Nurses’ understanding of this condition will aid symptom management and patient care.
- Long Covid presents as a constellation of symptoms persisting for more than 4 weeks after the acute phase of the COVID-19 infection.
- Diagnosing Long COVID is complex given the symptom diversity and the overlap with several other conditions.
- Effective treatment modalities for Long COVID continue to evolve. Many ongoing research studies aim at better understanding the condition and develop effective treatments.
- Nurses play a crucial role in providing comprehensive care, advocating for patients, and contributing to public health initiatives to mitigate the long-term impact of COVID-19.
Learning Objectives
- Explain the terminology related to defining Long COVID pathophysiology.
- Describe common symptoms and clinical manifestations of Long COVID.
- Define treatment approaches for patients with Long COVID.
No relevant financial relationships were identified for any individuals with the ability to control content of the activity.
Expiration: 1/1/28
The federal COVID-19 public health emergency (PHE), declared under the Public Health Service Act, officially ended at midnight on May 11, 2023, but the virus persists. Although we see encouraging signs that the pandemic is in the rearview mirror, for some who had COVID-19, the negative health consequences continue to ride shotgun.
Keys to understanding long COVID
Long COVID, a stigmatized and somewhat controversial condition, has begun to gain the public’s attention as some who previously had acute COVID-19 began reporting a unique constellation of symptoms. To best care for patients with Long COVID and provide them with the support and resources they need to manage symptoms, nurses must understand what it is and stay aware of the evolving research.
Long COVID defined
The term “Long COVID” emerged early as lay people described a set of signs and symptoms that continue or progress after the acute phase of the SARS-CoV-2 infection. The National Academies of Sciences, Engineering, and Medicine (National Academies) defines Long Covid as an infection-associated chronic condition that emerges after a SARS-CoV-2 infection and persists for at least 3 months. It can manifest as a continuous, relapsing and remitting, or progressive state that impacts one or more organ systems. Manifestations encompass a wide range and combination of signs, symptoms, and diagnosable conditions.
The National Academies released their broadly inclusive definition of Long COVID on June 11, 2024, aiming to improve documentation and treatment. This new definition and forthcoming framework strive to standardize terminology in future literature, leading to more consistent use of “Long COVID” rather than the previously common term “Post-acute sequelae of SARS-CoV-2 infection” (PASC). Many of the articles discussed in this review use PASC, the predominant term in earlier literature. Although PASC and Long COVID refer to the same general phenomenon of long-term effects after a COVID-19 infection, they may differ in terms of specific definitions, criteria, and use in different contexts (research vs. public policy).
