

In the healthcare arena, change happens at a rapid pace. Healthcare leaders face the continual challenge of delivering high-quality patient care while managing costs. A growing body of evidence shows that patient acuity-driven staffing is an effective way to optimize nurse staffing to improve patient outcomes and promote clinical and organizational excellence.
How do we turn that evidence into a transformative reality? On July 14, 2016, American Nurse Today and GE Healthcare cohosted a webinar that addressed that question. Four nurse leaders—all of them pioneers in acuity-based staffing research and implementation—presented a strong case detailing why acuity-based staffing is imperative, not just for patients and nurses but also for healthcare organizations as a whole. They offered practical guidelines on how nurses can foster change, both across the profession and within their local organizations.
Why should we examine the benefits of acuity-based staffing?
Currently, 14 states have legislation regarding nurse staffing in hospitals; some address nursepatient ratios, while others require various levels of reporting and accountability. This legislative momentum will likely continue, creating a legal impetus for healthcare organizations around the country to begin implementing more comprehensive staffing systems based on acuity. Acuity-based staffing is linked to a host of benefits, making adoption of data-driven acuity systems all the more compelling.
Positive clinical and operational outcomes linked to acuitybased staffing include decreases in mortality, adverse outcomes, and lengths of stay. “Acuitybased systems maximize patient and nursing outcomes through enhanced decision making, improved operational outcomes, and improved nurse and patient satisfaction—all while boosting financial performance through lower cost,” said Lillee Gelinas, MSN, RN, FAAN, webinar moderator and editor-in-chief of American Nurse Today.
Sophisticated acuity-based staffing systems can extract data pertaining to individual nurses caring for patients with variable needs, allowing a transparent examination of cost, quality, and performance. The data can then be integrated for better clinical and operational outcomes. According to Karlene M. Kerfoot, PhD, RN, NEA-BC, FAAN, chief nursing officer at GE Healthcare, “If we don’t recognize the variability [in patient care]…and provide the kinds of resources that can match a patient’s needs to an RN’s competencies—and do it within a healthy environment—we won’t be able to get the kinds of outcomes we desperately need to improve our healthcare system.”
Acuity-based staffing and nursing hours
Determining how to measure nursing care has been a persistent challenge for our profession. Often, nursing is seen as a cost center, not a core service. Healthcare organizations are reimbursed for medical care based on a diagnosis or procedure, but current payment systems don’t account for nursing care differences.
Patient acuity levels in acute-care settings have increased. What’s more, patients are being discharged from hospitals at a faster pace than ever, which increases the intensity of care each patient requires. Combined with the wide range of patient variability—even within the same patient population—this has made nursing care needs much more difficult to ascertain objectively. Patient acuity data offer transparency that allows accurate calculation of how many nursing hours are needed in a given situation.
John Welton, PhD, RN, FAAN, professor at the University of Colorado College of Nursing and senior scientist for Health Systems Research, shared data he presented at the 46th annual American Organization of Nurse Executives Conference, along with findings that show the calculation of direct-care hours and the cost of those hours for each patient on a medical-surgical floor. Patients who stayed 1 day had a much higher average of care need (in mean hours) than those who stayed 2, 3, or 4 days. Also, patients who stayed more than 3 weeks required more care on average. Although these patients made up only 20% of the patient population, they required 50.4% of all available nursing care hours and dollars. Additionally, patients aged 65 and older (the Medicare population) required 30 to 45 minutes more nursing care per day.
Acuity-based staffing and mortality
Jack Needleman, PhD, FAAN, professor and chair of the Department of Health Policy and Management at UCLA’s Fielding School of Public Health, presented findings from a 2011 article he coauthored, which reported results based on data collected from a large academic medical center that implemented a patient-acuity staffing system. The analysis showed a substantial increase in mortality during nursing shifts that fell 8 hours or more below target staffing levels—essentially one nurse short. When the researchers looked at patient turnover separately, they found patient mortality increased when staffing wasn’t adjusted for higher turnover rates.
