
Focused assessment can aid quick diagnosis and treatment.
Takeaways:
- Rapid nurse identification of myocardial infarction in medical surgical patients is key to achieving lifesaving treatment in the heart catheterization lab.
- Focused chest pain assessment, 12-lead ECG performance, emergent administration of loading medications such as aspirin, and an anti-platelet agent are imperative to the survival of heart muscle and patient lives.
Henry Low*, age 75, is admitted to a monitored unit with indigestion-related chest pain. After dinner he experiences chest pain and pushes his call button. The evening nurse, Sam Cordone, finds Mr. Low sitting up in bed and holding his hand to the center of his chest. Sam notes that Mr. Low is diaphoretic and short of breath, his respiratory rate (RR) has increased from 12 (when he was admitted) to 22 breaths per minute, and his O2 saturation is 95% on room air. Sam’s focused cardiac assessment indicates that Mr. Low’s blood pressure (BP) is 135/75 mmHG and his heart rate (HR) is 88 beats per minute (bpm). Mr. Low’s lungs are clear at the apex and diminished in the bases.
Sam asks Mr. Low if this is how he felt in the emergency department (ED) and then asks him to rate his pain on a 1 to 10 scale. Mr. Low rates his pain as 6 and tells Sam that he had a similar episode the previous week, but that he didn’t go to the ED. Sam reviews Mr. Low’s chart and finds that he’s been a smoker for 55 years and has a history of heart failure. Seeing nothing alarming, Sam leaves Mr. Low’s room to retrieve an antacid to treat indigestion.
Caring for patients with a left ventricular assist device
Attacking anterior-wall myocardial infarction in time
Identifying complete heart block in elderly patients
While Sam is waiting to retrieve the medication, Mr. Low pushes his call button again. When Sam returns, Mr. Low is bent over in bed clutching his chest. His HR is 104 bpm, RR 10 breaths per minute, pulse oximetry 90%, and BP 80/52 mmHG. Sam places Mr. Low on 2 L of oxygen by nasal cannula and calls the rapid response team (RRT). He then pushes the button on the telemetry pack to check Mr. Low’s heart rhythm and finds that he has sinus tachycardia with ST elevation.
When the RRT arrives, they perform a 12-lead ECG and draw blood for chemistry, troponin, and a complete blood count. The ECG confirms sinus tachycardia with an ST elevation of 2 mm in leads II, III, and aVF with reciprocal changes in leads I and aVL and ST elevation of 2 mm in V3-5. In addition, the J point is 4 mm above baseline. The RRT nurse notes lead II ST elevation in the 12-lead ECG from the ED. (See 12-lead ECG.)
12-lead ECG
The areas circled on the ECG tape show ST segment elevation, which is interpreted as acute inferior and right ventricular myocardial infarction with premature ventricular contractions.
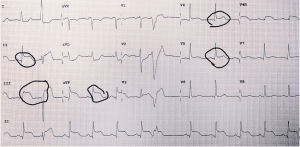
12 Lead courtesy of Wikimedia commons https://commons.wikimedia.org/wiki/File:Inferior_and_RtV_MI_with_PVC_15_lead.jpg
The RRT immediately notifies the heart catheterization laboratory, cardiologist on call, and attending provider, anticipating that Mr. Low will receive percutaneous coronary intervention (PCI) in the heart catheterization lab. Per protocol, the RRT nurse administers aspirin and clopidogrel before taking Mr. Low to the lab.
Myocardial infarction
Acute coronary syndrome (ACS) encompasses five types of myocardial infarction (MI) and injury. (See MI types.)
MI types
The five types of myocardial infarction (MI) are:
Type 1: Spontaneous MI related to ischemia caused by a primary coronary event (for example, plaque erosion or rupture, fissuring, or dissection)
Type 2: MI secondary to ischemia caused by either oxygen demand or decreased supply
Type 3: Sudden unexpected cardiac death with symptoms that suggest myocardial ischemia
Type 4: MI associated with percutaneous coronary intervention (Type 4a) or stent thrombosis (Type 4b)
Type 5: MI associated with cardiac surgery
Source: Thygesen et al. 2012
For the purposes of this review, we’ll focus on Type 1 MI (ST-segment elevation MI [STEMI]), which is caused by atherosclerotic plaque rupture, ulceration, fissure, or erosion leading to intraluminal thrombus formation and obstructed coronary blood flow. ST elevation on a 12-lead ECG and positive troponin blood chemistry indicate a medical emergency.
