Knowledge can help reduce stigmatization and improve access to care.
- Cases of human Mpox had been considered rare, but current data show rapid spread from human-to-human transmission.
- Transmission requires close contact and the most recent outbreak occurred among self-identified men who have sex with men.
- Nurses have a role to play in identifying patients who’ve been infected, ensuring proper testing, providing care, and advocating to prevent stigmatization.
Learning Objectives
- Describe Mpox and its transmission and symptoms.
- Discuss the diagnosis and treatment of Mpox.
- Discuss patient education strategies for Mpox prevention and treatment.
The author, planners, and peer reviewers of this CNE activity have disclosed no relevant financial relationships with any commercial companies pertaining to this activity. See the last page of the article to learn how to earn CNE credit.
Expiration: 3/1/26
Chris Allen* arrives at a local urgent care center for evaluation of a rash. He tells the nurse that he recently received notification of possible exposure to Mpox. The nurse informs the local health department and calls Mr. Allen’s primary care provider, who refers him to the local hospital emergency department (ED) for consultation with an infectious disease specialist. Sara Ryan, the public health nurse, calls Mr. Allen to gather information before he arrives at the hospital. He tells her that he, along with his two housemates, Wes Boyd and Frank Crawford, all of whom identify as men who have sex with men, attended an out-of-state event. Mr. Allen says that his housemates have been his only close contacts for several weeks before and during the event. When Sara speaks with Mr. Boyd, he states the same. Mr. Crawford tells Sara he had no prior contacts outside of his housemates until attending the event, but that he had intimate contacts, including with his housemates, while at the event.
