

Best practices for residents living in long-term care
Takeaways:
- A growing body of evidence supports the idea that personhood and selfhood are not lost even in advanced dementia.
- Person-centered dementia care can significantly reduce behavioral disturbances, specifically aggression and agitation.
- Person-centered care can be mutually beneficial for staff and patients.
According to the Alzheimer’s Association, approximately 5.7 million Americans have Alzheimer’s dementia, and that number is expected to grow. The progressively debilitating nature of the disease causes patients to lose the ability to live independently, so many rely on long-term care services. In the United States, about 1.4 million residents live in long-term care facilities; 50.4% of them have been diagnosed with dementia.
To receive Medicare and Medicaid funding, long-term facilities must comply with federal regulations that require them to promote residents’ quality of life and to preserve their dignity and self-determination. This includes allowing residents the opportunity to participate in the development and implementation of a person-centered care (PCC) plan.
What is PCC?
PCC incorporates knowledge and recognition of an individual’s life history, beliefs, values, needs, and preferences as the central influences on how caregivers interact with them. Personhood and selfhood are fundamental to PCC.
Personhood is a standing or status bestowed on an individual by others. Personal affirmation provided by relationships with others is essential for maintaining personhood.
Selfhood is defined as the attributes, characteristics, beliefs, and desires of the self. It also includes an individual’s roles and how they present themselves publicly. For those with dementia who live in long-term care, staff members can provide these personal affirmations. Lack of support for personhood can damage a vulnerable person’s self-esteem and lead to loss of selfhood.
Best practices in dementia care
A growing body of evidence suggests that personhood and selfhood aren’t lost in dementia. Behaviors that were once thought to be solely the result of dementia’s neuropathology are now viewed as a complex interaction with socio-psychological factors. Evidence from the Crisis Prevention Institute indicates that individuals with dementia maintain abilities at every stage of the condition. Those abilities can be used to maximize function and well-being and to promote social and leisure activities that positively impact activity levels and mood. Behaviors such as wandering, agitation, and resistance to care aren’t viewed as normal manifestations of dementia, but rather as expressions of a problem that can be minimized with best practices.
Ensuring quality of life for people with dementia begins with having accurate knowledge about the disease and an understanding of PCC principles.
- Recognize that people with dementia continue to express aspects of themselves (selfhood) in many ways, even as dementia progresses.
- Emphasize understanding behavior rather than managing it.
- Allow residents to exercise choice, use their abilities, express their feelings, and develop and maintain relationships.
- Make PCC the foundation to quality care.
Implementing best practices must include staff training. However, changing attitudes and beliefs about individuals with dementia can be challenging. Storytelling techniques actively engage staff in the experiences of others by asking them to imagine, embrace, listen to, and connect with the person who has dementia. “Let’s talk about it” (era.lib.ed.ac.uk/handle/1842/6559) is a downloadable toolkit that can be used for this type of staff training.
PCC benefits
Systematic review and meta-analysis of current evidence indicate that adopting a PCC approach can benefit long-term care facility residents and staff.
Resident benefits
Studies, including one by Chenoweth and colleagues, show that PCC can significantly reduce behavioral disturbances (such as aggression and agitation) and neuropsychiatric symptoms of dementia. When these behaviors are reduced, use of psychotropic medication also can be reduced, which aligns with the Centers for Medicare and Medicaid Services’ goal to decrease unnecessary use of antipsychotic medications in long-term care facilities.
Staff benefits
PCC training and education prepares staff to respond more effectively to the challenging situations that can occur when caring for residents with dementia. The result is lower staff stress and burnout and higher job satisfaction. However, according to Moyle and colleagues, staff who practice PCC will need opportunities to reflect on and deal with their emotions, workload, and time management. Support systems should be implemented to assist staff with balancing increased engagement with residents while maintaining professional boundaries.
PCC strategies
Many strategies can help caregivers implement PCC. Some of the most common approaches (and recommended resources) are described below.
Know the person
Life story work involves working with a resident and their family members to learn about the person’s life, recording that information in some way, and then incorporating it into the resident’s care.
Reminiscence therapy, frequently conducted in informal settings with other residents, involves sharing autobiographical memories. Themes to explore include food and cooking, family relationships, early memories, jobs, music, celebrations, and losses. (See Sample life story questions.)
Sample life story questions
To learn more about a resident’s life story, consider asking these questions.
- Can you tell me about your school days when you were a child?
- Who was important to you when you were growing up?
- What was it like growing up where you lived?
- What music did you listen to, and what music do you like now?
- Can you tell me about your first movie? First date? First job?
- Can you tell me about important life celebrations, such as birthdays, holidays, and graduations?
- Can you tell me about a difficult time in your life and how you adjusted?
- How would you like to be remembered?
To capture reminiscence activities, consider recording them in a life storybook (hard copy or digital), a written summary, or a memory box. The resident and family can use these to talk about life experiences, which will provide staff with insight into residents’ personal interests, values, beliefs, and culture. Hearing a resident’s life story can help staff see the person as an individual and develop a deeper relationship. Reconstructing and recording narratives from fragments of stories told over time by the resident with dementia also can help staff members get to know the person.
