Recognizing those at risk and exploring evidence-based strategies
Takeaways:
- Stroke prevalence is projected to rise significantly by 2030 and increasing survivorship will lead to increased hospital discharges and potential for readmissions.
- Stroke readmissions are multifaceted and complex. In addition to recognizing risk factors for recurrent stroke, nurses should focus on impacting potentially preventable readmission complications such as medication adherence issues, post-discharge infection, and other readmission etiologies.
- The versatility of the nursing profession across diverse settings positions nurses to impact stroke transitional care.
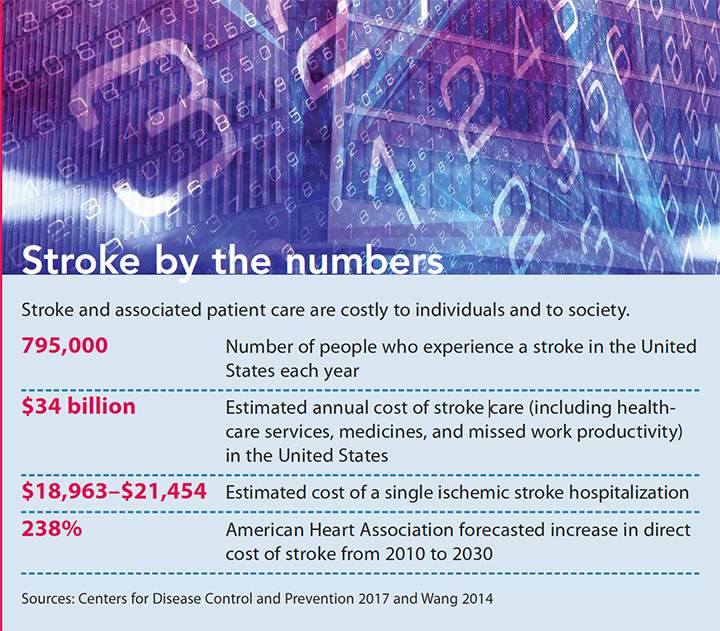
STROKE is a leading cause of long-term disability and mortality and its impact is far-reaching. (See Stroke by the numbers.) Stroke death rates in the United States are on the decline, but projections suggest that because of the aging population, prevalence will continue to increase. By 2030, an additional 3.4 million U.S. adults will have had a stroke, a 20.5% increase in prevalence from 2012. Stroke disproportionately affects Blacks (this population is two times more likely to suffer from first-time stroke when compared to Whites), and death rates among Hispanics has been increasing since 2013. Stroke survivors number in the hundreds of thousands each year, many of whom suffer from a variety of poststroke disorders, which can lead to readmission. With approximately 12% of ischemic stroke patients readmitted within 30 days after discharge, readmissions have become a popular targetable outcome measure, and readmission prevention has become a topic of national discussion. Understanding stroke and its etiologies and risk factors can help you identify patients at risk for readmission before they even leave the hospital.
Stroke defined
A stroke, defined as the sudden onset of neurologic deficit due to a vascular cause, can be classified as hemorrhagic (rupture of a vessel within the brain) or ischemic (acute obstruction of an intracranial vessel); 87% of strokes are ischemic. The blockage or rupture causes reduced blood flow to a brain region. If blood flow interruption persists, brain tissue within that region dies. Clinical manifestations vary, but can include loss of sensory or motor function on one side of the body; change in vision, gait, or ability to speak; or a sudden severe headache. Rapid evaluation of stroke is essential for medical treatment, including recanalization with clot dissolution via tissue plasminogen activator (tPA) or clot removal via thrombectomy. Risk factors for stroke include age, smoking, hypertension, diabetes, and history of high cholesterol.
Knowing a stroke’s etiology— atrial fibrillation, hypertension, atherosclerosis— can aid in establishing secondary prevention strategies. These strategies, such as treatment with a statin, antihypertensive, or appropriate antithrombotic, are essential to the patient’s discharge plan. They also are vital quality indicators. The etiology of nearly 30% of strokes remains unexplained, regardless of extensive workup.
