

Pre-hospital professionals can help ease workload demands.
- Paramedic training includes multi-tasking, working autonomously, and working under tremendous pressure, all skills critical to working in the emergency department setting.
- Paramedics can play an essential role as healthcare evolves and organizations struggle to meet an increasing health demands in the midst of a nursing shortage.
- Opportunities for quantitative and qualitative studies exist related to paramedics transitioning into alternative worksites and the benefits they can provide in emergency departments.
As nursing shortages around the United States continue to grow, including in emergency departments (EDs), hospital systems seek innovative solutions. Some systems have resorted to paying high salaries for travel nurses or increasing patient–nurse ratios to maximize staffing matrixes. In North Carolina, a free-standing ED has hired paramedics to help supplement its nursing staff and alleviate some of the pressure.
Palliative care in the emergency department
Drifting in the sea of an emergency department
Improving the nursing work environment
Paramedic scope of practice
Employing paramedics in the ED setting isn’t new, but allowing them to function at their full scope of practice is uncommon and in some cases has proven controversial. (See History of paramedics in the ED.)
Paramedics have a much broader scope of practice than nurses may realize and are skilled in performing advanced life-saving procedures. However, when employed in the ED setting, frequently they’re assigned duties more closely aligned with nurse aide responsibilities, such as obtaining vital signs, performing finger sticks, and drawing I.V. blood samples.