Recommended resources: Arts-and-crafts supplies and interview questions. Much of the information needed can be obtained in the admission and care planning process.
Effective communication
Staff may think that they don’t know how to communicate effectively with people who have dementia. They also may assume that someone with dementia can’t communicate or that it takes too much time. This sets the stage for nonengagement, which perpetuates withdrawal by both the resident and the caregiver, leads to caregiving without communicating, and prevents relationship building. Difficult behavior frequently is the result of miscommunication and unmet needs, leading to a cycle of misunderstandings and more difficult behavior. Breaking this cycle improves everyone’s quality of life and reduces the need for psychotropic drugs. (See Communication tips.)
Communication tips
Use these tips to communicate effectively with residents who have dementia.
- Always attempt to find the meaning of a resident’s behavior. For example, boredom and frustration frequently are communicated through behavior. In patients with more advanced dementia, behavior can signal unmet needs such as being cold, hungry, or frightened.
- Remember that communication is more than words. It includes gestures, body posture, and movements, which can be misinterpreted by people with dementia.
- Explain what you’re going to do before touching a resident, and give them time to respond.
- If the environment is too stimulating, some residents may need to withdraw to a quiet area.
- Knowing the person helps you understand their behavior.
- Try not to take bad behavior personally or judge it.
- Don’t use force to control a patient’s behavior.
- Keep in mind that communication is never a waste of time, even if you have other things to do.
Recommended resources: Stephen Miller’s Communicating Across Dementia: How to Talk, Listen, Provide Stimulation, and Give Comfort can be purchased as an e-book. This low-cost resource is easy to use for all levels of staff development training, including housekeeping, dietary, and nursing.
Concept mapping
A concept map is a visual representation of ideas or knowledge, including the links between them. It involves a person-centered assessment and problem-solving approach to managing behavioral and psychological symptoms of dementia. When completed by an interprofessional team (nurses, pharmacists, and occupational, physical, and recreational therapists), concept mapping can effectively identify what’s known and unknown so the team can get a new perspective for providing the best care.
Concept mapping starts with writing all available information and assessment data on a board, using predetermined categories (such as life history, dementia stage and current behaviors, health status, communication ability, and environment). Categories can be individualized as needed. After mapping is completed, missing information and links between categories become apparent. The goal is to understand the behavior and identify unmet needs so the team can develop individualized care strategies. (See Concept mapping in action.)
Concept mapping in action
These examples of residents (names are fictitious) in long-term care illustrate how concept mapping can help staff implement person-centered care (PCC).
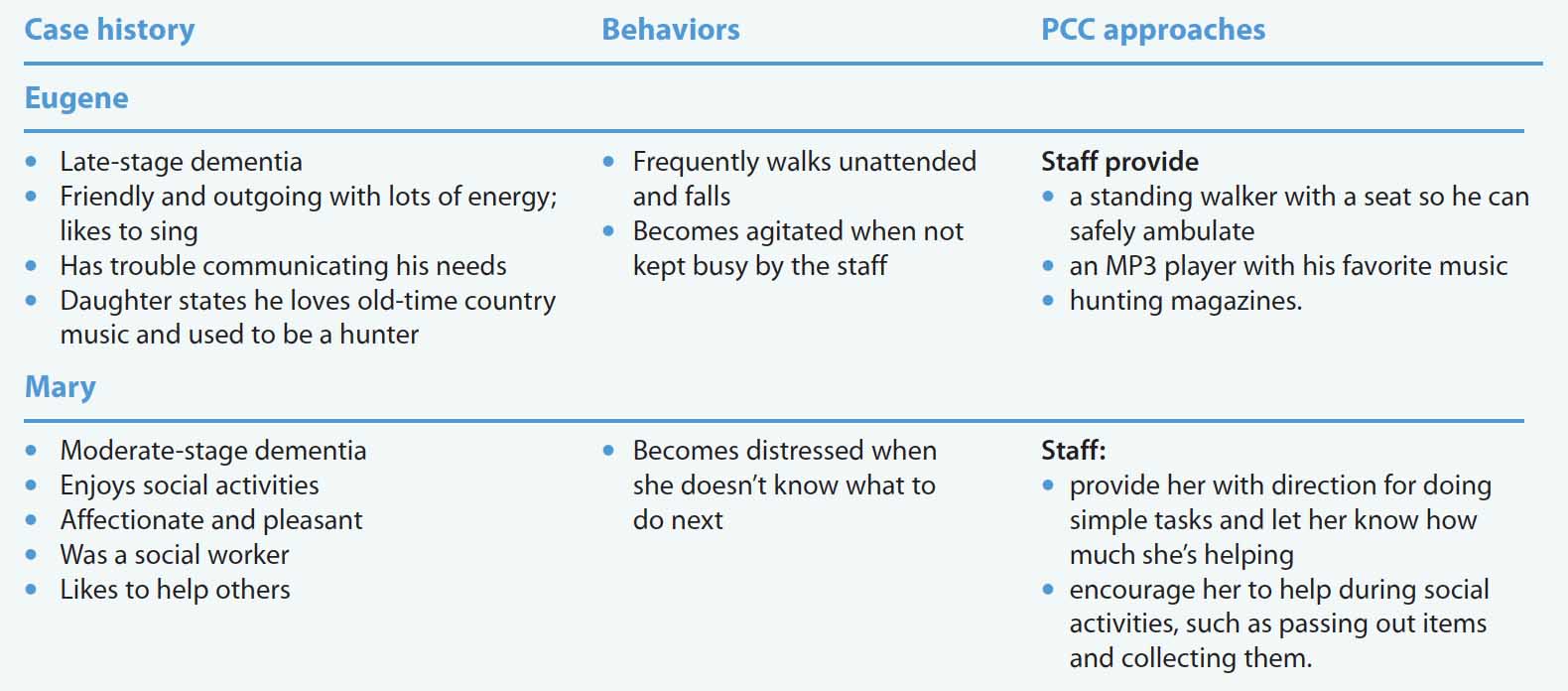
Recommended resources: Team meeting, patient information, white board, and markers.
