along with prevalence rates in various settings. Inaccurate documentation can lead to inappropriate medical treatment, which increases the risk of patient harm.
An exhaustive search found no literature that explored the potential relationship between ITD prevalence or basic skin integrity issues and steroid use. One study that discussed the use of topical steroids to treat ITD noted that although topical steroid use to decrease inflammation has a long history, little evidence exists to support it.
These literature search results prompted us to adjust the focus of our planned research. Rather than focusing on MASD (ITD specifically), we expanded the research to include a primary grouping of skin integrity issues and then a refined subset of MASD because we had no assurances that the clinical documentation identifying MASD would exist. This also would address the common misidentification of MASD as Stage 2 PIs.
The primary group included all skin integrity issues, while the subset included only those instances where electronic health record (EHR) documentation specifically mentioned MASD. In addition, we grouped all steroid medications in the primary group, with only oral or I.V. steroids included in the subset. We extracted data from three areas of the EHR: medications from the medication module and skin integrity issues from a pictorial avatar and the skin assessment module. Although clinicians document skin integrity issues in other locations within the EHR, skin issues always should be documented in these three areas. (See EHR and skin assessment.)
EHR and skin assessment
 We identified three fields within the electronic health record (EHR) that house data points applicable to our research: avatar, skin integrity, and medication administration.
We identified three fields within the electronic health record (EHR) that house data points applicable to our research: avatar, skin integrity, and medication administration.
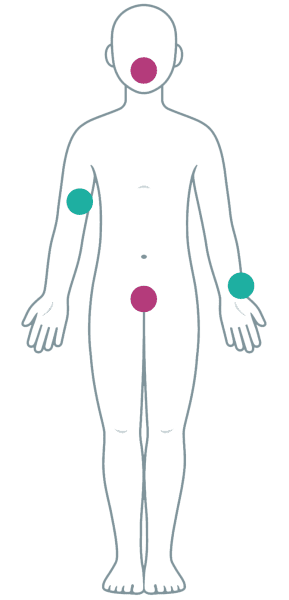
Avatar
The avatar provides a visual display of a human body, front and back (the image at right shows only the front). Nurses can place markers on the image to indicate the presence and type of skin integrity issue. We used two options to identify potential skin integrity issues: Wound—Pressure Injury and Wound—Non Pressure Injury.
Skin integrity
The assessment section of the EHR houses the skin integrity field. At our organization, nurses must perform an assessment at least once during each shift and more frequently if the patient’s condition changes. Possible data entries for potential skin integrity issues include the following:
- Abrasion
- Blanchable erythema
- Blanchable purple discoloration
- Blister
- Blood filled blister
- Bruising
- Burn
- Clobetasol
- Cortisone Acetate
- Edema/Swelling
- Electrode Mark
- Eschar
- Excoriation
- Hematoma
- Incontinence associated dermatitis
- Laceration
- Moisture associated skin damage
- New Epithelium
- Peeling of epidermis
- Petechiae
- Rash
- Redness
- Tear
- Vascular Ulcer
- Weeping
- Comments (other)
Medication administration
The medication administration field is separate from the other two fields but remains within the EHR. We identified several steroid medications in our chart review, including the following:
- Arnuity Ellipta
- Asmanex HFA
- Bacitra-x
- Beclomethasone Dipropionate
- Betamethasone Dipropionate
- Betamethasone Sod Phos & Acet
- Betamethasone Valerate
- Ciclesonide
- Clobetasol Proponate
- Deltasone
- Desonide
- Dexamethasone
- Difluprednate
- Durezol
- Flonase
- Flovent
- Fludrox
- Fluocinolone Acetonide
- Fluocinonide
- Fluorometholone
- Fluticasone
- Hydrocortisone
- Inveltys
- Lotemax SM
- Loteprednol Etabonate
- Medrol (Pak)
- Methylx
- Mometasone Furoate
- Neomycin-Polymyxin-Dexameth
- Neomycin-Polymyxin-HC
- Pred Forte OP
- Prednisolone
- Prednisolon-Gatiflox-Bromfenac 1-0.5-0.075 % OP SOLN
- Prednisone
- Proctozone-HC
- Qvar Redihaler 80 MCG/ACT in Aerb
- Rayos Po
- Sulfacetamide-X
- Tobradex 0.3-0.1 % OP Oint
- Triamcinolone Acetonide
Understanding that the EHR might not provide an accurate representation because of poor, missing, or incorrectly entered documentation, adding to the evidence on this topic required us to start with what was available. We began our dive into this topic to first determine if a relationship exists between steroid medication use and skin integrity issues.