On the second day of the 4-day event, Mr. Crawford developed a rash on the shaft of his penis and sought sexually transmitted infection (STI) screening at a local clinic. The provider prescribed antibiotics, but all testing was negative. On day five, the men travelled home (2 days before Mr. Allen’s urgent care visit). Currently, Mr. Allen and Mr. Crawford have lesions in the genital regions and arms and new lesions on the arms, chest, and neck. Mr. Boyd reports a sore throat and conjunctivitis. He self-treated the conjunctivitis and feels that it’s improving. He reports no rash.
All three, who are now together in the ED, feel fatigued but have no fever. Before they arrived, Sara notified the ED of their situation. She instructed the ED staff to isolate the men and test them for Mpox. Mr. Allen and Mr. Crawford are swabbed because they have visible lesions, but Mr. Boyd is not. They’re discharged home to await results. None are offered antiviral therapy or recommended for vaccine despite the Mpox contact and current information.
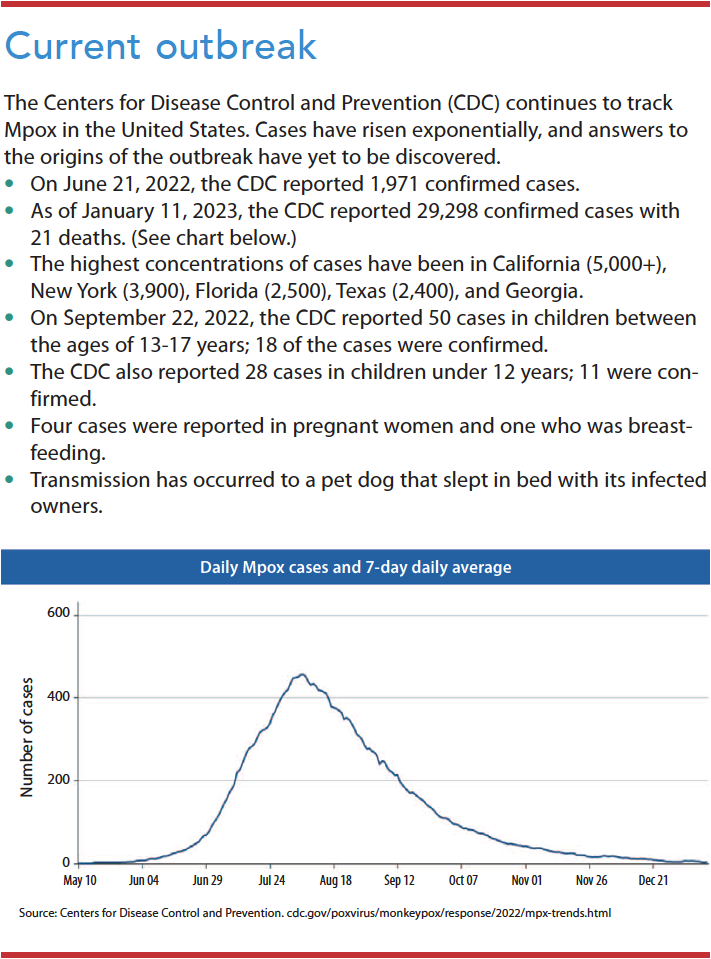
In 2022, several countries, including the United States, experienced an outbreak of Mpox. The Centers for Disease Control and Prevention (CDC) continues to track it. Previously, cases of human Mpox were considered rare. However, current data show rapid spread of the disease from human-to-human transmission. Most cases appear to occur among self-identified men who have sex with men (MSM), but transmission can occur among anyone. Others at risk for the disease include those who are immunocompromised, have certain skin conditions, are pregnant, or are very young. (See Current outbreak.)
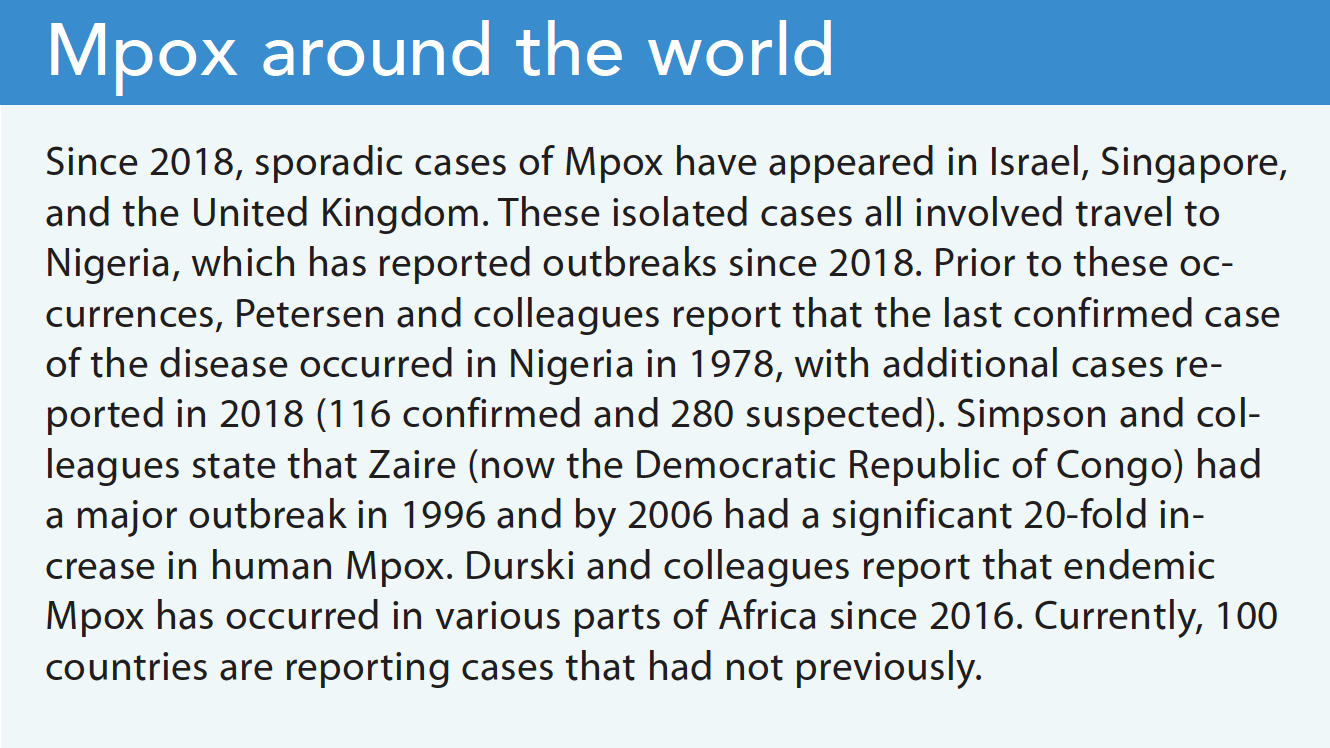
Before 2022, 47 confirmed and probable cases of Mpox were reported in 2003 across six states—Illinois, Indiana, Kansas, Missouri, Ohio, and Wisconsin. According to the CDC, this occurred due to an import of small mammals from Ghana, which then spread to prairie dogs adopted as pets. This resulted in a restriction on importing African rodents, which still exists. The current outbreak represents the first time human Mpox was reported outside of Africa. The CDC reported two additional cases in 2021, both associated with travel to Nigeria. These cases occurred in Texas and Maryland several months apart. (See Mpox around the world.)