Stroke and 30-day readmission rates
 The Centers for Medicare & Medicaid Services (CMS) reports 30-day risk-standardized readmission rates for patients discharged from the hospital with a diagnosis of ischemic stroke. The outcome, defined as any unplanned hospital readmission within 30 days of discharge, is a vital target for quality measures and improvement initiatives. This measure has been prioritized at the national level because of the high risk for readmission in this population. In some cases, readmission after stroke may be due to disease progression, but it also may be an indicator of poor quality inpatient and/ or outpatient care. The Medicare Access and CHIP (Children’s Health Insurance Program) Reauthorization Act of 2015 addresses this by requiring hospitals to provide care coordination, care plans, patient engagement for self-management, and shared decision-making for medically complex individuals.
The Centers for Medicare & Medicaid Services (CMS) reports 30-day risk-standardized readmission rates for patients discharged from the hospital with a diagnosis of ischemic stroke. The outcome, defined as any unplanned hospital readmission within 30 days of discharge, is a vital target for quality measures and improvement initiatives. This measure has been prioritized at the national level because of the high risk for readmission in this population. In some cases, readmission after stroke may be due to disease progression, but it also may be an indicator of poor quality inpatient and/ or outpatient care. The Medicare Access and CHIP (Children’s Health Insurance Program) Reauthorization Act of 2015 addresses this by requiring hospitals to provide care coordination, care plans, patient engagement for self-management, and shared decision-making for medically complex individuals.
Many stroke patients are discharged to settings that require ongoing care, and evidence suggests high rates of potentially preventable complications, such as urinary tract and respiratory infections. CMS recognizes that both of these complications can lead to readmission. Fortunately, opportunity exists to reduce readmission through appropriate intervention. Research indicates that improved care coordination can reduce readmission rates and healthcare costs in a variety of diseases, and it’s reasonable to assume this can be achieved in stroke patients as well.
The American Stroke Association and American Heart Association also have examined using 30-day all cause readmissions as a measure of hospital care quality. Although they recognize some strengths associated with this measure, they have identified limitations. Specifically, not all readmissions are preventable (so planned or elective readmissions should be excluded from the measure), hospitals may have little control of care after discharge, and readmission measures could create incentives to deny patients hospital admission, further contributing to the nation’s access to care issues.
Ultimately, this readmission measure may best be used when combined with metrics of poststroke functional status and mortality. And defining modifiable aspects of stroke care that can improve patient outcomes, including focusing on preventable causes of readmissions, deserve additional research.
Readmission factors
Identifying predictors of readmission after ischemic stroke may play an essential role in preventing them. Several studies have attempted to assess risk factors and etiologies of readmission in this population. An examination of the 2013 Nationwide Readmission Database representing all U.S. hospitalizations provides perhaps the broadest view. It determined that 12.1% of ischemic stroke patients were readmitted within 30 days of discharge, 89.6% of those readmissions were unplanned, and 12.9% were considered potentially Stroke and associated patient care are costly to individuals and to society. 795,000 Number of people who experience a stroke in the United States each year $34 billion Estimated annual cost of stroke care (including healthcare services, medicines, and missed work productivity) in the United States $18,963–$21,454 Estimated cost of a single ischemic stroke hospitalization 238% American Heart Association forecasted increase in direct cost of stroke from 2010 to 2030 Sources: Centers for Disease Control and Prevention 2017 and Wang 2014 Stroke by the numbers AmericanNurseToday.com December 2018 American Nurse Today 11 preventable. Those readmitted had Medicare coverage, a lower household income, were older, and had a higher proportion of individual comorbidities. Patients receiving recanalization therapy had lower odds of readmission.
Several retrospective analyses have assessed risk factors for and causes of readmissions.
Statins
One retrospective analysis identified that individuals taking statins had lower readmission rates than those not taking statins. Likewise, individuals less than 80 years old had lower readmission rates compared to those 80 years or older. And all cause readmissions were affected by statin use. This information highlights the role statins play in secondary prevention.
Causes for readmission: The study showed that after recurrent stroke, respiratory diseases, such as pneumonia and influenza, are the most common cause of readmissions.