Beginning our research
We reviewed the EHRs from adult patients admitted to a medical-surgical floor in a university medical center. We initially anticipated a minimum of 5,000 instances, but eventually found 213,657 to compare. We included patients admitted between January 1, 2019, and May 31, 2021.
The chart review included incidents of skin damage or steroid medication use rather than unique patients. We made this decision because a patient may or may not have had skin integrity issues or been on steroid medications throughout their entire hospital stay.
We understood that not all entries available under skin integrity indicate MASD and that documentation and classification of skin integrity could vary from person to person. To address this concern, we established a primary group that included all documented skin integrity issues and all steroid medications and a subset group that included all instances where the documentation noted MASD and either oral or I.V. steroid administration.
For example, skin tear and burns wouldn’t indicate potential MASD and aren’t frequently confused with other types of skin damage. The ITD subset included only two entries: incontinence-associated dermatitis and MASD. We included both areas where skin integrity might be documented. Using the avatar for more specific reviews might not prove helpful because it distinguishes only between wounds and non-wounds. It didn’t provide a breakdown or any other level of detail to help us determine whether the issue resulted from moisture or pressure.
The steroid medication subset (select steroids) included those most likely to have an impact on the skin due to dosing quantity. For example, a topical steroid application might not impact the skin as significantly as I.V. or oral steroids. We excluded all ointment, emollient, paste, cream, or ophthalmic solution steroid medications from this subset.
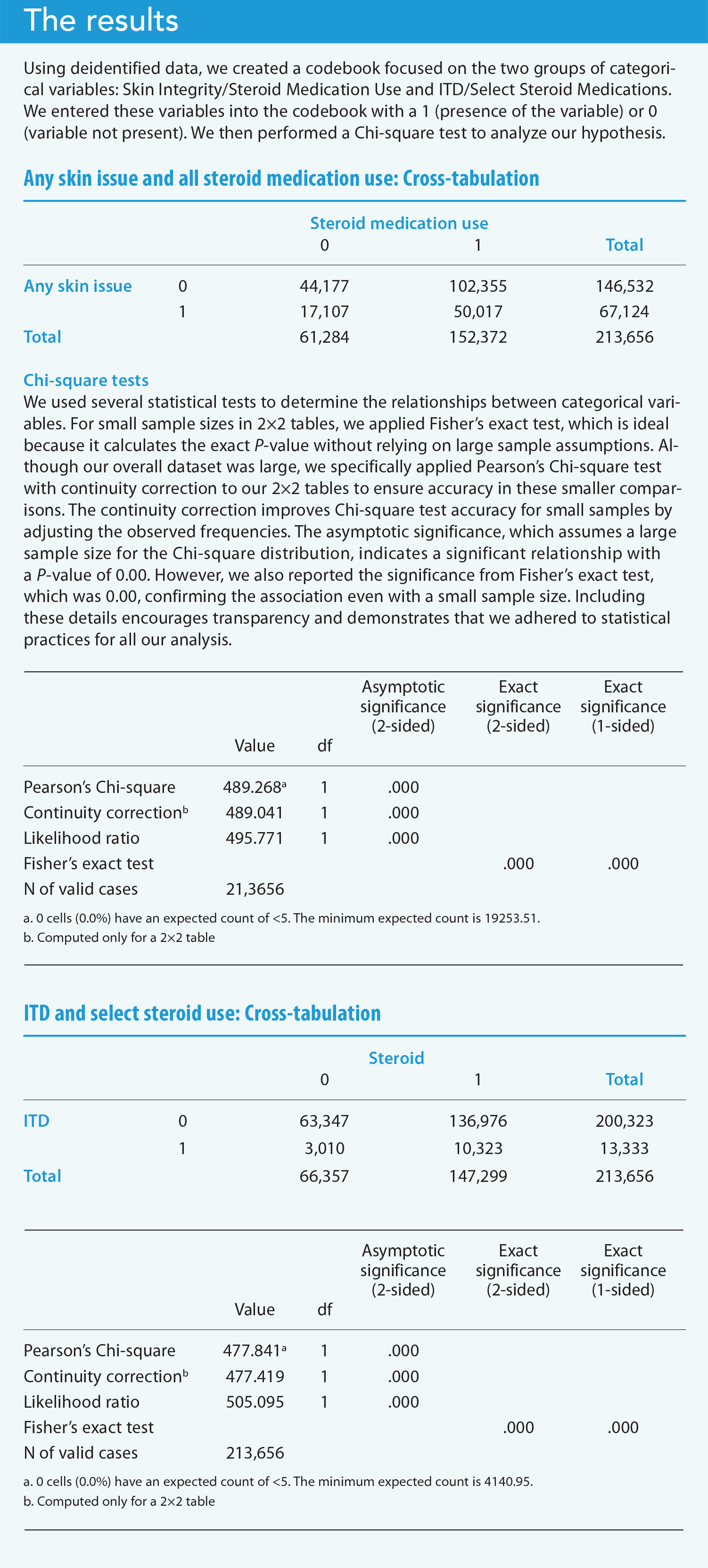
We created a codebook using deidentified data obtained from the retrospective chart review. In reviewing the data, we focused on the two groups of categorical variables: Skin Integrity/Steroid Medication Use and ITD/Select Steroid Medications. For inferential analysis, we entered these variables into the code book with a 1 (presence of the variable) or 0 (variable not present). On the basis of the data distribution, we determined the relationships between groups with nonparametric correlational statistics. We performed a Chi-square test (a statistical hypothesis test that assumes the observed frequencies for a categorical variable match the expected frequencies) for the categorical variable cross-tabulation.