Although EDs are the first to receive patients with MI, some may occur after admission. Patients admitted to the acute care setting are most at risk of death. Every nurse should have a working knowledge of key MI assessments.
Pathophysiology and prevalence
According to the Centers for Disease Control and Prevention, coronary heart disease is the leading cause of death in the United States. After menopause, the rate of heart disease in women increases and rivals that of men. (See MI risk factors.)
MI risk factors
Some myocardial infarction (MI) risk factors can’t be changed, whereas others can.
| Major risk factors that can’t be changed | Major risk factors that can be modified, treated, or controlled | Other factors that contribute to heart disease risk and that can be modified, treated, or controlled |
| Increasing age | Smoking | Stress |
| Gender | High blood pressure | Alcohol |
| Heredity (including race) | High blood cholesterol | Diet and nutrition |
| Physical inactivity | ||
| Obesity and overweight | ||
| Diabetes |
Atherosclerosis frequently occurs in bifurcated arteries or areas of blood-flow turbulence. As plaque increases, the artery’s lumen narrows, and eventually results in ischemia, which prevents oxygenated blood from reaching the heart muscle, causing chest pain. Atherosclerotic plaque can rupture through the lumen of the artery. Exposed collagen and plaque activate platelets and the coagulation cascade, resulting in thrombus formation. Thrombi block blood flow and cause ACS.
Mr. Low: Mr. Low has three risk factors: age 75, obesity, and smoking.
Nurse assessment: Clinical signs and symptoms
The key MI signs and symptoms include:
- chest pain (with or without radiation to jaw, neck, arm)
- shortness of breath
- dizziness
- diaphoresis
- atypical symptoms such as nausea, weakness, change in mentation, heartburn, or frequent belching
- ST changes of 1 mm or more
- tachyarrhythmias
- Levine’s sign (clutching chest).
Patients may not have all of these signs. In addition, gastroesophageal reflux, severe anxiety, aortic dissection, and other diseases may mimic cardiac-related chest pain. (See Nursing chest pain assessment.)
Nursing chest pain assessment
The nursing chest pain assessment should focus on capturing features of the patient’s pain using the PQRST mnemonic.
Provoke: What provokes the pain?
Quality: Is the pain dull, sharp, or stabbing?
Radiation: Does the pain move to the jaw, neck, or arms?
Severity: How severe is the pain (use a pain scale)?
Time and Triggering factors: When and for how long is the pain felt?
Mr. Low: Sam’s assessment and clear communication of Mr. Low’s symptoms help the RRT deliver quick care and advocate for Mr. Low’s need for cardiac catheterization and PCI for a STEMI.
Diagnostic tests
An MI is a life-threatening cardiac emergency. Nurses should anticipate and advocate with their medical colleagues for definitive tests (serial troponin tests, 12-lead ECG, and cardiac catheterization). The most significant sign for definitive diagnosis of an MI is a positive troponin test with ST changes in at least two contiguous leads.
Troponin tests. Troponin is a protein that causes contraction in skeletal and cardiac muscle fibers (normal values are 0 to 0.4). It’s released from the heart muscle when injury occurs. A positive troponin test of >0.4 means the heart has been injured (the test is 99% specific to cardiac injury). Other diagnoses for a positive troponin test include atrial fibrillation, heart failure, myocarditis, damage to the heart from some cancer treatment medications, pulmonary embolism, chronic kidney disease, and chronic obstructive pulmonary disease. These conditions typically result in conditions related to Type 2 MI because they have ST depression, not elevation.
12-lead ECG. An ECG is an electronic depiction of energy waves moving in 12 directions through the heart. An alteration in two contiguous leads means that a change has occurred in the area of the heart supplied by that specific blood vessel. ST elevation indicates a complete block (Type 1 MI). In most cases, ST depression indicates a partial block or a low-flow state such as shock (Type 2 MI). (See ST elevation and depression.)