Although the recent Mpox outbreak appears to have slowed, nurses should be familiar with its symptoms so they can promptly isolate potentially infected individuals, ensure proper testing, and provide care. Nurses also can advocate for these patients and educate them about infection risks and what they should do if they think they’ve been exposed.
What is Mpox?
The World Health Organization (WHO) defines Mpox as an orthopoxvirus, a virus similar to smallpox but less severe. It’s transmitted from animals to humans and humans to humans. Mpox was first discovered in 1958 as an outbreak of vesicular rashes in captive monkeys brought to Denmark from Africa for research. This finding originally led to calling the disease Monkey Pox. The change to Mpox aims to avoid confusion and stigmatization. Mpox can be found in many animals other than primates, including squirrels, rats, dormice, and other rodents.
Researchers have identified two Mpox subtypes (clades), one of which is less fatal (1%) than the other (10%). The current U.S. outbreak is classified as the milder clade. Many theories exist to explain the emergence of Mpox after the eradication of smallpox and the cessation of vaccination in 1978. One theory posits that waning immunity in the post-smallpox eradication era resulted in the emergence of other orthopoxviruses, including Mpox. However, no actual evidence explains the origins of the current outbreak or why it has appeared in countries that don’t usually report it.
Symptoms
According to the CDC and WHO, Mpox spreads via close contact with an infected animal or person. Human-to-human spread involves skin-to-skin contact with an infected person who displays the Mpox rash, vesicles, or scabs, as well as contact with their saliva, upper-respiratory secretions, and areas around the anus, rectum, and vagina. The risk of infection through contact with contaminated items (such as common surfaces, clothing, and sheets) is low.
Common symptoms include fever, headache, lymphadenopathy (especially submental, submandibular, cervical, or inguinal), muscle aches, and fatigue. These flu-like symptoms (the prodromal stage) lead to a rash that can involve any part of the body, including the mouth, pharynx, and anogenital and urogenital areas. The Mpox incubation period ranges from 5 to 21 days. The prodromal stage, followed by the skin eruption stage to time of healing, can last 2 to 4 weeks.
The rash presents in varying degrees of red flat spots, which then form umbilicated pustules (the hallmark identifier) that crust or scab over before healing. This process occurs over several weeks. Patients may experience secondary skin infections, as well as pneumonitis, encephalitis, or keratitis (for eye involvement). Proctitis (inflammation of the inner lining of the rectum) has occurred in some individuals with anal lesions.
Most patients don’t require hospital admission, unless they’re immunocompromised. Some hospitals have reported admissions for pain management in individuals with anogenital lesions. A child in Florida (under 2 years old) who became infected as a result of close contact with infected caregivers required hospitalization due to disease severity.