Acuity-based staffing and adverse outcomes
Acuity-based staffing is linked to decreased adverse events, including falls, infections, and pressure ulcers. A study by Pappas et al. of a transplant unit identified patient risk factors that indicate a higher acuity level. A patient score of 4 or higher indicated the need for a lower nurse-to-patient ratio assignment to accommodate increased nursing time or intensity.
These risk factors include:
• organ transplant (kidney, liver, pancreas, or a combination) received on current admission (score of 2)
• hepatic failure (score of 2)
• gynecologic surgical post-operative patient during the first 12 to 24 hours (score of 2)
• high fall risk and age older than 78 (score of 2)
• transplant patient in isolation (score of 1)
• transplant patient readmission (score of 1).
The researchers also measured four nurse-sensitive indicators and compared them to a national database of similar inpatient units. The indicators included falls incidence, catheterassociated urinary tract infections, central line–associated bloodstream infections, and pressure-ulcer prevalence. Rates for all four indicators decreased after staffing was adjusted to account for higher-acuity patients. Study findings also showed decreased overtime hours and reduced costs per case. Clinical nurses attributed decreased overtime to having adequate time during the shift to complete their work.
Making the business case for acuity-based staffing
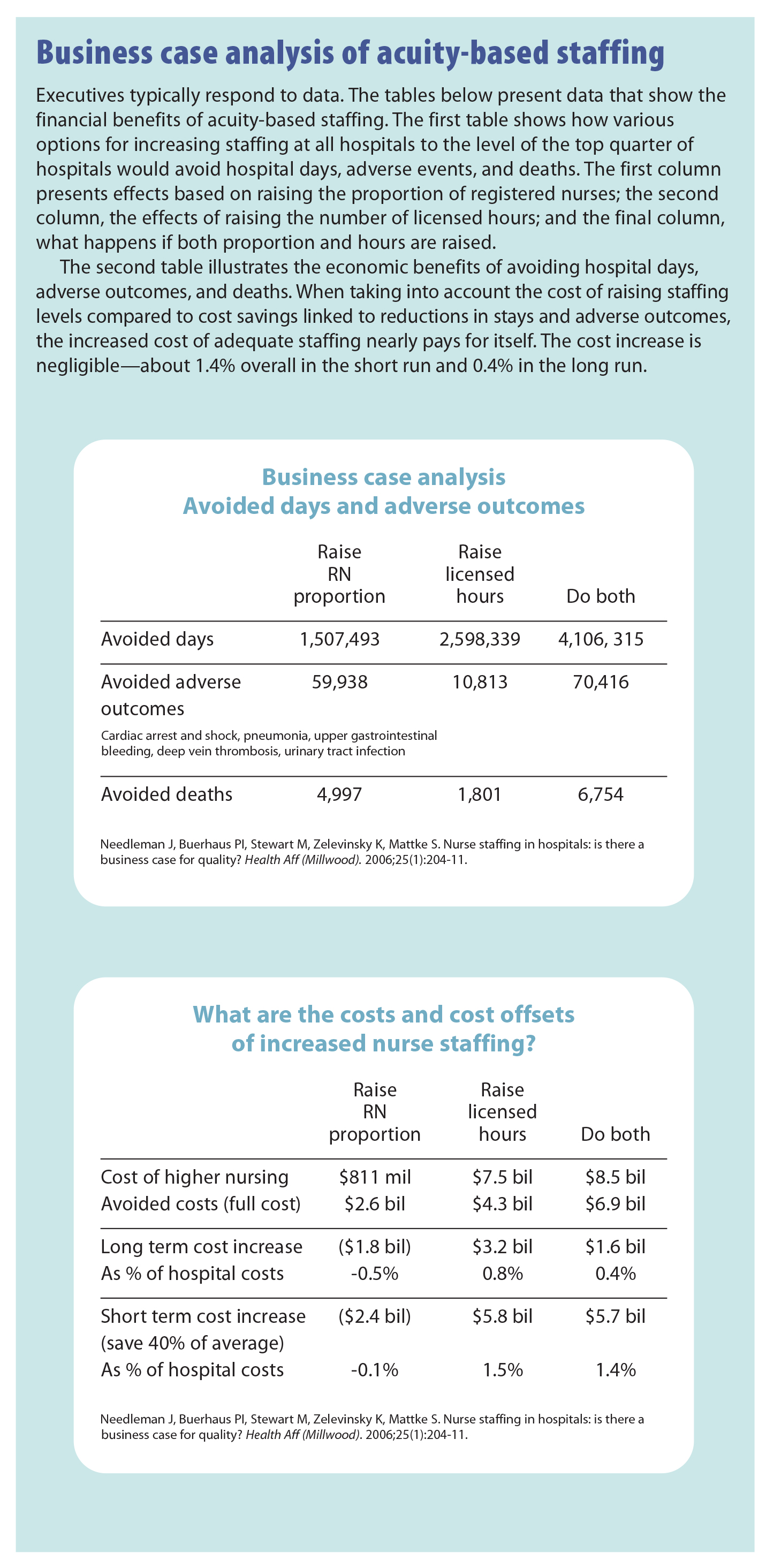
Needleman emphasized that the cumulative effects of the benefits of avoided hospital days, avoided adverse outcomes, and avoided deaths make a powerful business case for acuity-based staffing systems. He cited data from a classic analysis that found such systems bring significant financial advantages to organizations. (See Business case analysis of acuity-based staffing).