The National Academies’ definition emphasizes the chronicity and variability of Long COVID. It provides a structure and inclusive framework for understanding and diagnosing the condition, which will help minimize terminology variations across research and health sectors. (See Long COVID and its impact.)
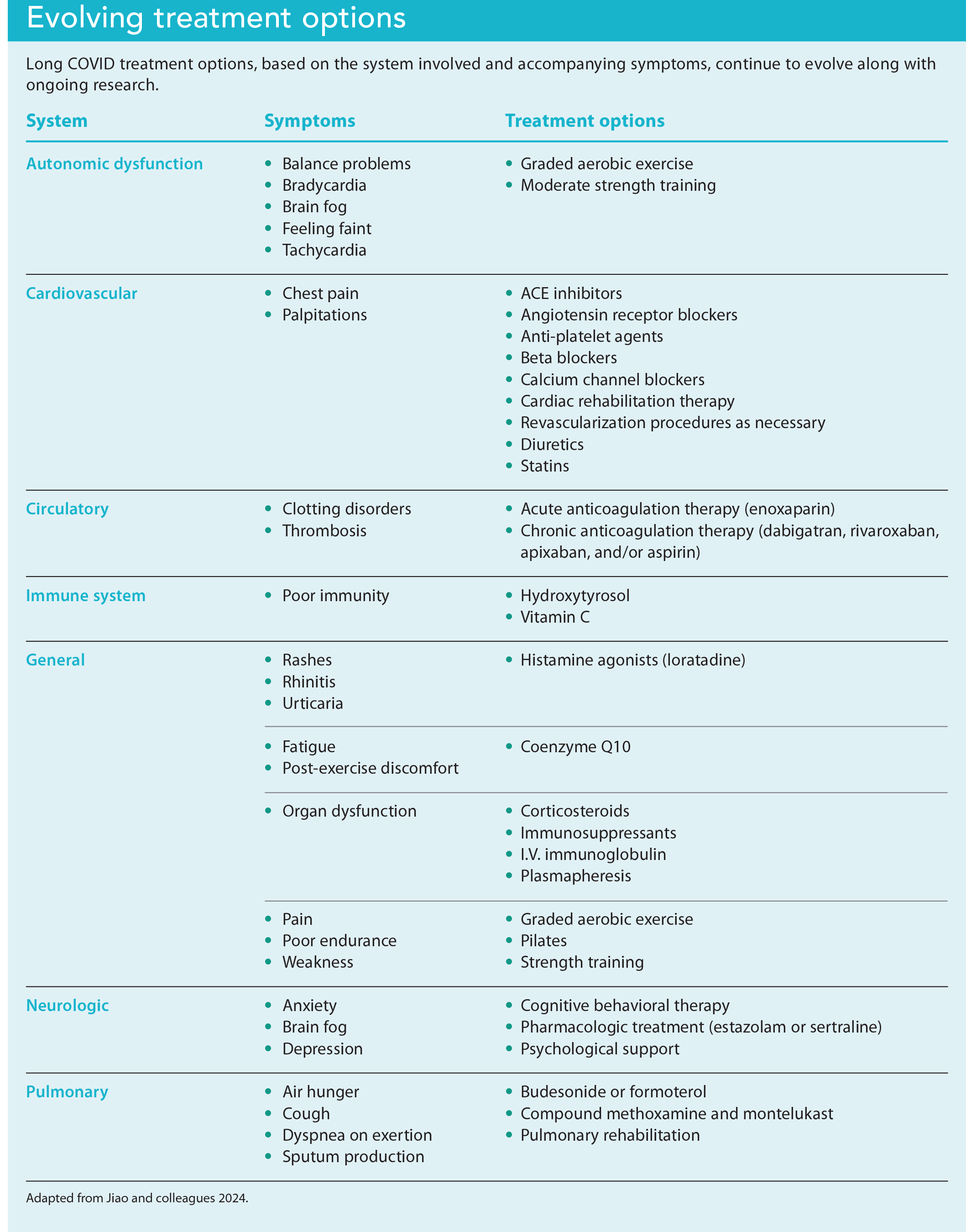
Long COVID and its impact
Understanding the key characteristics of Long COVID and their impact on patients can help nurses provide appropriate care.
Adapted from U.S. Department of Health and Human Services. Terms & definitions. October 28, 2024. covid.gov/be-informed/longcovid/about#term
Despite the National Academies’ recent efforts to standardize terminology, researchers have used Long COVID, PASC, Long-haul COVID, Chronic COVID syndrome, Post-COVID-19 condition, and Post-acute COVID-19 syndrome interchangeably since the pandemic began. Although PASC remains commonly used in medical research, to support efforts to standardize terminology, I’ll use Long COVID here unless the original author used PASC.
Epidemiology
Long COVID prevalence remains uncertain due to the differences in terminology and how it’s defined and studied. In addition, the methods for calculating rates differ dramatically across available studies.
The most extensive study, by the Global Burden of Disease Long COVID Collaborators, included a meta-analysis of 54 studies and two medical record databases across 22 countries from March 2020 to January 2022. The authors found that at 3 months post-infection, 6.2% of individuals who had symptomatic COVID-19 infection experienced at least one of a set of three Long COVID symptom clusters. The clusters consisted of persistent fatigue with body pain or mood swings (3.2%), cognitive issues (2.2%), or ongoing respiratory problems (3.7%).
Sedgley and colleagues analyzed the electronic health records (EHRs) of nearly 1 million ambulatory patients with COVID-19. They found that 15% had at least one Long COVID symptom 12 to 20 weeks after the infection, compared to only 2.9% of patients without COVID-19.
In another study of patients from around the world, Chen and colleagues suggest a global estimated pooled prevalence of around 0.43% of individuals who’ve had COVID-19 experiencing long-lasting symptoms or complications after recovering from the acute phase. Commonly experienced symptoms included joint stiffness (4.5%), cough (3.0%), and fatigue (2.7%). Among individuals diagnosed with COVID-19, those with pre-existing medical conditions had the highest likelihood of experiencing long-lasting symptoms.