Diagnosis
Providers diagnose Mpox using active lesion culture. Samples, collected by vigorous swabbing of lesions, ulcers, or scabs without un-roofing, are sent to commercial labs for polymerase chain reaction testing using sterile, dry polyester or Dacron swabs placed in a dry sterile container and refrigerated or frozen for processing. State health department labs also perform testing, but this use varies. Labs typically report results in 3 to 5 days.
Differential diagnoses include sexually transmitted infections related to new groin lesions and strep throat related to pharyngitis. Lymphadenopathy differentiates Mpox from chickenpox but not herpes simplex infections. Other considerations include syphilis, chancroid, coxsackie virus, molluscum contagiosum, and cryptococcus.
Treatment
Treatment includes postexposure prophylactic vaccination. The federal government has stockpiled two vaccines—Jynneos (preferred because of fewer side effects) and ACAM2000—for smallpox and Mpox. Initially, each state received only limited quantities of Jynneos, but production has since caught up with demand. Guidelines for administering the vaccine are expanding as available vaccine increases. Some states with the largest outbreaks held mass vaccination clinics for vulnerable populations to help slow disease spread. The vaccine can be given up to 14 days after exposure to individuals not experiencing symptoms. Those who’ve received the vaccine show protection against, or minimization of, Mpox symptoms. Researchers believe that individuals who received the smallpox vaccine before its cessation in 1978 also have protection from Mpox and may experience mild symptoms if they do become infected.
After symptoms first appear and a diagnosis is confirmed, treatment focuses on supportive care and symptom management. It also may include antiviral medications or antibody treatment. Tecovirimat, an oral antiviral that’s approved to treat smallpox, is considered an investigational new drug (IND) when used with Mpox and requires state and federal approval before the CDC can dispense it. Antibody treatment, which also requires state and federal approval, is administered via I.V. infusion; it’s reserved for the most severe cases. Providers also should include pain management and treatment of secondary bacterial infections in the plan of care.
Sara calls Mr. Allen, Mr. Boyd, and Mr. Crawford daily to investigate further contacts and monitor symptoms. Mr. Allen describes experiencing more lesions (the original lesions have become umbilicated) as well as some mild discomfort. Mr. Crawford reports that his lesions have healed and that he doesn’t feel ill. Mr. Boyd still has a sore throat, now has lesions on his neck and in his throat, and feels something in his rectum. Only his throat is painful; his eye has improved.
Three days after being seen in the ED, the men receive positive test reports for Mpox. They continue to gather information from their network of friends who also attended the event, all of whom have symptoms. Multiple calls and emails by Sara and her public health office colleagues to get antiviral care for the housemates go unanswered by the initial providers through the weekend. Mr. Allen and Mr. Boyd report increasing discomfort. Sara arranges for further infectious disease consultation after the weekend. The infectious disease provider prescribes gabapentin for pain but declines the request for tecovirimat. The next day, Mr. Allen and Mr. Boyd say that that their pain isn’t controlled, and that the rectal pain is especially bad. They describe it as “constant pressure” and that “bowel movements are like passing shards of glass that take your breath away.” Sara advises them to contact the infectious disease provider for better pain management. Both decline because they feel the provider isn’t taking their symptoms seriously.
Education and public health
Individuals with a known contact to Mpox should monitor for symptoms, avoid close physical contact with others, and take their temperature twice a day for 21 days. They don’t need to quarantine unless they experience prodromal symptoms or a rash. If either occurs, they should isolate until lesions heal, which can take up of 4 weeks.
Healthcare providers must notify local health departments for case investigation as well as close contacts of the patient for prophylactic vaccination of exposed individuals. The role of public health nurses includes case investigation, isolation and quarantine guidelines, and monitoring for fever or development of symptoms in those who’ve been exposed. Public health nurses or health department epidemiologists perform daily check-ins with close contacts to monitor symptoms and provide supportive care. Local health departments arrange grocery delivery and other necessities for infected individuals due to the long isolation period.