In a healthcare environment where payment structures let hospitals retain savings gained by maximizing cost efficiencies while meeting quality standards, nurse leaders can help executives understand the advantages of acuity staffing to the organization’s bottom line.
Criteria for evaluating an acuity-based staffing system
An important factor in deciding which acuity-based staffing system to adopt is how much time and effort implementation will require. Optimally, the system should carry a minimal additional workload requirement.
As a vice president and system chief nursing officer, Sylvain Trepanier, DNP, RN, CENP, helped lead adoption of an acuity- based staffing system at Premier Health, a not-for-profit multihospital system in Southern Ohio with 14,000 employees and more than $1.6 billion in revenue. One of his key aims was to find a system that fit seamlessly into the organization’s workflow—one in which “we could leverage what’s in our electronic health record [EHR] as it relates to nursing documentation and treatment orders, patient placement, medication administration, and all of the activities documented in the health record that show what’s going on with the patient, up to and including transfers, admission, and discharge.” Premier Health was able to find a user-friendly commercial system that incorporated timely, actionable data—something that could be acted upon on an hourly basis.
The staffing system should be built on a foundation of expert nursing judgment and should reflect the nursing work. “Nurses understand their care better than anybody else,” Needleman explained.
Indicators that affect staffing
Another factor to consider when choosing an acuity-based staffing system is to ensure that the indicators measure patient complexity and required nursing care. To evaluate this, leaders need to consider several variables identified in the literature when determining adequate staffing. These variables fall into three major categories: patient needs, nurse characteristics, and unit and organizational factors.