History of paramedics in EDs
Paramedics have been working in emergency departments for years, but many have considered this practice controversial. In 1992, for example, the American Nurses Association (ANA) issued a position statement on the subject, which read in part, “Regulatory entities have been pressured to lower agency staffing standards, for instance, by allowing emergency medical technicians to function in the emergency room without registered nurse supervision or by substituting unlicensed personnel for licensed nurses. These unlicensed persons have not completed nursing education programs or met other licensing requirements. In many instances, substitutions of unlicensed personnel for licensed nurses clearly violates state nurse practice acts. At the very least, it is not in the interest of the health, safety, and welfare of the public.”
In 2015, the Texas Emergency Nurses Association adamantly opposed two state bills that proposed allowing paramedics to function at their full scope of practice in the ED setting. Citing safety, the association expressed concerns about the ability of paramedics to safely operate under the supervision of a physician from inside the hospital and encouraged members of the state legislature to vote no on the bills.
Those Texas bills eventually passed, and in 2014, ANA issued the Essential Principles for Utilization of Community Paramedics, which provides standards and strategies for RNs and community paramedics cooperating in various settings and across the continuum of care. The document acknowledges overlapping care responsibilities and minimum standards of education and training for community paramedics that prepares them to perform expanded functions. Read the full document at bit.ly/3RIu9TU.
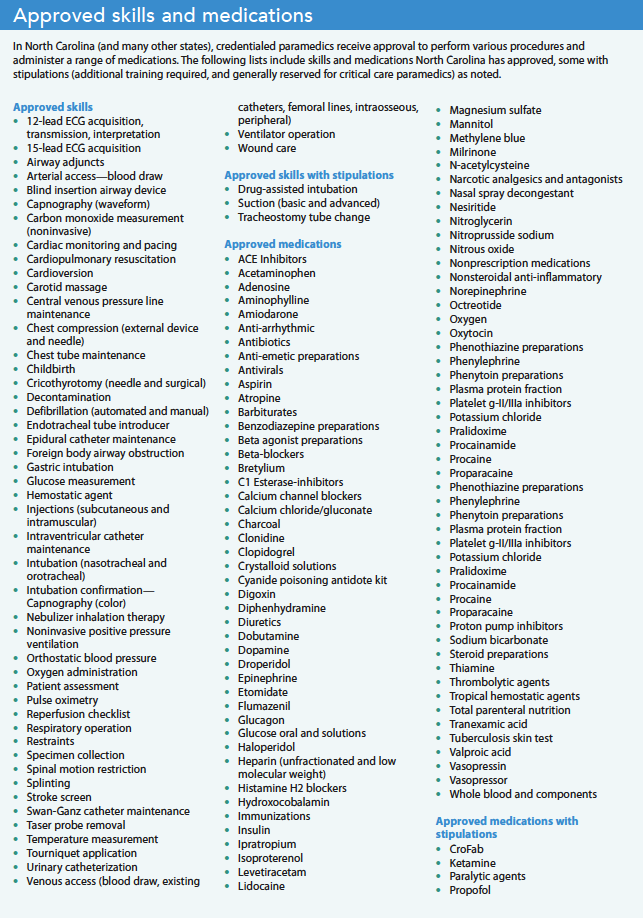
Individual states set paramedic scopes of practice, but in North Carolina, paramedics frequently play a role in advanced pre-hospital care. For example, hospital-based air medical teams employ paramedics to work alongside emergency nurses on critical care transport helicopters and ambulances. In many instances, the paramedic shares most of the same job responsibilities as the nurse. In 2019, the North Carolina Board of Nursing and the North Carolina Office of Emergency Medical Services issued a joint position statement on alternative practice settings for paramedics. The statement highlighted that the RN must always remain responsible and accountable for all aspects of nursing care when collaborating within an interprofessional team. It stated that paramedics are restricted to performing within their scope of practice defined by the North Carolina Medical Board and must perform under the protocols and policies of the practice setting. (See Approved skills and medications.)
Paramedics in the ED
In mid to late 2021, our ED hired one part-time and two full-time paramedics to complement staff nurses from 3 pm to 3 am. The urban, 12-bed, not-for-profit ED sees patients of all ages, but primarily adults over 18. The facility provides treatment for various illnesses and injuries and is staffed by experienced emergency physicians, nurses, technicians, respiratory therapists, and now paramedics. They see approximately 35,000 patients annually. The move to hire paramedics resulted from two main factors: the influx of patients during the last peak of COVID-19 and high staff turnover. The strain of increased patient volume combined with fewer staff nurses led to decreased patient satisfaction scores, longer patient wait times, and exhausted nurses.
Initially, hiring the paramedics resulted in some confusion and hesitation. Clinical nurses weren’t familiar with paramedic scope of practice, and the paramedics felt uncertain about expectations for their role. In the beginning, paramedics primarily initiated I.V. access and drew blood samples or helped the triage nurse obtain patient height, weight, and vital signs. Although well within the paramedics’ scope of practice, these fundamental skills didn’t take advantage of their full abilities.
As training continued the role of paramedics in the ED evolved. For example, they administer medications within their scope of practice, obtain lab specimens, and occasionally are assigned patient rooms while under the direct supervision of an RN. Because paramedics aren’t assigned specific patients, they can float and assist nurses throughout the department.
Similar to staff nurses, the paramedics fall under the medical direction of the hospital and ED, so they can complete physician orders when entered into the electronic health record. Allowing paramedics to work within their full scope of practice permits nurses to focus on patient-specific initiatives such as triage, assessments, medication education, and discharge instructions.
Wins and challenges
The results of this initiative have been overwhelmingly positive. After only a short few months, paramedics have become valuable and essential partners in the ED workflow. As with all nursing specialties, emergency nurses frequently have to juggle multiple priorities, and the paramedics provide an extra level of support. We have plans to hire more paramedics so we can staff the positions around the clock. Other EDs in the area have taken notice of our success and have implemented similar strategies.
However, some confusion still exists. For example, although paramedics can perform an extensive range of skills and administer several medications in North Carolina, that doesn’t always translate into an individual paramedic’s comfort level. Nurses shouldn’t expect that all paramedics feel comfortable administering all medications, and paramedics shouldn’t feel ashamed or embarrassed to admit when they’re uncomfortable. Open dialogue among nurses and paramedics helps to address this issue.
All available resources
According to a report in the World of Irish Nursing & Midwifery, the effects of the pandemic on nurses (moral injury, trauma, stress, physical illness, and post-traumatic stress disorder) may increase the projected worldwide shortage of six million nurses in 5 years to 13 million. The nursing profession may be in trouble, and any future discussions related to innovative strategies to alleviate emergency nursing shortages that don’t involve paramedics ignore an untapped potential for highly qualified and skilled medical professionals who may desire a transition from pre-hospital to in-hospital patient care.
Nurses will never be replaced, but as a profession we must do what’s right to ensure quality patient care. This includes using our strength as leaders to guide interprofessional care using all available resources, including paramedics and other pre-hospital providers.
Randy Hamm is an associate professor of nursing at Barton College in Wilson, North Carolina, and clinical staff nurse IV at WakeMed Health and Hospitals in Raleigh, North Carolina. David Allsbrook is a clinical educator and supervisor at WakeMed Health and Hospitals in Garner, North Carolina.
References
American Nurses Association. ANA’s Essential Principles for Utilization of Community Paramedics. March 2014. bit.ly/3RIu9TU
Blau G, Chapman S. Why do emergency medical services (EMS) professionals leave EMS? Prehosp Disaster Med. 2016;31(S1):S105-11. doi:10.1017/S1049023X16001114
Boland LL, Kinzy TG, Myers RN, et al. Burnout and exposure to critical incidents in a cohort of emergency medical services workers from Minnesota. West J Emerg Med. 2018;19(6):987-95. doi:10.5811/westjem.8.39034
Clarke A. What are the clinical practice experiences of specialist and advanced paramedics working in emergency department roles? A qualitative study. Br Paramed J. 2019;
4(3):1-7. doi:10.29045/14784726.2019.12.4.3.1
Moore A. Covid has proven nurses’ worth. World of Irish Nursing & Midwifery. 2022;30(5):23.
United States Department of Transportation. EMS workforce for the 21st century: A national assessment. June 6, 2008. rosap.ntl.bts.gov/view/dot/16483
American Nurse Journal. 2023; 18(3). Doi: 10.51256/ANJ032336
Key words: paramedics, nursing shortage, emergency departments, patient surges
















2 Comments. Leave new
very informative
Before becoming a nurse, I worked as a paramedic in the ED. I think the nurses I worked with appreciated the help paramedics could provide. There was confusion as to understanding what paramedics could do for the nurses regarding medications, procedures, etc. This could be alleviated by training nurses and paramedics during onboarding to help understand the scope of practice. Additionally, in Colorado where I worked, our scope of practice was dictated via a set of protocols signed off by the physician who worked as our medical director since the paramedic works under the physician’s license, not the nurse’s license. This is similar to what occurs with an EMS organization. Finally, I think we see hesitation of this type of arrangement because various groups feel as if their jobs could be done by someone else or without justification feel there are safety issues. This is similar to why some physician groups don’t feel as if APRNs and PAs should work independently.