Perlis and colleagues conducted a cross-sectional study of over 16,000 survey respondents who tested positive for COVID-19 within the prior 2 months. In this study, 14.7% of respondents reported continued COVID-19 symptoms more than 2 months after acute infection. Notably, patients who completed the primary vaccine series before infection had a decreased risk for Long COVID.
Risk factors for developing Long COVID aren’t well defined. Individuals with higher body mass index, older adults, and those with multiple comorbidities are considered at highest risk of developing symptoms. Female gender also appears to be a risk factor. Individuals with a history of significant pre-existing conditions, such as hypertension, obstructive pulmonary disease, obesity, allergies, a cognitive disorder, transient ischemic attack, depression, and anxiety, also fall into the high-risk category. Having a severe case of acute COVID-19 illness also predisposes patients to Long COVID.
Clinical manifestations
Most Long COVID studies examine the frequency of individual symptoms. However, due to their retrospective nature and absence of a comparison group of uninfected patients, these studies have produced varying prevalence estimates. They also have widely divergent inclusion and exclusion criteria: some include hospitalized patients; others, non-hospitalized patients; some use EHR data; and others take a survey approach. Precisely pinpointing the symptoms unique to Long COVID can prove perplexing. The diverse and overlapping symptoms of PASC create challenges to accurately link the constellation of presenting symptoms to the condition. According to a study by Davis and colleagues, PASC has over 200 associated symptoms.
Thaweethai and colleagues completed a complex prospective cohort study to develop a definition of PASC. In this study, involving 9,764 participants from the Researching COVID to Enhance Recovery (RECOVER) adult cohort, researchers identified 37 symptoms that commonly occur in those known to have COVID-19 and persist for 6 months or more after infection compared to uninfected participants. They developed a preliminary method for diagnosing PASC based on a combination of these symptoms.
Symptoms contributing to the PASC diagnosis included post-exertional malaise, fatigue, cognitive impairment, dizziness, GI issues, heart palpitations, changes in sexual function, loss of smell or taste, thirst, chronic cough, chest pain, and abnormal movements. Among 2,231 participants infected with COVID-19 after December 1, 2021, and enrolled within 30 days of infection, 10% were identified as PASC-positive at 6 months. Across all sources examined, the list provided in this study appeared to correlate with the bulk of the literature.
A significant challenge in quantifying Long COVID is the overlap of its associated symptoms with those of other diseases. This overlap is evident in studies that included a control group consisting of individuals not suspected of having had COVID-19. For example, according to the Office for National Statistics in the United Kingdom, although 5.0% of individuals reported Long COVID symptoms 12 to 16 weeks after infection, 3.4% of a control group who had not tested positive for COVID-19 reported similar symptoms.
Due to the complexities surrounding presentation and symptomatology, an accurate list of what we can and can’t call Long COVID remains elusive. A universal list could simplify Long COVID diagnosis, but the diverse range of human health profiles makes that task challenging, which highlights the need for a holistic, interprofessional approach to diagnosis. (See Common symptoms.)
Common symptoms
According to the Centers for Disease Control and Prevention, the most common symptoms of Long COVID include the following:
Digestive
- Diarrhea
- Stomach pain
General
- Chest pain
- Cough
- Difficulty breathing or shortness of breath
- Fever
- Rapid heart rate, pounding heart, or palpitations
- Symptoms that worsen after physical or mental exertion
- Tiredness and fatigue (interferes with daily life)
Neurologic
- Change in taste or smell
- Depression or anxiety
- Difficulty concentrating (brain fog)
- Dizziness when standing up
- Headache
- Pins-and-needles feelings
- Sleep problems
Other
- Changes in menstrual cycle
- Joint or muscle pain
- Rash
Adapted from the Centers for Disease Control and Prevention. Signs and symptoms of Long COVID. July 11, 2024. www.cdc.gov/covid/long-term-effects/long-covid-signs-symptoms.html
Diagnosis
Srikanth and colleagues completed a scoping review of the literature in search of papers focused on Long COVID diagnosis. After identifying 225 records, the authors used detailed inclusion and exclusion criteria in conjunction with the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews to narrow them down to 11 original papers focused on the process of Long COVID diagnosis. Their work resulted in a systematic approach to diagnosing a patient with Long COVID who’s recovered from the acute phase of COVID-19 and currently tests negative for the virus.