ST elevation and depression
ST elevation indicates a complete block of one more coronary arteries. ST depression indicates a partial block.
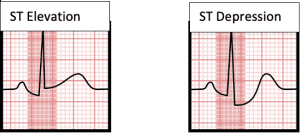
Type 1 MI ST elevation is an emergency; Type 2 MI ST depression is urgent.
Cardiac catheterization: Heart catheterization, the gold standard for evaluating cardiac disease, uses injected dye and imaging to accurately measure ejection fraction and to view muscle contractions and arterial blood flow through the heart.
If cardiac catheterization shows significant narrowing, a PCI may be performed. In this procedure, a small stent placed on an expandable balloon is guided into the narrowed artery. The stent is then expanded, providing support and widening the artery to improve blood flow. The goal for patients with Type 1 MI is to achieve PCI within 90 minutes.
Nurse’s role
When a patient arrives in the ED and reports chest pain, the nurse should perform an immediate assessment. They also should think of the 12-lead ECG as a sixth vital sign and obtain it within the first 10 minutes of arrival (at the first complaint of chest pain for in-patients). The 12-lead ECG should be repeated every 10 to 15 minutes when suspicion for MI is high. Comparing each ECG with previous ones and noting changes are critical for cardiac-related chest pain identification.
If the 12-lead ECG is unremarkable and cardiac enzymes aren’t elevated, but symptoms continue, the patient should be admitted with continued telemetry, cardiac enzyme, and 12-lead ECG monitoring. If ST segment changes occur and cardiac enzymes become positive, the patient is showing signs of a cardiac event. Most hospitals have RRTs that nurses can call for immediate assistance. The patient’s provider also should be notified.
Initial interventions when STEMI is suspected include the following (nurses should follow their organization’s protocol and provider orders):
• Start an I.V. and place the patient on a heart monitor and pulse oximeter.
• Supply oxygen to maintain levels >90%.
• Follow advanced cardiac life support protocols.
• Administer non-enteric coated aspirin 325 mg (chewed and swallowed or given rectally) unless contraindicated (such as with aortic dissection).
• Complete a focused assessment, including cardiac, neuro, pulmonary.
• Have the checklist for administering fibrinolytic therapy at hand. (Fibrinolytic therapy is indicated for patients who are unable to undergo PCI because the distance to a hospital that offers the procedure is more than 90 minutes away.)
• Draw blood, including biomarkers (for troponin), electrolytes, complete blood count, and anticoagulation studies.
• Ask patients if they are taking any anticoagulants or have any conditions that cause coagulopathy; check their medications for any that can cause coagulopathy such as platelet inhibitors. Coagulopathy may be a contraindication for fibrinolytic therapy.
• Administer medications to correct hypokalemia and hypomagnesemia.
• When cardiac pain is present, administer three sublingual nitroglycerin tablets (0.4 mg): one at a time every 5 minutes (or three aerosol sprays under the tongue every 5 minutes). Be mindful of contraindications for nitroglycerin, including hemodynamic compromise (right ventricular infarction) or phosphodiesterase inhibitors (sildenafil for erectile dysfunction).
• Administer diuretics to treat left heart failure if no contraindications exist.
• Administer a beta blocker if the patient shows no signs of heart failure, hemodynamic compromise, bradycardia, or severe reactive airway disease (beta blockers are contraindicated for cocaine-related chest pain).
• Administer morphine sulfate (2 to 4 mg I.V. slow push every 5 to 15 minutes) for pain.
• Administer a lipid-lowering agent (such as 80 mg of atorvastatin) before PCI if the patient isn’t on a statin. If the patient is on a statin, anticipate switching to atorvastatin 80 mg.
• Administer oral antiplatelet therapy (plus aspirin): clopidogrel for fibrinolytic therapy, ticagrelor for no reperfusion therapy, or ticagrelor or prasugrel with primary PCI.
• Administer anticoagulant therapy (unfractionated heparin or bivalirudin) plus aspirin.
