
Best practices to achieve good outcomes.
Takeaways:
- The most common complication of transradial access is radial artery occlusion.
- Ensuring flow through the radial artery while compressing for hemostasis is fundamental to protecting the radial artery from occlusion.
- The best practice for ensuring radial artery patency is performing the reverse Barbeau assessment.
Coronary angiography, with and without percutaneous coronary intervention, is one of the most common cardiac procedures performed in the United States. Although advances in technology, equipment, and techniques have decreased complications associated with cardiac catheterization to less than 1% of cases, the most frequent complications occur at the arterial access site. They include bleeding complications (hemorrhage, hematoma, and compartment syndrome) related to the puncture of a major artery and compromise to the blood vessel (pseudoaneurysm, arteriovenous fistula formation, clots, and limb ischemia).
In the 1970s, providers began using catheters and balloons (percutaneous intervention) to treat coronary artery stenosis. This minimally invasive treatment is now recognized as an effective treatment for many patients with coronary artery disease. Initially, many U.S. interventional cardiologists preferred using the femoral arteries in the groin for procedural access. Over the past decade, that trend has been changing since several multi-institutional, prospective, randomized studies (PREVAIL, STEMI-RADIAL, and RIFLE-STEACS) began comparing the transradial and femoral approaches. The studies demonstrated that, when performed by an experience operator, the transradial approach frequently results in better patient outcomes, including reduced mortality, cardiac events, and access site complications. Patients also prefer radial site access because it doesn’t require long bedrest and is more comfortable.
As radial access increases, more nurses in noncritical care settings will see these patients post-procedure. Increase your knowledge of the procedure, patient care, and potential complications to ensure the best outcomes.
Radial access recovery
In addition to fewer complications, radial access allows patients to sit up and eat soon after the procedure and to ambulate early. Most access sites heal quickly so patients can return to normal daily activities. However, explain to patients that they should avoid heavy lifting and aggressive exercise with the affected wrist for at least a few days.
Acute or chronic radial artery occlusion is the most common complication of transradial access, but many nurses overlook it. Because the hand receives blood from two arteries, occlusion of the radial artery may go undetected when the ulnar artery continues to perfuse blood. A systematic review and meta-analysis of 24 studies with 10,938 patients by Rashid and colleagues found a 7.7% incidence of radial artery occlusion within 24 hours of catheterization.
Patients may never know that they have a radial artery occlusion, but the complication remains a concern because it can leave the affected vessel unavailable for future catheterizations and may limit its use if the patient requires a graft for bypass surgery or radial arteriovenous fistula for dialysis. In some rare cases, the occlusion may compromise perfusion to the hand, resulting in numbness, tingling, pain, and possible damage to the fingers. (See Transradial access recovery.)
Transradial access recovery
Transradial access recovery has many aspects similar to femoral access recovery.
- Closely monitor the patient’s vital signs (heart rate and rhythm, respiratory rate, neurologic status, blood pressure, pulse oximetry, temperature, and pain level), noting significant changes from baseline and alerting the appropriate provider.
- Assess the access sites frequently (at least every 15 minutes for the first hour after the procedure) for bleeding and neurovascular complications.
- Visualize the site for bleeding, and palpate it to assess for hematoma (blood pooling beneath the skin).
- Ensure the site is dry and soft to palpation.
- If bleeding or hematoma occurs, apply manual compression, adjust the compression device, or notify the provider based on your organization’s policies.
- Distal to the procedure site, perform and document neurovascular (pulses, color, capillary refill, warmth and coolness, paresthesia) and pain assessments.
- Decreased pulses, extremity duskiness, prolonged capillary refill, coolness of the affected extremity compared to the unaffected, new paresthesia, and new moderate-to-severe pain may indicate decreased flow to the extremity and the need to decrease compression.
- Perform the reverse Barbeau test to confirm if assessment changes are due to artery occlusion.
- The patient’s hand may appear dusky, swollen, or cool due to the compression device inhibiting venous return. Elevate the affected arm on a pillow to promote venous return and enhance comfort.