If symptoms such as fatigue, chest pain, dyspnea, post-exertion signs, or altered function persist 4 weeks after recovery from COVID-19 or patients experience symptoms for more than 6 weeks, they should follow-up with their healthcare provider for the evaluation of symptom persistence and severity, as well as to assess for pre-existing conditions. Initially, providers should treat the patient’s symptoms, with consideration given to other potential diseases. If the symptoms persist without resolution, providers should suspect Long COVID.
Confirming Long COVID involves ruling out other post-viral conditions and disorders. Depending on the geographic region where the patient lives, the provider should order tests to exclude conditions such as post-infectious mononucleosis, vitamin deficiency, thyroid disorders, anemia, and post-West Nile virus.
Given the subjective nature of this diagnostic process, underestimation of Long COVID may exist among certain populations. Black and Hispanic communities in the United States were affected more than others in the acute phase of the pandemic, but their reported Long COVID rates are comparable to those of the White population. Although this finding isn’t understood, it does create cause for concern; individuals from certain demographics and those experiencing complicated social determinants of health frequently encounter more barriers to accessing healthcare services, which may result in underreporting of Long COVID within these populations.
The article by Srikanth and colleagues also speaks to a “wariness” that clinicians may feel about assigning a diagnosis of Long COVID. This wariness may arise from a lack of treatment options and concerns that patients might take advantage of an uncertain diagnosis to obtain social benefits, such as unemployment, work accommodations, or disability. These concerns serve as motivation to standardize Long COVID criteria and highlight the importance of approaching each case with empathy while conducting a thorough history and physical. Most patients genuinely seek relief from their symptoms rather than external rewards.
In addition, efforts continue to find biomarkers, such as specific proteins, detectable by blood tests and other diagnostic methods. This sort of sophisticated testing might help clinicians feel more confident in their diagnostic accuracy and their ability to provide patients with an explanation for their ongoing symptoms.
Causes
Fully comprehending the pathophysiology that contributes to Long COVID may take decades; despite the number of scientists participating in extensive research, the exact underlying mechanism of long COVID remains unknown and effective treatments remain elusive. Discussing the overwhelming amount of literature related to the causal mechanisms of Long COVID is beyond the scope of this article. However, Krishna and colleagues note that several potential mechanisms have been proposed, including enduring end-organ damage resulting from acute infection, lingering viral presence, autoimmune reactions, immune system dysfunction, vascular issues or blood clotting disorders, and the reactivation of dormant viruses.
In 2023, Wong and colleagues presented a “unified pathway,” which integrates previously hypothesized causal routes (autonomic dysfunction, hypercoagulability, chronic inflammation, viral persistence) and offers potential avenues for therapeutic intervention. Their research suggests that a link may exist between Long COVID and a reduction in serotonin levels.
They hypothesize that inflammation from the virus contributes to serotonin deficits as a result of decreased absorption of tryptophan (the precursor of serotonin) in the intestines, heightened platelet activation and subsequent depletion of serotonin stores, and increased serotonin turnover mediated by monoamine oxidase. Their hypothesis suggests that this complex series of events impairs vagus nerve function, which leads to compromised hippocampal function and memory impairment. These findings may shed light on the brain fog symptoms observed in Long COVID and potentially extend to other post-viral syndromes.
Treatment
Long COVID treatment, which continues to evolve, varies based on each patient’s symptoms and requires an individualized approach. Each set of symptom clusters or psychosocial challenges necessitates a different subgroup of interventions, specialists, and interprofessional care coordination.
Social services sits at the center of Long COVID management. From financial stress and employment uncertainty to relationship and quality of life disruptions, the cascading effects of Long COVID can prove extensive. Social workers play a crucial role in addressing these issues, linking patients to resources and serving as advocates.
Not all patients require a referral to specialists, but some may need one or more to address ongoing symptoms and reduce morbidity and mortality. Primary care providers have the best understanding of the patient from a holistic perspective. They’re well positioned to treat patients and also act as care managers to coordinate specialists and ensure physical and psychosocial needs are met.