Patient teaching and discharge instructions
Mr. Low is taken to the heart catheterization lab where one stent is placed in the right coronary artery, which has a 90% blockage. He recovers in the cardiac intensive care unit for 1 day and then returns to the cardiac telemetry unit before discharge. Sam meets with Mr. Low to discuss discharge instructions and provide patient education, which includes following a low-fat diet, taking nitroglycerin for chest pain, exercising, managing medication, making lifestyle changes (such as smoking cessation, blood pressure control, and stress management), and scheduling regular medical checkups. Sam also makes a follow-up appointment for the patient. Mr. Low thanks Sam for being with him and keeping him calm when he had his heart attack.
Anita J. White is an acute care clinical nurse specialist at VA Northeast Ohio Healthcare System in Cleveland.
References
Alexander KP, Newby LK, Armstrong PW, et al. Acute coronary care in the elderly, part II: ST-segment-elevation myocardial infarction: A scientific statement for healthcare professionals from the American Heart Association Council on Clinical Cardiology: In collaboration with the Society of Geriatric Cardiology. Circulation 2007;115(19):2570-89. doi:10.1161/CIRCULATIONAHA.107.182616
American Heart Association. Understand your risks to prevent a heart attack. June 30, 2016. heart.org/en/health-topics/heart-attack/understand-your-risks-to-prevent-a-heart-attack
Benjamin EJ, Virani SS, Callaway CW, et. al. Heart disease and stroke statistics—2018 update: A report from the American Heart Association. Circulation. 2018;137(12):e67-492. doi: 10.1161/CIR.0000000000000558.
Berwick DM, Calkins DR, McCannon CJ, Hackbarth AD. The 100,000 lives campaign: Setting a goal and a deadline for improving health care quality. JAMA. 2006;295(3):324-7. doi:10.1001/jama.295.3.324
Cannon CP, Hand MH, Bahr R, et al. Critical pathways for management of patients with acute coronary syndromes: An assessment by the National Heart Attack Alert Program. Am Heart J. 2002;143(5):777-89. doi: 10.1067/mhj.2002.120260
Goldberg RJ, McCormick D, Gurwitz JH, Yarzebski J, Lessard D, Gore JM. Age-related trends in short- and long-term survival after acute myocardial infarction: A 20-year population-based perspective (1975-1995). Am J Cardiol. 1998;82(11):1311-7. doi:10.1016/s0002-9149(98)00633-x
Jneid H, Addison D, Bhatt DL, et al. 2017 AHA/ACC clinical performance and quality measures for adults with ST-elevation and non–ST-elevation myocardial infarction: A report of the American College of Cardiology/American Heart Association Task Force on Performance Measures. J Am Coll Cardiol. 2017;70(16):2048-90. doi:10.1016/j.jacc.2017.06.032
Levine GN, Bates ER, Blankenship JC, et al. 2015 ACC/AHA/SCAI focused update on primary percutaneous coronary intervention for patient with ST-elevation myocardial infarction: An update of the 2011 ACCF/AHA/SCAI guideline for percutaneous coronary intervention and the 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. Catheter Cardiovasc Interv. 2016;87(6):1001-9. doi:10.1002/ccd.26325
McCord J, Jneid H, Hollander JE, et al. Management of cocaine-associated chest pain and myocardial infarction: A scientific statement from the American Heart Association Acute Cardiac Care Committee of the Council on Clinical Cardiology. Circulation. 2008;117(14):1897-907. doi:10.1161/CIRCULATIONAHA.107.188950
Morrow DA, Antman EM, Parsons L, et al. Application of the TIMI risk score for ST-elevation MI in the National Registry of Myocardial Infarction 3. JAMA. 2001;286(11):1356-9. doi:10.1001/jama.286.11.1356
Thygesen K, Alpert JS, Jaffe AS, et al. Third universal definition of myocardial infarction. Circulation. 2012;126(16):2020-35. doi: 10.1161/CIR.0b013e31826e1058















2 Comments. Leave new
This is a great educational article, and as a current nursing student, I appreciate it! Thank you!
This is an excellent cardiac article.