

Sustaining a framework and advancing nursing professionalism
- Shared governance provides nurses with a voice to guide and influence practice change.
- This hospital created a job description for shared governance representatives (SRGs), which includes supporting nurse educators and working on a range of projects aimed at driving change and improving patient outcomes.
- The SRG role aids engagement and provides nurses with an opportunity for professional development.
Start and colleagues describe shared governance, a foundational component of Magnet®-recognized hospitals, as empowering frontline nurses with decision-making authority. It serves as a structural model through which nurses can express and manage their practice with professional autonomy, partnership, equity, accountability, and ownership. Hess refers to shared governance as decision-making among nurse leaders and frontline staff nurses with regard to evidence-based practice (EBP) projects, equipment purchases, staffing allocation and utilization, and other key resources.
Shared governance can prove successful at different levels throughout an organization, including unit, specialty, campus-wide, regional, and system levels. The American Nurses Credentialing Center defines shared governance as a dynamic partnership among leadership, nurses, and other healthcare professionals that helps promote collaboration, decision-making, and accountability to ensure quality patient outcomes and enhance nurses’ work life.
Nursing ethics and shared governance model
Fisher and colleagues recognize hospitals with shared governance as key to providing a safe, comfortable, and collaborative environment for nurses. It allows them enhanced autonomy and opportunities to achieve higher levels of care within their practice. A professional practice environment requires autonomy. According to Start and colleagues, nurses who provide direct patient care should make 90% of clinical decisions. Shared governance provides nurses with a voice to guide and influence change in their practice. Positive outcomes associated with shared governance include staff empowerment and engagement, a collaborative culture, improved patient outcomes, and opportunities for leadership.
A Magnet-recognized hospital in Northeastern Pennsylvania has established a strong shared governance structure, which includes various councils and shared governance representatives (SGRs) who have become true partners in practice improvement and patient care quality.
A history of shared governance
For over a decade, our organization has enculturated a shared governance structure at the council and unit levels, which ensures that nurses have a voice in their practice. Goals of this framework include providing council members with a holistic view of operations, fostering collaboration among departments, and giving nurses a voice in decisions.
Interprofessional team members across the hospital recognize the shared governance councils as a forum of nurse collaboration aimed at gaining knowledge and sharing best practices to improve practice and patient outcomes. To ensure all units have a voice in their practice, they each have at least one SGR from day shift and night shift (or however many the unit can support). SGRs also help ensure attendance at council meetings and increase nurse involvement and engagement.
The SGR role
The SGR job description focuses primarily on the role, which has evolved over the years, as an extension of the nurse educator assigned to a unit. They support nurse educators in developing education, including onboarding and selecting annual competencies using the Wright Model for Competency Assessment. SGRs also collaborate with nurse educators in deciding how staff demonstrate knowledge.
SGRs have protected time each month to attend the 8-hour in-person council day. Originally, they also had an additional 4 to 8 hours per month of protected time on the unit to complete projects. The role’s evolution has increased protected time to 16 hours per month.
As part of their dedicated time, SGRs serve in various roles and work on a range of projects and initiatives that drive change and improve patient outcomes throughout the hospital. They serve as preceptors; resources for all staff, patients, and families; role models; skin care/mobility champions; unit practice council facilitators; education liaisons; and active participants in conversations, problem-solving, and information sharing.
As unit leaders, SGRs facilitate their unit practice councils. They also collaborate with their nursing operations leaders to monitor quality metrics and develop strategies to improve quality outcomes of specific patient populations. Our organization achieves nursing operations leadership support through quarterly one-on-one meetings with nursing professional development leaders. Conversations at these meetings include discussion of program value, current SGR council activity, and future unit staff needs.
Discussion of the SGR role led to the nursing operations team seeing the value that these bedside leaders bring to their unit. Many units asked for additional SGR positions.
Council agenda and committee structure
Shared governance councils help each nurse participate in achieving quality patient care outcomes. Through shared governance, all nurses act as patient care leaders.