Patient needs
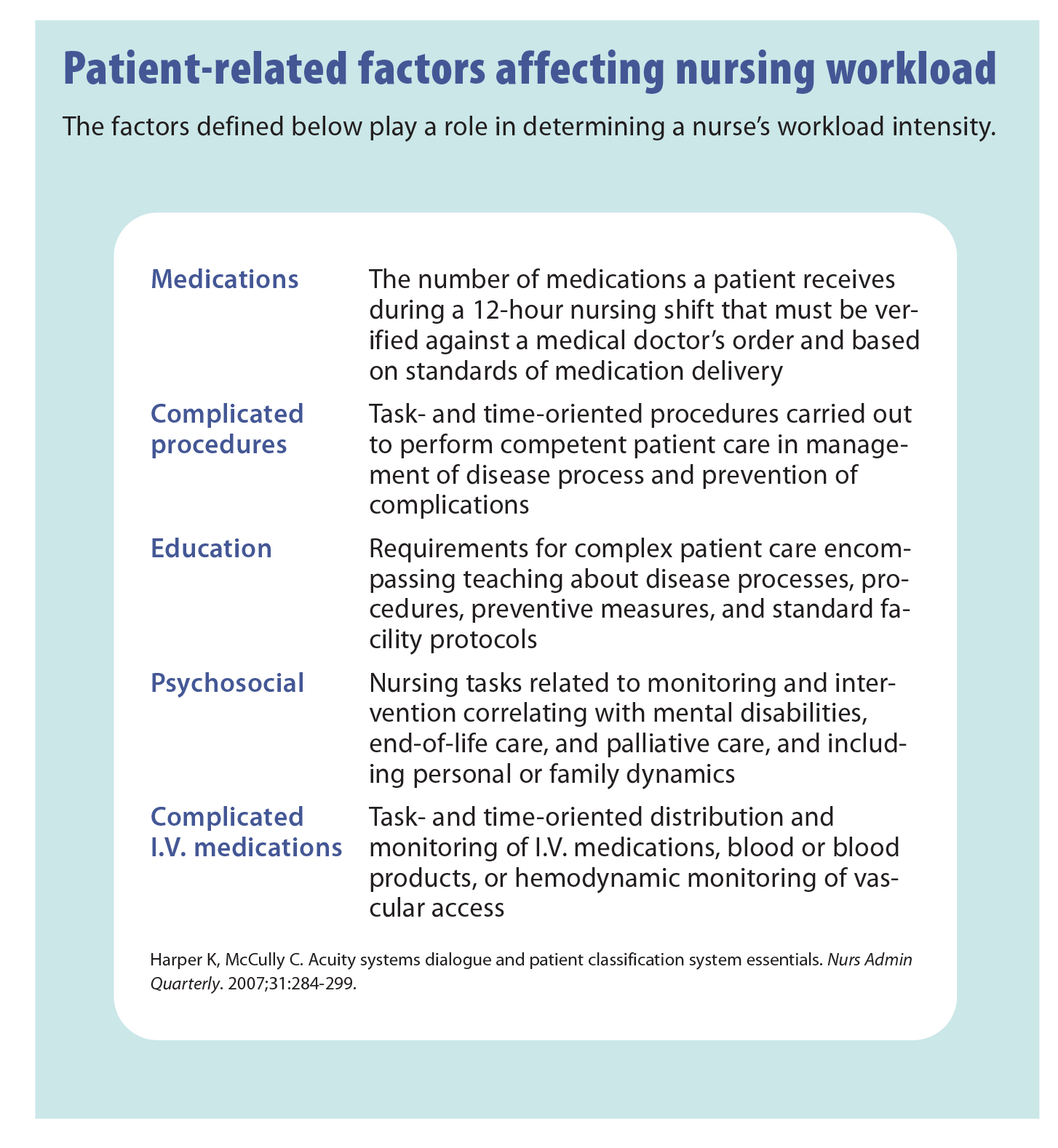
To a large extent, patient variables naturally drive staffing needs. Emphasis should be placed not just on disease or status but also on outside factors that influence acuity—patient complexity, length of stay, functional status, activities of daily living, need for transport, and age. All of these play a role in determining the patient’s nursing care needs. Several additional items also affect nursing workload intensity. (See Patient-related factors affecting nursing workload.)
Nurse characteristics
Nursing staff characteristics must be taken into account. A particular nurse’s training, education, and skills should be matched with the needs of a particular patient.
Unit and organizational factors
These factors may include workflow processes, documentation expectations for nursing staff, physical layout of the floor, and existing support, including nursing assistance and stocking of supplies.