30-day readmission
A retrospective analysis examining mortality in 30-day readmissions after stroke found that mortality is 2.5 times higher in stroke than in other admissions, and in those readmitted for recurrent stroke, mortality is greatest. Risk factors associated with 30- day readmission included age more than 75 years; living in a facility prior to stroke; comorbidities, such as previous stroke, diabetes, heart failure, and atrial fibrillation; and admission to a non-neurology service.
Causes for readmission: This study found that the most common reason for readmission was urinary tract or respiratory infection, followed by recurrent stroke or transient ischemic attack.
Long-term care
Up to one-third of patients who’ve had a stroke require long-term care placement after they’re discharged, which may mean that care in these settings and readmission characteristics from them should be considered. Assessment of the CMS Minimum Data Set in nursing home residents was scrutinized in an attempt to generate models for readmission prediction.
Causes for readmission: Although these particular models didn’t significantly improve prediction accuracy, progressively lower odds of readmission were associated with certain patient characteristics, including lower comorbidity scores on formalized comorbidity indexes and higher levels of social engagement in the nursing home after hospital discharge.
Demographics
A retrospective analysis of the demographic characteristics from an urban primary stroke center supports the findings of the literature mentioned above.
Causes for readmission: This analysis determined that most 30- day readmissions after stroke are for noncerebrovascular complications attributed to a variety of factors, including respiratory infections, GI complications, and injury.
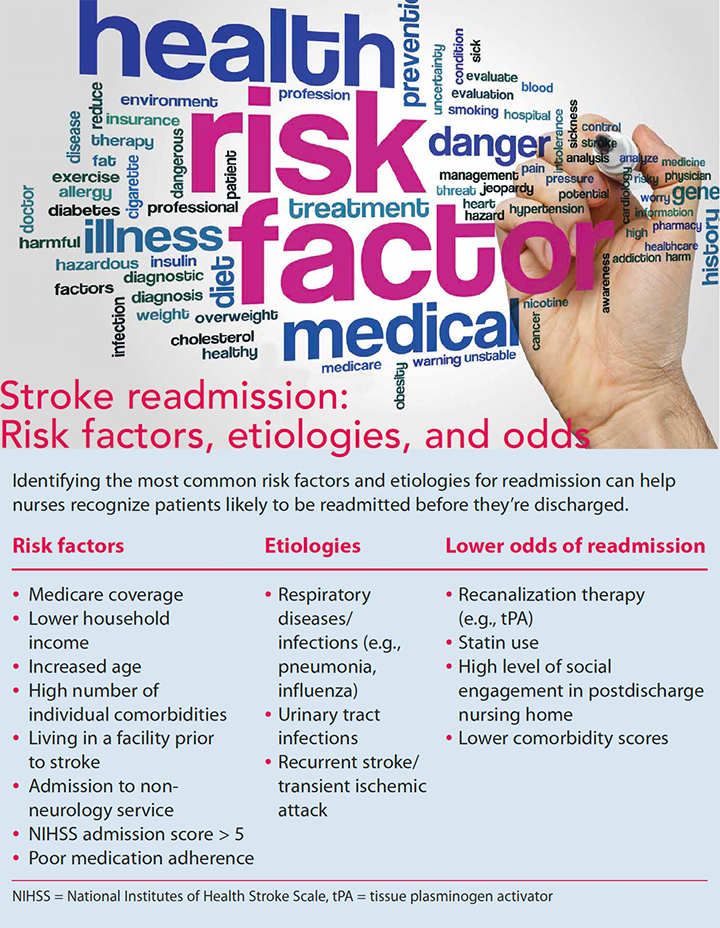
All of these studies highlight the multifaceted risk factors and etiologies that affect stroke readmissions. (See Stroke readmission: Risk factors, etiologies, and odds.) And with as many as 70% of stroke survivors requiring assistance with activities of daily living, medication adherence can be particularly challenging. In addition to barriers related to medication cost and access, stroke survivors often suffer from mild, unrecognized physical and cognitive deficits that affect their ability to take medications as prescribed, and family caregivers may be ill-prepared to manage the medications.