Environment and activities
Multisensory environments that support sensory therapeutic activities are recommended for individuals in all dementia stages. Having a variety of activities that can be self-chosen supports personhood rather than using a one-size-fits-all approach. Activities can include drama, art, music, and dance. Some residents may enjoy hand massage and aromatherapy. Everyday tasks within a resident’s abilities—such as making coffee, setting and clearing a table, cleaning, pairing socks, or watering plants—are associated with resident quality of life in long-term care. Providing dusters, dolls, soft toys, handbags, jewelry, musical instruments, bubbles, and puppets can spark interest and engagement.
Recommended resources: Donations of items can be sought from groups such as the Girl Scouts, places of worship, and families. Therapists can help evaluate individual residents’ personal abilities to promote the highest level of function.
Make the commitment
PCC is an expected standard of care, but it can be difficult to maintain. Effectively influencing the attitudes and behaviors of staff about PCC can be challenging, as can restructuring the work environment and culture. Successfully implementing PCC requires a commitment by all stakeholders, which includes providing further education and adequate resources to develop, deliver, and sustain the practice.
Gloria Brandburg is lead faculty at Franklin University in Columbus, Ohio. Josie Tombrella is an assistant professor in the school of nursing at the University of Texas Medical Branch in Galveston.
References
Aberdeen SM, Byrne G. Concept mapping to improve teamwork, team learning and care of the person with dementia and behavioural and psychological symptoms. Dementia (London). 2018;17(3):279-96. doi: 10.1177/1471301216641785
Alzheimer’s Association. 2019 Alzheimer’s disease facts and figures. Alzheimers Dement. 2019;15(3):321-87. https://www.alz.org/media/documents/alzheimers-facts-and-figures-2019-r.pdf
Björk S, Lindkvist M, Wimo A, Juthberg C, Bergland Å, Edvardsson D. Residents’ engagement in everyday activities and its association with thriving in nursing homes. J Adv Nurs. 2017;73(8):1884-95. doi:10.1111/jan.13275
Chenoweth L, Jeon Y-H, Stein-Parbury J, et al. PerCEN trial participant perspectives on the implementation and outcomes of person-centered dementia care and environments. Int Psychogeriatr. 2015;27(12):2045-57. doi:10.1017/S1041610215001350
Crisis Prevention Institute. Person-centered dementia care: Warchol Best-Abilities Care Model. March 15, 2019. crisisprevention.com/Blog/April-2019/Person-Centered-Dementia-Care-the-Warchol-Best-Ab
Dementia Care Matters. The feeling of mattering really matters in dementia care. Dementiacarematters.com
Electronic Code of Federal Regulations. Requirements for long-term care facilities: Residents rights. 42 C.F.R. §483.10. ecfr.gov/cgi-bin/text-idx?node=pt42.5.483&rgn=div5#se42.5.483_110
Fazio S, Pace D, Flinner J, Kallmyer B. The fundamentals of person-centered care for individuals with dementia. Gerontologist. 2018;58(S1):S10-9. doi:10.1093/geront/gnx122
Kim SK, Park M. Effectiveness of person-centered care on people with dementia: A systematic review and meta-analysis. Clin Interv Aging. 2017;12:381-97. doi:10.2147/CIA.S117637
McKinney A. The value of life story work for staff, people with dementia and family members. Nurs Older People. 2017;29(5):25-9. doi:10.7748/nop.2017.e899
Miller S. Communicating Across Dementia: How to Talk, Listen, Provide Stimulation, and Give Comfort. London: Little Brown Book; 2015.
Moyle W, Venturato L, Cooke M, et al. Evaluating the capabilities model of dementia care: A non-randomized controlled trial exploring resident quality of life and care staff attitudes and experiences. Int. Psychogeriatr. 2016;28(7):1091-1100. doi:10.1017/S1041610216000296
Sakamoto ML, Moore SL, Johnson ST. “I’m still here”: Personhood and the early-onset dementia experience. J Gerontol Nurs. 2017;43(5):12-7. doi:10.3928/00989134-20170309-01
