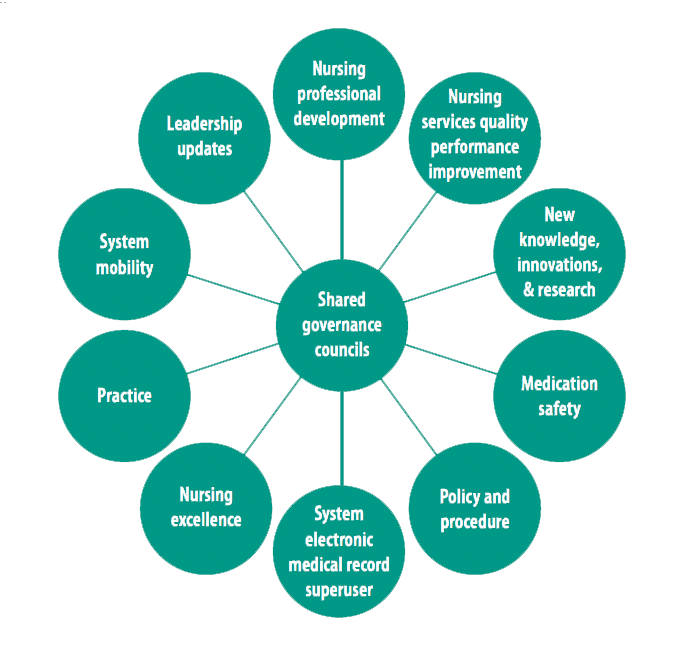
The 8-hour shared governance council day comprises an array of nursing councils in which all SGRs participate. SGR input, campus/system priorities, and collaborative partnerships have led to the development of these councils, which include Nursing Professional Development, Nursing Services Quality Improvement, New Knowledge, Innovations & Research, Nursing Excellence (Magnet), Policy and Procedure, Medication Safety, System Electronic Medical Record Superuser, System Mobility Committee, and Nursing Leadership Updates. (See Shared governance: Successful framework.)
Shared governance: Successful framework
Our organization’s shared governance structure includes several councils, which meet once a month for 8 hours to share ideas, review data, and develop recommendations to improve practice and patient outcomes.
- Nursing Professional Development Council. Coordinate the dissemination of new knowledge and clinical practice to all nursing staff and provide a structure to support a culture of continuous learning.
- Nursing Services Quality Performance Improvement Council. Provide an interprofessional structure to support a culture of continuous performance improvement, safety, and regulatory compliance. Review and identify nursing quality indicators to monitor for improvement of patient care quality outcomes.
- New Knowledge, Innovations & Research Council. Understand nursing research and discuss its use in current practice. Collaborate with team members and leaders to create a New Knowledge, Innovations & Research environment for implementing improvement strategies. Facilitate evidence-based practice interventions to advance nursing practice and patient outcomes.
- Practice Council. Make key decisions regarding nursing council activities and organize nursing action via evidence-based best practice. To address nursing practice issues or concerns, co-facilitation occurs in conjunction with two nursing operations managers.
- Nursing Excellence (Magnet®) Council. Promote and support the Magnet culture through education, integration of the Professional Practice Model, and evidence-based best practice standards.
- Policy and Procedure Council. Establish and maintain policies based on evidence-based practice by developing clear and concise nursing guidelines. Report any policy changes or updates to the system-wide policy and procedure council.
- Medication Safety Council. Prevent harm and reduce the risk of adverse events via data analysis, literature review, and proactive initiatives within the medication-use system.
- System Electronic Medical Record Superuser Council. Implement changes, update current electronic health record tools, and share new needs and updates.
- System Mobility Council. Collaborate with the health system on mobility initiatives and data overview.
- Nursing Leadership Updates Council. Dedicated time to attend and provide updates on campus, region, and system news; perform stoplight report reviews; discuss nursing quality metrics; and provide Q&A opportunities.
Leadership connection
Nurse leaders can support decision-making by helping to ensure shared governance councils have the protected time, resources, education, and support they need to guide the practice environment and practice outcomes. However, because not every nurse can participate as a member of a shared governance council, structures and processes should enable bidirectional communication and feedback among all nurses at the unit level to help drive action plans, practice changes, and nurse autonomy. This approach creates an environment where bedside nurses feel engaged and comfortable having conversations with nurse leaders.
Engaged staff, vital to a shared governance structure, require leadership trust and commitment. During the dedicated shared governance day, the chief nursing officer and other nursing leaders provide a forum for concerns and ideas. Follow-up helps establish trust and a connection with the nurse leaders, which increases bi-directional communication.
Clinical nurses and EBP
Shared governance nurse members engage in various EBP projects each year. The New Knowledge, Innovations & Research council aims to advance members’ skills in generating new knowledge, potentially establishing a gateway to promote nursing research. Ultimately, clinical nurses should define the parameters of nursing professional practice and performance through the development and implementation of protocols and standards of practice via evaluation of EBP and regulatory compliance.
Each month’s council day agenda builds on the previous month, establishing knowledge of the Johns Hopkins Model of Evidence-Based Practice, gaining managerial support, submitting projects for Institutional Review Board approval, and conducting projects. Teams form into self-assigned groups and determine project direction, distribution of assignments, review of literature, and development of actionable items throughout the year. SGRs partner with content experts on the relevant subject matter and ensure nursing leaders receive regular project updates, including any encountered barriers.