Interventions to reduce readmissions
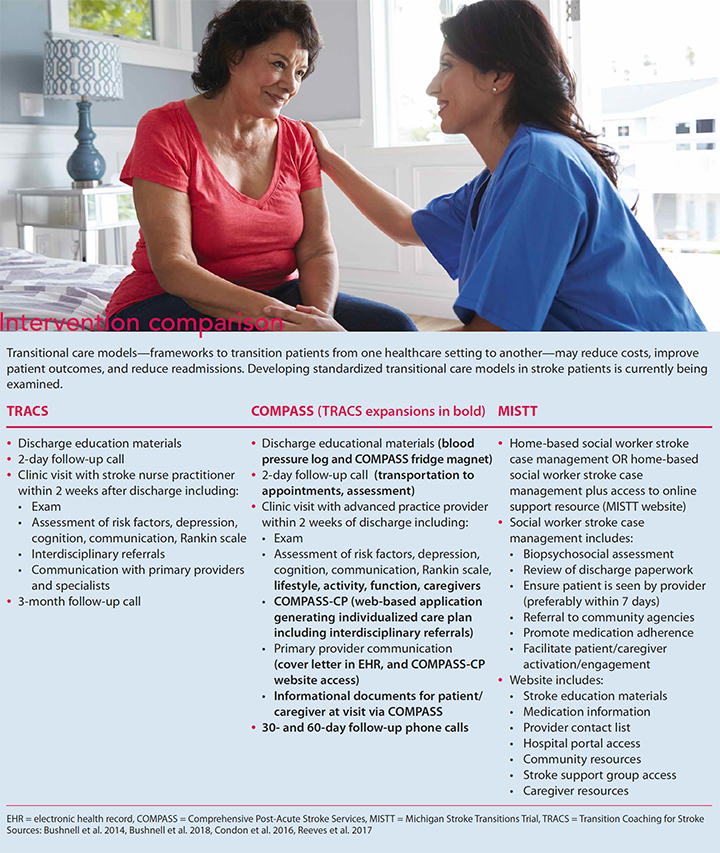
Little research exists about successful interventions for posthospital transitions in patients who’ve experienced a stroke. In most of the studies that do include stroke patients, few have demonstrated a significant degree of positive benefit from transitional care models, which is surprising since these models have been effective when tested with other diagnoses. However, researchers continue to scrutinize various transitional care frameworks because multicomponent interventions can reduce healthcare costs, provide patient-centered care, and positively impact readmissions. Several promising programs have begun to emerge, including the Transition Coaching for Stroke (TRACS) model, the Comprehensive Post-Acute Stroke Services (COMPASS) trial, and the Michigan Stroke Transitions Trial (MISTT). (See Intervention comparison.)
TRACS
The TRACS model is one of the most encouraging frameworks to date and serves as a foundation for additional clinical trials developing stroke transition evidence. TRACS addressed the immediate needs of stroke patients recently discharged home by providing coaching through a nurse practitioner–led transitional stroke clinic. Participants received medication education, as well as followup phone calls from an RN, who reviewed medications, assessed new problems after arriving home, and confirmed appointments. Nurse practitioners saw each patient after discharge and performed a standardized assessment that included evaluating medication use (persistence), missed medication doses (adherence), and addressed any medication access or side-effect issues.
Patients received a telephone call 2 days after discharge for medication reconciliation, assessment of functional markers, and confirmation of the transitional stroke clinic appointment. TRACS demonstrated an overall medication regimen persistence (medications the same from discharge to follow-up) of 80.3%. Additionally, those who received a follow-up call were more likely to attend the transitional stroke clinic visit, and this visit resulted in a 48% reduction in 30-day readmission rates.
TRACS’ role in medication persistence and adherence may help address secondary prevention of recurrent stroke. Stratifying risk factors (such as atrial fibrillation and hyperlipidemia) allows medications to be prescribed to modify them. For example, measuring a lipid profile and subsequent treatment with a statin is a reported core performance measure. However, appropriate medication is only the first step in secondary prevention; medications must be taken to be effective, making interventions like TRACS promising.
The TRACS model provides a solid foundation of existing evidence for a stroke transitional model, but more evidence is needed because the United States has no established standard for using this type of model after discharge. This is inconsistent with care currently provided in Canada and the United Kingdom, where early supported discharge has been widely tested and adopted in stroke transition management. The COMPASS and MISTT trials are attempting to address this gap.
