Learn how support surfaces work to help prevent pressure injuries.
Takeaways:
- More than pressure should be considered about when selecting a surface.
- Selecting a support surface requires identification of specific patient needs.
- Understanding support surface characteristics facilitates selection.
By Deborah Sidor, MSN, MSNA, NP, ACNS-BC, CCRN, and Mary Sieggreen, MSN, CNS, NP, CVN
Support surfaces are valuable tools for reducing pressure injury (PI) development and progression, but choosing the right one can be challenging. Nurses can make a difference in a patient’s care by learning how support surfaces—such as mattress overlays, mattress replacements, and specialty beds—redistribute or reduce tissue pressure and prevent PIs from developing or worsening. To understand how support surfaces help, you also need to understand how surfaces might contribute to PIs.
Fearsome forces
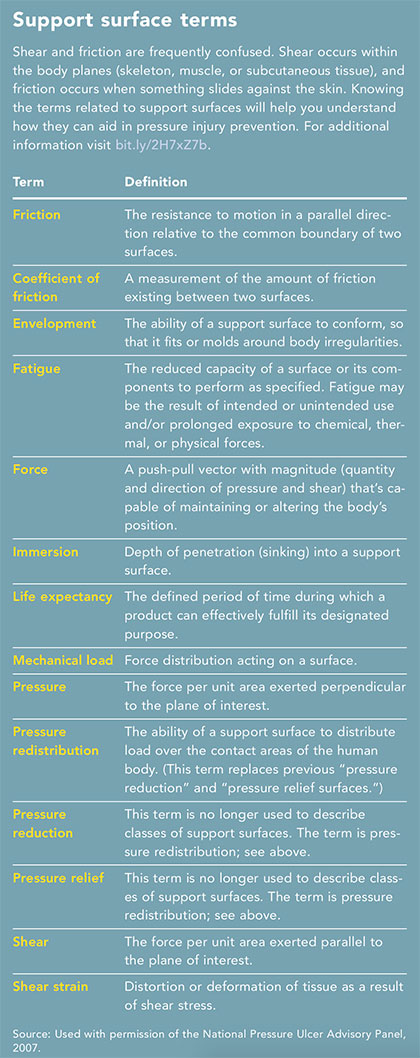 Factors that contribute to PIs include pressure, shear, and microclimate. (See Support surface terms.)
Factors that contribute to PIs include pressure, shear, and microclimate. (See Support surface terms.)
Pressure
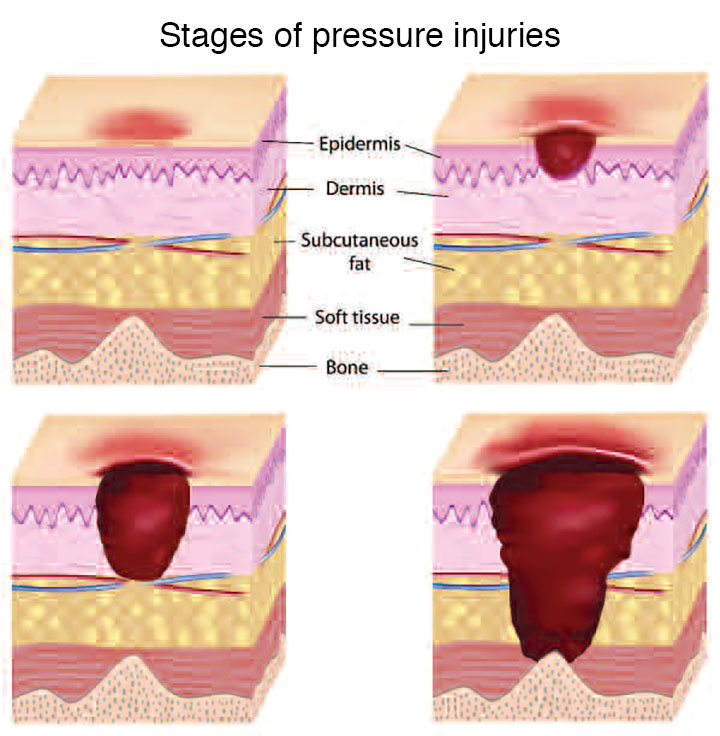
A PI develops when external pressure against the skin exceeds capillary pressure for an extended length of time, resulting in tissue ischemia. It occurs when soft tissue is compressed between a bony prominence and a surface, such as a bed or chair.
Shear
Shear refers to pulling or stretching one part of the body while an adjacent part is pulled or stretched in the opposite direction, damaging both superficial and deep tissues. Shear reduces the tissue’s ability to withstand pressure to less than half of its ability without the shear force. In clinical situations, shear occurs when the head of the bed is elevated more than 30 degrees and the patient slides toward the foot of the bed. The patient’s skin adheres to the bed linen, while the bony skeleton slides downward, resulting in pulling and stretching of blood vessels and underlying tissue distortion.
Microclimate
Microclimate between the patient’s skin and the support surface includes temperature, humidity, and airflow. Normally, the skin releases heat and moisture into the air, allowing the body to cool itself. Because the outward flow of heat and moisture is inhibited when a patient is on a mattress, both increase at the interface between the skin and mattress. As the temperature rises, the metabolic needs of the skin rise. Moisture build-up weakens the skin and makes it more prone to damage.
For support surfaces to successfully contribute to PI prevention, pressure, shear, and microclimate need to be managed.
Support options
The National Pressure Ulcer Advisory Panel (NPUAP) says a support surface is “a specialized device for pressure redistribution designed for management of tissue loads, microclimate, and/or other therapeutic functions.” The most important role of a support surface is redistribution of pressure on the tissue loads.