At the end of each year, the SGRs present at an annual symposium to an audience of executives, leaders, nursing professionals, and collaborative practice partners. Active engagement ensures that leaders hear SGR nurses’ voices and that changes to nursing practice result. The over 100 completed projects include development of nurse driven protocols, product changes, streamlined electronic health record documentation, regulatory performance improvement action plans, additional equipment purchases, communication enhancements, and department engagement and nurse health and safety improvements.
Evolving structure
SGR feedback enhances the shared governance structure and builds upon the previous year’s outcomes, direction, and interests. Direct care nurses provide regular feedback—such as reducing the number of councils due to repetitive discussions—to enhance the shared governance role. For example, discussions in the former Nursing Retention and Recruitment Council (NRCC), which focused on staffing, also occurred in the Nursing Leadership Updates Council. The SGRs felt that this redundancy resulted in no resolution because key stakeholders couldn’t attend at the same time to approve suggestions. Other councils, such as the Nurse Practice Council, discussed nurse retention solutions. Ultimately, the SGRs eliminated the NRCC.
Although councils for each region (Northeast, Central, Western, and North Central) of this health system underwent revision, leadership considered combining the two Northeast campus council days; they frequently discussed the same issues and offered opportunities to pursue a regional practice approach. Before this regionalization, duplication frequently resulted in delays regarding decisions on practice or policies because the separate campus councils occurred at various times and days and changes required approval from both campuses. The SGRs and nursing leadership team agreed to combine both campus councils into one regional council with separate nursing practice councils to discuss issues unique to each campus.
SGR retention and professional development
Each year, 40% to 50% of SGRs reapply for the role; in 2024, 75% reapplied. This retention helps to extend work on initiatives, maintain rapport with leadership, and ensure a high level of engagement to improve nursing practice and patient outcomes. The SGR program also has led to leadership development; several clinical nurses have assumed other nursing leadership roles, including middle management, manager, nurse educator, and nurse specialist.
Taking advantage of SGR as a professional development platform has enabled clinical nurse advancement. Over 55% of nurse managers, clinical coordinators, and nursing professional development practitioners previously served as SGRs. The role opens doors for a voice in practice, professional development, and leadership evolution.
Time and a village
The establishment of a robust shared governance structure has enabled not only collaborative decision making but also advancements in nursing practice and professional development within an acute care setting. Nursing leaders and interprofessional teams rely on clinical nurses in the SGR role to serve as sounding boards. The SGRs provide valuable feedback, including with regard to the council’s evolution.
It takes time and a village to establish a strong shared governance structure. With a reliable team, positive practice changes begin to occur when clinical nurses participate and see advancements, which in turn leads to more engagement and partnership.
The authors work at Geisinger Health System in Wilkes-Barre, Pennsylvania. Lauren M. Murphy is manager of nursing quality. Lindsey Ford is system director of nursing excellence, shared governance, and nurse residency/fellowship programs. Megan Lamoreux is northeast regional manager of nursing professional development.
American Nurse Journal. 2025; 20(1). Doi: 10.51256/ANJ012528
References
American Nurses Credentialing Center. 2023 Magnet® Application Manual.
Fisher CA, Jabara J, Poudrier L, Williams T, Wallen GR. Shared governance: The way to staff satisfaction and retention. Nurs Manager. 2016;47(11):14‐6. doi:10.1097/01.NUMA.0000502808. 67918.e8
Hess RG. Shared governance: Nursing’s 20th-century Tower of Babel. J Nurs Adm. 1995;25(5):14-7. doi:10.1097/00005110-199505000-00005
Orton A. Supporting nursing autonomy through shared governance. Nurs Manage. 2021;52(12):44-6. doi:10.1097/01.NUMA.0000800404.94545.fb
Start RE, Hancock BJ, Porter-O’Grady T. Professional Governance for Nursing: The Framework for Accountability, Engagement, and Excellence. Burlington, MA: Jones & Bartlett Learning; 2024.
Swihart D, Hess R. Shared Professional Governance: A Practical Approach to Transforming Interprofessional Healthcare. 5th ed. Pennsauken, NJ: BookBaby; 2023.
Wright D. The Ultimate Guide to Competency Assessment in Health Care. 3rd ed. Bloomington, MN: Creative Health Care Management; 2005.
Key words: shared governance, shared governance representatives, professional development