Commercial vs. local systems
A key decision organizations face when choosing an acuitybased staffing system is whether to use a commercial system, as Premier Health did, or develop one locally. Both options have advantages and drawbacks. The biggest advantage of commercial systems is that they offer an already developed algorithm that potentially can be tailored to the local nursing model. Commercial systems typically include modules that allow direct tracking of actual vs. target indicators to see how those indicators affect patient processes.
However, many commercial systems have a high data-entry burden, although this can be mitigated by linkage to the EHR (a feature vendors increasingly are working to accommodate). Also, these systems typically focus on patient need and don’t take into account patient turnover and the associated increase in nursing workload intensity.
Local systems, on the other hand, can be adjusted for local patient variation on specific units or adapted to incorporate variability the nursing staff considers relevant—for instance, patient turnover. But they also can impose a data-entry burden if no linkage exists to track data entry and storage, which means data must be collected by hand.
During rollout of a new acuity-based staffing system, Trepanier emphasized, shared governance and having significant support in place are crucial for making the process as seamless as possible. He recommended that those responsible for implementing the system identify and address resistance to change early and incorporate the system slowly from one service area to the next rather than taking a “big bang” approach.
Call to action
Optimal staffing is linked to clinical and organizational excellence. Rigorous evidence is emerging to support acuitybased staffing as way to provide consistent, high-quality care while managing financial burden. Nationally, legislation mandating acuity-based staffing is increasing, and union contracts are starting to consider the role of acuity-based staffing as well. As a result, healthcare organizations will likely have difficulty ignoring the move away from census- or opiniondriven staffing toward acuity-driven systems.
The onus now lies on nursing leadership, with many opportunities to help push for change. Externally, nurses can commit to supporting research surrounding acuity-driven staffing and disseminating that work through presentations and publications. They can support professional nursing organizations that are spearheading change. For instance, the American Nurses Association is developing white papers to help educate nurses and support the movement.
Internally, nurse leaders need to support a move away from opinion-based acuity staffing toward data-driven acuity-based staffing. This will require educating teams, management, and chief executives about the potential for data-driven staffing to improve patient care and control cost. “Historically, many have been suspicious of acuitydriven staffing,” said Kerfoot, “because it has been opinion based. But that’s not the case now. We have to help people understand this isn’t the acuity system of 20 years ago. Today’s data-driven systems make an incredible difference.”
Kerfoot urges nurses, particularly nurse leaders, to advocate for data-driven acuity-based staffing technology and to empower nursing to leverage the EHR investment and use robust data that will bring a significant return on investment.
Nurse leaders must stay well informed to ensure that a nursing voice is already at the table when workforce staffing technology decisions are being considered.
Acuity-based staffing isn’t just a way to achieve better patient outcomes. It’s also an opportunity to demonstrate the significant value nursing contributes to patient care. Trepanier pointed out, “If we don’t have the data to demonstrate the hard work—the practice and influence we make in light of those we serve—we won’t be able to appropriately demonstrate our value contribution.”
Meaghan O’Keeffe is a freelance healthcare writer and clinical editor based in Framingham, Massachusetts.
Editor’s note: Access a recording of the webinar.
Selected references
Harper K, McCully C. Acuity systems dialogue and patient classification system essentials. Nurs Adm Q. 2007;31(4):284-99.
Needleman J, Buerhaus P, Pankratz VS, Leibson CL, Stevens SR, Harris M. Nurse staffing and inpatient hospital mortality. N Engl J Med. 2011;364(11):1037-45.
Needleman J, Buerhaus PI, Stewart M, Zelevinsky K, Mattke S. Nurse staffing in hospitals: is there a business case for quality? Health Aff (Millwood). 2006;25(1):204-11.
Pappas S, Davidson N, Woodard J, Davis J, Welton JM. Risk-adjusted staffing to improve patient value. Nurs Econ. 2015;33(2):73-8.
Welton JM, Caspers B, Sanford K. Inpatient nursing hours and cost outcomes within a health care system. American Organization of Nurse Executives 46th Annual Conference. March 2013, Denver, Colorado.















{kind=link}
{kind=link}