- If you suspect radial artery occlusion, notify the provider or make adjustments to the compression device according to your organization’s policies.
Reducing occlusion risk
Nurses and interventional cardiologists have roles to play in reducing occlusion risk. Most interventional cardiologists use ultrasound and fluoroscopy to guide access, apply smaller hydrophilic sheaths, and administer anticoagulants and a cocktail of vasodilators through the site. Many providers apply a radial artery compression device when the hydrophilic sheath is removed at the end of the procedure. These devices, usually bracelet shaped, either clamp or have an air-filled bladder to maintain pressure on the access site. They remain on after the procedure while the anticoagulant (usually heparin) metabolizes and the site heals. The length of compression time and method of device removal depends on the type of device used, the patient’s anticoagulation status, physician preference, and organization policy. To avoid increased risk of occlusion associated with longer compression times, ensure the device is removed as ordered.
Nursing skills contribute to decreasing complication incidence during recovery. Evidence indicates that radial artery occlusion risk lessens when providers use a compression device to obtain patent hemostasis. The device should hold enough pressure to maintain hemostasis, or prevent bleeding and swelling, while also allowing blood flow through the vessel. Traditional site assessments can help you ensure the patient isn’t experiencing a bleeding complication; however, checking the radial pulse below the compression device isn’t enough to identify an occlusion. Because the radial and ulnar artery meet in an arch in the palm of the hand, you may detect a palpable radial pulse even when the radial artery is occluded.
The current best nursing practice to ensure patent flow through the radial artery includes a reverse Barbeau test. Perform the test when the patient enters recovery, frequently while the compression device is in place, after any device adjustments, and after removal. If your organization uses manual compression after radial procedures rather than compression devices, still perform a reverse Barbeau test after hemostasis and before discharge to rule out radial artery occlusion.
Reverse Barbeau test
The Barbeau and reverse Barbeau tests, objective versions of the traditional Allen’s test, assess for healthy flow in the individual arteries of the hand. The Barbeau test assesses for ulnar artery patency and the reverse Barbeau, performed in recovery, ensures radial artery patency. A study by Jirous and colleagues found the reverse Barbeau comparable to duplex ultrasound in identifying radial artery occlusion. You can perform the reverse Barbeau at the bedside without advanced technical training or complicated equipment. You need only pulse oximetry and knowledge. (See Reverse Barbeau test.)
Reverse Barbeau test

Follow these steps when performing the reverse Barbeau test:
- Place the pulse oximeter on the thumb or pointer finger of the procedural extremity.
- While watching the pulse oximetry waveform on the monitor, apply firm, occlusive pressure to the ulnar artery for no longer than 2 minutes. This allows ample time to assess for changes that may occur in the radial flow as ulnar compression itself may increase radial flow.
- While the ulnar is occluded, interpret the waveform using the Barbeau scale.
- Pulsatile waveform indicates radial artery flow.
- Flat waveform indicates radial artery occlusion.
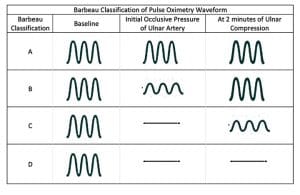
- Use the Barbeau classification to categorize and document the pulse oximetry waveform appearance:
- Category A: no change in waveform when opposite vessel is occluded (patent hemostasis).
- Category B: dampening of waveform with return to normal occurs within 2 minutes (patent hemostasis).
- Category C: flat line with return of waveform occurs within 2 minutes (patent hemostasis).
- Category D: flat line waveform without return of waveform within 2 minutes (indicative of radial artery occlusion; reduce compression device pressure and notify provider).
The time and method for removing radial compression devices vary by device and organization policy. Learn these policies to ensure prompt device removal. Shorter lengths of compression have been associated with decreased radial artery occlusion rates. After removing the device, reassess the reverse Barbeau and document artery patency. If the reverse Barbeau test indicates Category D (the pulse oximetry waveform is a flat line indicating occlusion), contact the provider immediately. Many providers will order a Doppler ultrasound to confirm an occlusion diagnosis. Prompt diagnosis and treatment can reverse most acute occlusions.