Reviewing the results
We completed a cross tabulation using SPSS version 22. We used Pearson’s correlation (r) to assess whether a statistically significant relationship (occurrence is large enough to be unlikely in the sample without a relationship) existed between the categorical variables. Pearson’s r resulted in a P value of <.05, indicating a statistically significant relationship between skin integrity issues and steroid medication use. We analyzed the additional subset of data looking at only skin integrity issues that described the presence of moisture (ITD) and oral or I.V. steroid medications. Pearson’s r resulted in a P value <.05, also indicating a statistically significant relationship between the subset of categorical variables.
The results indicate that a relationship exists between instances when a patient has a skin integrity issue and when they’re receiving steroid medications. We found this relationship in both the primary group and the group from the EHR that specifically used the words “moisture-associated damage” when completing a skin assessment. (See Results)
Considering the limitations
Despite the large amount of data available and project length, the results may not be generalizable to all facilities or patient populations. We conducted the project at a small university hospital with a large elderly population in the northeast region of the United States. In addition, documentation may have contained inaccuracies or inappropriate use of EHR fields. This study didn’t account for situations or conditions that could have impacted skin integrity, including co-morbid disease states, laboratory results, mobility, and activity levels.
Due to the gap in available literature, we decided to complete this first study as a pilot to determine if a basic relationship exists. We now plan to conduct a follow-up study and include additional variables for consideration, including co-morbid conditions, activity level, and laboratory data.
Understanding the practice and research implications
We found several implications for nursing practice and research, including steroid use in skin integrity assessment, data accuracy, the need for research refinement, and the consequences of inaccuracy or misidentification of skin issues.
Steroid use in skin integrity assessment
Despite anecdotal awareness that steroid medications impact skin integrity, we found no relevant studies on this topic. Our research identified a statistically significant relationship between skin integrity and steroid medication use, but because no other similar studies exist, we can’t compare these results or discuss potential deviations.