Throughout the literature, researchers highlight fatigue as one of the most common features of Long COVID. For these patients, treatment should focus on improving their functional status and capacity for physical activity. Light aerobic exercise, such as walking and Pilates, is recommended. Gradually increasing the intensity of the exercise over 4 to 6 weeks, in conjunction with a gradual return to work, can prove effective.
Long COVID can impact many body systems, leading to pulmonary, cardiovascular, central nervous system, sensory, and mental health symptoms. (See Evolving treatment options)
Pulmonary
The most commonly reported Long COVID symptoms include pulmonary complications; many patients have persistent difficulty breathing with or without radiologic abnormalities. These symptoms may persist for months after recovery from COVID-19. Although not all patients with difficulty breathing have radiologic findings, those who do may have “ground-glass” opacities or fibrotic lesions. Studies indicate that these signs improve over time.
Pulmonary function testing can help reveal decreased lung capacity and decreased forced vital capacity, which tend to improve with time. Definitive treatment of these anomalies continues to evolve, but some treatments—including pulmonary rehabilitation therapy, antifibrotic agents, corticosteroids, and inhaled therapeutic agents—show promise. In severe cases, such as when patients can’t be weaned from ventilator support or for those who experience persistent and severe oxygen dependence, lung transplantation, although controversial, may be warranted.
Cardiovascular
Many patients with Long COVID experience cardiovascular complications; the most common is myocarditis. In its acute phase, myocarditis can lead to significant decompensation, dysrhythmias, cardiogenic shock, and death. Beyond the acute phase, patients are at risk for developing chronic heart failure related to cardiomyopathy and injury to myocardial cells.
Patients with activity intolerance, palpitations, edema, chest pain, shortness of breath, or other associated symptoms should undergo a thorough evaluation by a board-certified cardiologist. Traditional therapies—such as cardiac rehabilitation, beta-blockers, ACE-inhibitors, anti-arrhythmic drugs, and diuretics—have proven effective in improving cardiac complications.
Central nervous system
COVID-19 infection can result in acute and long-term central nervous system and neurocognitive complications. Common symptoms include headache, insomnia, and psychosis. Many patients with Long COVID report persistent headache, which also may be associated with dizziness, mental fog, and fatigue. Headaches associated with Long COVID have been observed to exhibit only a limited reaction to first line pain-relieving medications; other treatment options are still being evaluated. Referral to a neurologist offers options for further evaluation and advanced treatment.
The National Institutes of Health (NIH) initiated clinical trials through the RECOVER initiative, which included study of a web-based brain training program as possible treatment for impaired cognitive function. The NIH continues to evaluate the use of a web-based goal management training program to improve executive function as well as a home-based transcranial direct current stimulation device to increase brain activity and blood flow. The RECOVER initiative has several other ongoing clinical trials aimed at addressing Long COVID-related disorders and symptoms.
Sensory
A pair of commonly overlooked symptoms of acute COVID-19 and Long COVID are anosmia (loss of smell) and ageusia (loss of taste). Although not all who had acute COVID-19 or Long COVID symptoms experience anosmia or ageusia, those who do may face disruptions in their quality of life including loss of appetite, weight loss, alterations in eating habits, and changes in food preferences.
These troubling symptoms, which may last from months to years, highlight the important role that dieticians can play. Most of the sensory experience related to eating centers around the flavor of foods; anosmia and ageusia alter this relationship with food. However, various interventions can help.
For example, changing food textures and colors can stimulate the trigeminal nerve and brain activity respectively. Adding more color to one’s diet and combining different food textures with strong flavors may increase the pleasure of eating. Research also indicates that olfactory training with intense aromas, such as lemon, rose, clove, and eucalyptus, may facilitate a return of the sense of smell.
Psychological
Anxiety and depression rank as the second and third most frequently reported Long COVID symptoms. Limited evidence or guidance exists on how best to treat challenging mental health conditions in patients with Long COVID; the science continues to evolve. However, patients should be screened for psychiatric disorders such as anxiety, depression, and PTSD using reliable and valid tools. They also should be assessed for risk of self-harm. Patients determined to be at risk for self-harm require inpatient referral and a suicide prevention plan.