COMPASS
The COMPASS model, an extensive trial taking place across 41 hospital sites involving more than 6,000 participants, uses the TRACS model as its foundation and expands on several key components to more comprehensively address stroke patients’ medical, psychosocial, and practical discharge needs. Highlights of the COMPASS expansion include telephone follow-up at 2, 30, and 60 days after discharge to address medication reconciliation, transportation to appointments, functional status, and referrals; clinic visit including a standardized assessment conducted by a nurse and provider within 14 days after discharge; a community resources directory based on patient address and needs; and self-reported functional and social determinants of health via a web-based application (COMPASS-CP). This application, considered one of the highlights of the COMPASS expansion, uses algorithms that look at various assessments— poststroke limitations, medication reconciliation, and lifestyle information—to generate an individualized care plan with suggestions for self-management and referrals.
MISTT
MISTT aims to add valuable evidence by establishing a standard of care to address psychosocial and health-related challenges facing stroke survivors and their caregivers during the postdischarge transition. The trial plans to improve stroke survivor and caregiver outcomes by concentrating on patient activation and quality of life. Primary goals focus on home-based case management by social workers that includes a visit within a week of returning home, a second visit about 30 days later, and weekly follow- up phone calls. A patient-centered online information resource will be added in a second intervention group to provide stroke and medication information and support group access.
The ultimate goal of MISTT is to actively engage stroke patients and caregivers in decision-making and self-management after returning home by incorporating social work principles, healthcare technology, and aspects of the chronic care model. Highlights of the trial include reviewing discharge paperwork and incorporating identified discharge activities; promoting medication adherence through education, lists, and pill organizers; individualizing education to emphasize the importance of stroke prevention and recovery; and facilitating access to community services.
Nursing and stroke readmission prevention
As many as 60% of stroke survivors require postacute care services in a variety of settings, including rehabilitation facilities, skilled nursing centers, outpatient rehabilitation, and home health. This means that you have an opportunity to help transform healthcare transitions for these patients by identifying and documenting suspected transition issues early, implementing strategies to address them, and communicating the transition plan effectively. (See Nursing and stroke care transitions.)
You must work as part of the interprofessional care team to develop and evaluate the transitional care plan. A key component to ensuring optimal outcomes for stroke survivors starts with determining the appropriate level of care they need after discharge. You can add vital input through your assessments and close patient and family interactions, which can provide insight into circumstances that may affect transitional care planning.
Help patients and caregivers be engaged as active partners and advocates in their postdischarge care by educating them about what they should expect. For example, patients should expect to be routinely assessed for medical needs, prestroke function, rehabilitation tolerance, community support needs and options, financial barriers, and family caregiver dynamics. Additional support includes providing information, education, and resources on care needs; stroke prevention and recovery; strategies to manage emotional, financial, and family needs; medication management, adherence, and access; and follow-up care.
Use your knowledge
Whether or not you work in an organization that has an established stroke transitional care model, use your knowledge about readmission risk factors, etiologies, and successful components of existing and emerging models to focus patient education. And use this knowledge to stratify individualized risk during a patient’s hospital stay and throughout various levels of care and create actionable targets for intervention. For example, stratification can be used to reduce postdischarge infection, screen for and recognize barriers to medication adherence, provide medication education, and reconcile medications.
Taken together, this knowledge provides nurses with a platform to advocate for adopting successful transitional models in various practice settings by championing quality improvement initiatives and insisting on the use of evidence-based transitional care.
Kristen M. Poston is an instructor at the Medical University of South Carolina College of Nursing in Charleston.
Selected references
Benjamin EJ, Virani SS, Callaway CW, et al. Heart disease and stroke statistics—2018 update: A report from the American Heart Association. Circulation. 2018;137(12):e67-e492.
Bushnell C, Arnan M, Han S. A new model for secondary prevention of stroke: Transition coaching for stroke. Front Neurol. 2014; 5:219.