Components of support surfaces include air, gel, fluid, and foam. Support surface categories include reactive, active, integrated bed systems, nonpowered, powered, overlays, and mattresses. (See Support surface categories.)
Therapeutic support surfaces redistribute tissue loads through immersion (depth of the patient’s body pressing into the support surface) and envelopment (ability of the surface to conform around the body). As the body surface area contacts the support surface, pressure redistribution occurs.
Foam is the most widely used support surface. Foam surfaces are available in a variety of densities, including basic elastic and viscoelastic. High specification foam is preferred for patients at any risk of injury. Density/hardness defines the foam grade; a high specification mattress has a density of 35 kg/m3, a hardness of 130 N (the higher the newton, the more force needed to compress the mattress, which means it’s firmer than one with a lower newton), and a depth of at least 5.9 inches.
But foam isn’t always the best choice, or it may not be the only intervention needed. Select support surfaces based on features that best fit the patient’s needs. For example, studies have shown that beds or surfaces that are air fluidized, have low air loss, or are powered, are effective for patients at high risk for PI or who have existing injuries. The key is to find the right combination. For example, a powered mattress overlay can reduce skin shear while providing a microclimate that removes excessive heat and moisture.
Choose wisely
 In 2014, NPUAP developed these general recommendations for support surface selection and monitoring:
In 2014, NPUAP developed these general recommendations for support surface selection and monitoring:
- Select a support surface that meets individual patient needs.
- Choose a support surface compatible with the care setting.
- Examine the appropriateness and functionality of the surface on each encounter with the patient.
- Identify and prevent complications of support surface use.
- Verify the support surface is used within its functional lifespan.
- Reposition the patient regularly.
- Choose devices, incontinence pads, linen, and clothing compatible with the support surface.
Despite these recommendations, selecting a support surface can be challenging because of confusing terminology and standards. Fortunately, you have two excellent resources.
- NPUAP created the Support Surface Standards Initiative (S3I) to help develop uniform support surface terminology, test methods, and reporting standards.
- The Wound Ostomy Continence Society created an evidence- and consensus-based algorithm for support surface selection. Instructions for the algorithm are provided in a free education module.
Monitoring and more
Your work isn’t done after support surfaces are selected and placed. You must monitor the system to ensure it’s working properly and assess patients vigilantly. A change in patient condition may require a change in support surface. Document patient assessments and support surfaces used in the patient’s health record and communicate them during patient hand-offs.
A tailored approach
Tailor prevention and treatment interventions to individual patient needs and desires. When selecting an appropriate support surface, consider the patient’s PI risk assessment results, level of immobility, need for microclimate control and shear reduction, and his or her size and weight. Also consider the number, severity, and location of existing PIs; the patient’s comfort and preference; and surface availability and ease of use. No one surface is ideal for all patients, so use your analytical skills to ensure the optimal fit between the patient and the support surface. •
Deborah Sidor is a nurse practitioner at St. John Providence Health System in Novi, Michigan. Mary Sieggreen is a nurse practitioner for vascular surgery and a clinical nurse specialist for wound care at Harper University Hospital in Detroit, Michigan.
Selected references
Call E, Tescher A. S3I Update: New support surface testing standards. Implications for clinical practice. NPUAP Annual Conference: Where Research meets Practice presentation. Las Vegas, March 3, 2018.
Clark M, Black J. Skin IQ microclimate manager made easy. Wounds International. 2011;2(2):1-6.
Doughty DB, McNichol LL. Wound, Ostomy and Continence Nurses Society Core Curriculum: Wound Management. Wolters Kluwer; Philadelphia; 2015.
Jordan RS, Phipps S. Understanding therapeutic support surfaces. Wound Care Advisor. 2014. woundcareadvisor.com/understanding-therapeutic-support-surfaces-vol3no3/
Maklebust J. Take the load off by choosing the right support surface. Nursing. 2004;Suppl:12-5.
McInnes E, Jammali-Blasi A, Bell-Syer SE, Dumville JC, Middleton V, Cullum N. Support surfaces for pressure ulcer prevention. Cochrane Database Syst Rev. 2015;3(9):CD001735.
McNichol L, Watts C, Mackey D, Beitz JM, Gray M. Identifying the right surface for the right patient at the right time: Generation and content validation of an algorithm for support surface selection. J Wound Ostomy Continence Nurs. 2015;42(1):19-37.
McNichol L, Watts, Mackey D, Beitz J, Gray M, Carchidi C. Choosing a support surface to prevent pressure ulcers: An evidence-based algorithm aids selection. Am Nurse Today. 2015;10(11):13-4.
National Pressure Ulcer Advisory Panel. Terms and definitions related to support surfaces. 2007.
National Pressure Ulcer Advisory Panel, European Pressure Ulcer Advisory Panel and Pan Pacific Pressure Injury Alliance; Haesler E (ed). Prevention and Treatment of Pressure Ulcers: Clinical Practice Guideline. 2014; Osborne Park, Western Australia; Cambridge Media.
Serraes B, Beeckman D. Static air support surfaces to prevent pressure injuries: A multicenter cohort study in Belgian nursing homes. J Wound Ostomy Continence Nurs. 2016;43(4):375-8.
Serraes B, van Leen M, Schols J, Van Hecke A, Verhaeghe S, Beeckman D. Prevention of pressure ulcers with a static air support surface: A systematic review. Int Wound J. 2018 [Epub ahead of print.]
Stone A, Brienza D, Call E, et al. Standardizing support surface testing and reporting: A National Pressure Ulcer Advisory Panel executive summary. J Wound Ostomy Continence Nurs. 2015;42(5):445-9.
ANT0518_Dabir_NavigatingMazeSupportSurfaces