Traditional treatment approaches—such as cognitive behavioral therapy, selective serotonin reuptake inhibitors, mood stabilizers, and anti-anxiety medications—have proven beneficial for patients with mental health disorders associated with Long COVID. The degree of severity should guide the care of individuals coping with mental health challenges. Referrals to mental health specialists such as psychiatrists, mental health counselors, psychologists, and others should be considered for patients with moderate-to-severe symptoms. (To learn more about evolving treatment options, visit myamericannurse.com/?p=411491.)
Nursing implications
Understanding Long COVID enhances nurses’ ability to deliver compassionate, comprehensive, and high-quality patient care. Nurses at the frontline can recognize and assess Long COVID severity to ensure timely and appropriate management. This understanding enables effective patient education about Long COVID, its potential long-term effects, and the importance of ongoing treatment.
Patient education
Nurses can provide specific interventions, such as developing symptom management plans, coordinating interprofessional care, and offering mental health support. For example, nurses can help patients manage fatigue by teaching them about energy conservation techniques and how to pace activities. In addition, nurses can offer guidance related to breathing exercises to build respiratory capacity and aid anxiety management. They also can recommend mindfulness, guided imagery, and relaxation techniques to manage pain.
Emotional support
The emotional support nurses provide patients includes listening to their concerns, validating their experiences, and providing reassurance. For example, nurses can establish support groups in which patients have an opportunity to share their experiences and learn coping strategies.
Collaborative care
Nurses can work with physicians, physical therapists, mental health professionals, and other members of the care team to develop holistic, comprehensive care plans tailored to each patient’s needs. Nurses also can participate in public health initiatives, such as community education programs about Long COVID and vaccination drives to prevent COVID-19.
Advocacy
Nurses, empowered with Long COVID knowledge, have the opportunity to advocate for patients, influence healthcare policies, and ensure resource allocation for Long COVID care. For example, nurses should consider advocating for extended follow-up care for patients with COVID-19, working to elect patient-focused legislators and thought leaders, and supporting policies that fund Long COVID research and treatment programs.
Self-care
Finally, nurses must emulate self-care and strengthen their own well-being through healthy eating, regular exercise, mindfulness practices, and adequate rest. They also should seek support from peers, mentors, and behavioral health professionals. By prioritizing their own health, nurses serve as examples for those they engage with. Self-care allows nurses to remain resilient and possess the compassion necessary to provide high-quality care.
A monumental effort
The emergence of Long COVID presents significant challenges for patients and healthcare professionals alike. This unique constellation of waxing and waning symptoms after an acute COVID-19 infection affects a significant number of individuals worldwide. Although the science continues to evolve, we’re beginning to get a better sense of relevant diagnostic and treatment approaches. The monumental effort underway by scientists and healthcare workers to continue research efforts will benefit society, instill hope, and help us all heal from the tragedies of this global pandemic.
Erik P. Southard is a professor and DNP program director at Indiana State University School of Nursing in Terre Haute.
American Nurse Journal. 2025; 20(1). Doi: 10.51256/ANJ012506
References
Centers for Disease Control and Prevention. Long COVID basics. July 11, 2024. cdc.gov/covid/long-term-effects/?CDC_AAref_Val=https://www.cdc.gov/coronavirus/2019-ncov/long-term-effects/index.html
Centers for Medicare & Medicaid Services. Moving forward after COVID-19 public health emergency. September 19, 2024. cms.gov/priorities/health-equity/minority-health/resource-center/moving-forward-after-COVID-19-public-health-emergency