Bushnell CD, Duncan PW, Lycan SL, et al. A person-centered approach to poststroke care: The COMprehensive Post-Acute Stroke Services model. J Am Geriatr Soc. 2018; 66(5):1025-30.
Camicia M, Lutz BJ. Nursing’s role in successful transitions across settings. Stroke. 2016;47(11):e246-9.
Centers for Disease Control and Prevention. Stroke facts. Updated September 6, 2017. cdc.gov/stroke/facts.htm
Centers for Medicare & Medicaid Services. Hospital 30-day, all-cause, unplanned riskstandardized readmission rate (RSRR) following an ischemic stroke hospitalization. Agency for Healthcare Research and Quality. 2017. Updated November 13, 2017. https:// cmit.cms.gov/CMIT_public/ViewMeasure?Me asureId=5043
Condon C, Lycan S, Duncan P, Bushnell C. Reducing readmissions after stroke with a structured nurse practitioner/registered nurse transitional stroke program. Stroke. 2016; 47(6):1599-604.
Duncan PW, Bushnell CD, Rosamond WD, et al. The comprehensive post-acute stroke services (COMPASS) study: Design and methods for a cluster-randomized pragmatic trial. BMC Neurol. 2017;17(1):133.
Fehnel CR, Lee Y, Wendell LC, et al. Postacute care data for predicting readmission after ischemic stroke: A nationwide cohort analysis using the minimum data set. J Am Heart Assoc. 2015;4(9):e002145.
Haynes HN, Gallek MJ, Sheppard KG, Drake KW, Ritter LS. Transitions of care for stroke and TIA. J Am Assoc Nurse Pract. 2015; 27(10):558-67.
Katzan IL, Spertus J, Bettger JP, et al. Risk adjustment of ischemic stroke outcomes for comparing hospital performance: A statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2014;45(3);918-44.
Nouh AM, McCormick L, Modak J, Fortunato G, Staff I. High mortality among 30-day readmission after stroke: Predictors and etiologies of readmission. Front Neurol. 2017;8:632.
Okere AN, Renier CM, Frye A. Predictors of hospital length of stay and readmissions in ischemic stroke patients and the impact of inpatient medication management. J Stroke Cerebrovasc Dis. 2016;25(8):1939-51.
Puhr MI, Thompson HJ. The use of transitional care models in patients with stroke. J Neurosci Nurs. 2015;47(4):223-34.
Reeves MJ, Hughes AK, Woodward AT, et al. Improving transitions in acute stroke patients discharged to home: The Michigan stroke transitions trial (MISTT) protocol. BMC Neurol. 2017;17(1):115.
Smith WS, Johnston SC, Hemphill JC. Cerebrovascular diseases. In: Kasper DL, Fauci AA, Hauser SL, Longo DL, Jameson JL, Loscalzo J, eds. Harrison’s Principles of Internal Medicine. 19th ed. New York, NY: McGraw-Hill Education; 2017.
Vahidy FS, Donnelly JP, McCullough LD, et al. Nationwide estimates of 30-day readmission in patients with ischemic stroke. Stroke. 2017;48(5):1386-88.
Wang G, Zhang Z, Ayala C, et al. Costs of hospitalization for stroke patients aged 18-64 years in the United States. J Stroke Cerebrovasc Dis. 2014;23(5):861-8.
ant12-CE Stroke-1127


















2 Comments.
Care transitions and planning for what can be done to avoid readmission is a very patient and care centered focus. Expanded discharge planning to include care-giver and family understanding and education, identifying proper resources and ensuring availability of those resources, follow up in the community, and strong educational tools for “what to expect” in the short AND long term are tantamount to a comfort level for the patient and family, and a better opportunity in achieving a low readmission rate.
This article is a good educational read because it emphasizes key components in providing holistic best practice care to patients with stroke. Registered nurses have the professional obligation to prevent stroke readmission as highlighted in the article. However, nurses should not underestimate the role family members play in recognizing the slightest change from the “new normal” of their loved one.
It is vital to create more awareness and to take the sooner-the-better approach to nip any sign or symptom that could propel the patient back to the hospital. Besides, family members should be encouraged to voice out any deviation to nursing staff without being perceived as a complainant