The future
Studies continue to identify methods for reducing radial artery occlusion risk, protecting the radial vessel, decreasing negative outcomes, and ensuring the artery remains healthy for use in future procedures. New compression devices provide simultaneous pressure on the radial and ulnar artery, which has shown evidence of increasing radial artery flow and decreasing occlusion rates.
As interventional cardiologists develop radial access skills during their initial training and the American Heart Association promotes a “radial-first” recommendation for acute coronary syndromes, radial access may become the primary arterial access choice. Other specialties—including interventional radiology and interventional neurology—also use transradial access. Understanding best practices and optimizing patient care will enhance positive experiences and improve outcomes.
Ellen Willock Moreno is a clinical nurse III at New York–Presbyterian Columbia University Irving Medical Center in New York, New York.
References
Barbeau GR, Arsenault F, Dugas L, Simard S, Larivière MM. Evaluation of the ulnopalmar arterial arches with pulse oximetry and plethysmography: Comparison with the Allen’s test in 1010 patients. Am Heart J. 2004;147(3):489-93. doi:10.1016/j.ahj.2003.10.038
Bernat I, Aminian A, Pancholy S, et al. Best practices for the prevention of radial artery occlusion after transradial diagnostic angiography and intervention: An international consensus paper. JACC: Cardiovasc Interv. 2019;12(22):2235-46. doi:10.1016/j.jcin.2019.07.043
Bernat I, Horak D, Stasek J, et al. ST-segment elevation myocardial infarction treated by radial or femoral approach in a multicenter randomized clinical trial: The STEMI-RADIAL trial. J Am Coll Cardiol. 2014;63(10):964-72. doi:10.1016/j.jacc.2013.08.1651
Bonnett C, Becker N, Hann B, Haynes A, Tremmel J. Preventing radial artery occlusion by using reverse Barbeau assessment: Bringing evidence-based practice to the bedside. Crit Care Nurse. 2015;35(4):77-82. doi:10.4037/ccn2015428
Jirous S, Bernat I, Slezak D, Miklik R, Rokyta R. Post-procedural radial artery occlusion and patency detection using duplex ultrasound vs. the reverse Barbeau test. Eur Heart J Suppl. 2020;22(suppl F):F23-9. doi:10.1093/eurheartj/suaa095
Manda YR, Baradhi KM. Cardiac catheterization risks and complications. StatPearls. 2022.
Mason PJ, Shah B, Tamis-Holland JE, et al. An update on radial artery access and best practices for transradial coronary angiography and intervention in acute coronary syndrome: A scientific statement from the American Heart Association. Circ Cardiovasc Interv. 2018;11(9):e000035. doi:10.1161/HCV.0000000000000035
Pancholy S, Coppola J, Patel T, Roke-Thomas M. Prevention of radial artery occlusion–patent hemostasis evaluation trial (PROPHET study): A randomized comparison of traditional versus patency documented hemostasis after transradial catheterization. Catheter Cardiovasc Interv. 2008;72(3):335-40. doi:10.1002/ccd.21639
Pristipino C, Trani C, Nazzaro MS, et al. Major improvement of percutaneous cardiovascular procedure outcomes with radial artery catheterization: Results from the PREVAIL study. Heart. 2009;95(6):476-82. doi:10.1136/hrt.2008.150714
Rashid M, Kwok CS, Pancholy S, et al. Radial artery occlusion after transradial interventions: A systematic review and meta-analysis. J Am Heart Assoc. 2016;5(1):e002686. doi:10.1161/JAHA.115.002686
Romagnoli E, Biondi-Zoccai G, Sciahbasi A, et al. Radial versus femoral randomized investigation in ST-segment elevation acute coronary syndrome: The RIFLE-STEACS (radial versus femoral randomized investigation in ST-Elevation acute coronary syndrome) study. J Am Coll Cardiol. 2012;60(24):2481-9. doi:10.1016/j.jacc.2012.06.017
Key words: radial artery, occlusion, transradial angiography, patent hemostasis, reverse Barbeau