Chen C, Haupert SR, Zimmermann L, Shi X, Fritsche LG, Mukherjee B. Global prevalence of post–Coronavirus disease 2019 (COVID-19) condition or Long COVID: A meta-analysis and systematic review. J Infect Dis. 2022;226(9):1593-1607. doi:10.1093/infdis/jiac136
Cheng AL, Anderson J, Didehbani N, et al. Multi-disciplinary collaborative consensus guidance statement on the assessment and treatment of mental health symptoms in patients with post-acute sequelae of SARS-CoV-2 infection (PASC). PM R. 2023;15(12):1588-1604. doi:10.1002/pmrj.13085
Davis HE, McCorkell L, Vogel JM, Topol EJ. Long COVID: Major findings, mechanisms and recommendations. Nat Rev Microbiol. 2023;21(3):133-46. doi:10.1038/s41579-022-00846-2
Frontera JA, Simon NM. Bridging knowledge gaps in the diagnosis and management of neuropsychiatric sequelae of COVID-19. JAMA Psychiatry. 2022;79(8):811-7. doi:10.1001/jamapsychiatry.2022.1616
Global Burden of Disease Long COVID Collaborators. Estimated global proportions of individuals with persistent fatigue, cognitive, and respiratory symptom clusters following symptomatic COVID-19 in 2020 and 2021. JAMA. 2022;328(16):1604–15. doi:10.1001/jama.2022.18931
Greenhalgh T, Knight M, A’Court C, Buxton M, Husain L. Management of post-acute COVID-19 in primary care. BMJ. 2020;370:m3026. doi:10.1136/bmj.m3026
Jiao T, Huang Y, Sun H, Yang L. Research progress of post-acute sequelae after SARS-CoV-2 infection. Cell Death Dis. 2024;15(4):257. doi:10.1038/s41419-024-06642-5
Krishna B, Wills M, Sithole N. Long COVID: What is known and what gaps need to be addressed. Br Med Bull. 2023;147(1):6-19. doi:10.1093/bmb/ldad016
Naidu AS, Clemens RA. No smell, no taste—Dealing with a “senseless” phase of the pandemic: Nutritional management of COVID-19 and postacute sequelae of COVID-19. Nutr Today. 2022;57(6):309-16. doi:10.1097/NT.0000000000000574
National Academies of Sciences, Engineering, and Medicine. A Long COVID definition: A chronic, systemic disease state with profound consequences. Washington, DC: The National Academies Press; 2024. doi:10.17226/27768
National Institutes of Health. NIH launches Long COVID clinical trials through RECOVER Initiative, opening enrollment. July 31, 2023. www.nih.gov/news-events/news-releases/nih-launches-long-covid-clinical-trials-through-recover-initiative-opening-enrollment
Office for National Statistics. Technical article: Updated estimates of the prevalence of post-acute symptoms among people with coronavirus (COVID-19) in the UK: 26 April 2020 to 1 August 2021. September 16, 2021. bit.ly/48wxTjJ
Parker AM, Brigham E, Connolly B, et al. Addressing the post-acute sequelae of SARS-CoV-2 infection: A multidisciplinary model of care. Lancet Respir Med. 2021;9(11):1328-41. doi:10.1016/S2213-2600(21)00385-4
Perlis RH, Santillana M, Ognyanova K, et al. Prevalence and correlates of Long COVID symptoms among US adults. JAMA Netw Open. 2022;5(10): e2238804. doi:10.1001/jamanetworkopen.2022.38804
Sedgley R, Winer-Jones J, Bonafede M. Long COVID incidence in a large US ambulatory electronic health record system. Am J Epidemiol. 2023;192(8):1350-7. doi:10.1093/aje/kwad095
Srikanth S, Boulos JR, Dover T, Boccuto L, Dean D. Identification and diagnosis of long COVID-19: A scoping review. Prog Biophys Mol Biol. 2023;182:1-7. doi:10.1016/j.pbiomolbio.2023.04.008
Thaweethai T, Jolley SE, Karlson EW, et al. Development of a definition of postacute sequelae of SARS-CoV-2 infection. JAMA. 2023;329(22):1934-46. doi:10.1001/jama.2023.8823
Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann Intern Med. 2018;169(7):467-73. doi:10.7326/M18-0850
Wang L, Foer D, MacPhaul E, Lo YC, Bates DW, Zhou L. PASCLex: A comprehensive post-acute sequelae of COVID-19 (PASC) symptom lexicon derived from electronic health record clinical notes. J Biomed Inform. 2022;125:103951. doi:10.1016/j.jbi.2021.103951
Williams S. Emerging research on postacute COVID-19 complications. JAAPA. 2023;36(7):11-5. doi:10.1097/01.JAA.0000937252.09508.f0
Wong AC, Devason AS, Umana IC, et al. Serotonin reduction in post-acute sequelae of viral infection. Cell. 2023;186(22):4851-67. doi:10.1016/j.cell.2023.09.013
Key words: COVID-19, post-acute sequelae of SARS-CoV-2 infection, PASC, pandemic, Long COVID

















2 Comments. Leave new
thanks for info.
Excellent article. I will also use it to educate my family and friends.