Imperfect data
Data collection must offer an accurate representation of the patient and the care provided. These accuracy challenges will continue to require researchers to account for data variations and mis-documentation.
If we want to use EHR data to improve care or identify gaps, we must use what’s currently available and then work to make improvements for the future. Collaborate with your hospital’s informatics group to add available selection options, improve avatars, or combine entry options when overlap or duplication exists. Rather than focusing on the front end (data collection by the user), consider the backend and use entries that populate in other areas of the record. For example, if a nurse identifies a skin integrity issue while completing the physical assessment, that assessment data should populate on the avatar. Nurses shouldn’t have to remember to enter it in another location.
These recommendations also would apply to alerts or triggers. Nurses use the Braden scale to identify patients at risk for skin integrity issues. As the patient’s EHR is populated, those individual data elements should automatically generate a Braden risk score. For instance, if a nurse documents that a patient is bed bound or not ambulatory, that information should automatically populate in the Braden risk score calculation.
Research refinement
The ease of access to electronic data doesn’t negate the need to first understand what’s available and how we collect data. For example, we know that several variables can impact skin integrity. This pilot study helped us determine if a relationship existed, without factoring in confounding variables.
Inaccuracy or misidentification
Although we didn’t track or include costs within the context of this research project, it’s important to note the confusion between MASD and Stage 2 PI and the risk for negative impact on organization reimbursement in the event of misclassification.
Accuracy key to improvement
We can’t stress enough the importance of accurate healthcare documentation. Consider completing an audit to assess your organization’s EHR in relation to skin assessment documentation. Are staff correctly identifying and documenting MASD vs PI? A larger-scale review will help determine if the addition of clinical, mobility, activity, and laboratory variables support the conclusions of our current study.
Kathryn Fleming is president of Clinical Consulting Services in North Hanover, New Jersey. Isabella Kocienski is a bedside RN at Ocean University Medical Center in Brick, New Jersey.
American Nurse Journal. 2024; 19(8). Doi: 10.51256/ANJ082413
References
Borojeny LA, Albatineh AN, Dehkordi AH, Gheshlagh RG. The incidence of pressure ulcers and its associations in different wards of the hospital: A systematic review and meta‑analysis. Int J Prev Med. 2020;11:171. doi:10.4103/ijpvm.IJPVM_182_19
Centers for Medicare & Medicaid Services. Hospital-acquired condition reduction program. October 27, 2023. cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/Value-Based-Programs/HAC/Hospital-Acquired-Conditions
Floyd NA, Dominguez-Cancino KA, Butler LG, Rivera-Lozada O, Leyva-Moral JM, Palmieri PA. The effectiveness of care bundles including the Braden scale for preventing hospital acquired pressure ulcers in older adults hospitalized in ICUs: A systematic review. Open Nurs J. 2021. doi:10.2174/1874434602115010074. opennursingjournal.com/volume/15/page/74/fulltext
Gabriel S, Hahnel E, Blume-Peytavi U, Kottner J. Prevalence and associated factors of intertrigo in aged nursing home residents: A multi-center cross-sectional prevalence study. BMC Geriatr. 2019;19(1):105. doi:10.1186/s12877-019-1100-8
National Pressure Injury Advisory Panel. NPIAP pressure injury training modules 1-3. learn.npiap.com/products/npiap-pressure-injury-training-modules-1-3
Nobles T, Miller RA. Intertrigo. StatPearls. September 19, 2022. ncbi.nlm.nih.gov/books/NBK531489
World Health Organization. WHO calls for global action on sepsis—Cause of 1 in 5 deaths worldwide. September 8, 2020. who.int/news/item/08-09-2020-who-calls-for-global-action-on-sepsis—cause-of-1-in-5-deaths-worldwide
Key words: intertriginous dermatitis, ITD, moisture associated skin damage, MASD, steroid medication














1 Comment. Leave new
American nurse journal is doing a great job in terms of continuous education in nursing practice and professionalism.