Nursing implications
Nurses and other healthcare providers caring for anyone suspected of having or at risk of Mpox should use appropriate personal protective equipment—including N95 masks, gloves, gowns, and eye protection—to prevent contamination of clothing, skin, and mucous membranes. Place infected patients in a private room with the door closed, if safe to do so; negative pressure rooms aren’t necessary. Healthcare exposures can occur when a patient admitted for an unrelated illness develops Mpox symptoms. If you provided care without protective equipment, you should receive postexposure prophylaxis.
Advocate for appropriate care to address painful Mpox lesions. Swabbing lesions for testing can exacerbate pain, so support patients emotionally during the sampling process. For patients with anogenital lesions, offer stool softeners to help relieve pain during bowel movements. Consult with infectious disease specialists for guidance and ordering antiviral medications as appropriate.
On day 10, Mr. Allen tells Sara that he feels much improved from the previous day without any change in medication. He’s been using a combination of coconut, lavender, and tea tree oil with some success in soothing the lesions. He believes that neomycin applied to the penile lesions also helped. He expresses frustration that friends in another state have experienced minimization of their painful symptoms and that they’ve been denied antivirals. He believes the doctors aren’t taking it seriously. Mr. Boyd says he feels worse on day 10; his course of rash and lesions is a few days behind Mr. Allen and Mr. Crawford. He’s optimistic that he’ll improve in the next 36 to 48 hours.
In follow-up text messaging on day 12, Mr. Allen and Mr. Boyd say that they continue to improve. No new symptoms or lesions have appeared, and their pain has diminished. Mr. Crawford is almost completely healed and has no new symptoms.
Advocate to reduce treatment disparity
The MSM population appears to be disproportionately affected by this current outbreak. Theories posit close physical, skin-to-skin contact and multiple sex partners as possible explanations. These theories also hypothesize that this explains why some patients experience genital lesions first as opposed to facial lesions, which the literature previously noted as most common. Past investigations indicated that the Mpox incubation period is 5 to 21 days, but recent cases demonstrate lesions starting within 48 hours of exposure. In addition, the prodromal phase is mild or nonexistent.
The CDC believes the outbreak will remain concentrated in the MSM population as spread in other subpopulations has remained low. Several factors should be considered when trying to determine the trajectory of the outbreak. They include sexual behaviors among high-risk groups and the impact of behavior change in these groups, uptake and effectiveness of vaccine against infection and severe disease, the potential for sustained transmission in non-MSM populations, viral mutation, and the impact of asymptomatic spread of infection. The CDC launched the Mpox Vaccine Equity Pilot program to encourage states to expand vaccine access to disproportionally affected populations. This voluntary mini-grant program allows states to submit proposals detailing programs designed to address disparities and access to vaccination in disproportionately affected communities.
Although regular treatment updates are disseminated to the healthcare community, many providers seem unaware of providing treatment options that fit the symptoms. For example, some providers may be reluctant to prescribe the antiviral if patients aren’t immunocompromised, even though guidelines recommend this treatment for any patient with Mpox symptoms. Other reasons for hesitation may include lack of knowledge of tecovirimat and the IND status of the drug, which requires paperwork for approval. States with higher case counts are ahead of the curve in management of vaccine efforts and antiviral therapies compared to less-affected states. The CDC recently changed the process for acquiring tecovirimat, eliminating some of the redundant paperwork; however, it remains a time-consuming process.
Limited information exists about the experience of patients with Mpox. Many patients describe the rash as initially itchy, similar to chickenpox, but then becoming painful as the lesions become umbilicated. The most painful lesions, as reported by patients, are in the throat and rectal areas. Pain management, beyond over-the-counter medications, is essential. Many patients express frustration with healthcare providers who don’t seem to take them seriously or dismiss the pain they’re experiencing. Nurses must advocate on behalf of this marginalized population, but ultimately providers decide what to prescribe. Combatting misinformation about Mpox can help prevent stigma against the LGBTQ+ community. Remind your colleagues and others that Mpox can affect anyone. It’s an illness of close skin-to-skin or sexual contact regardless of sexual orientation.
The Mpox outbreak evolved quickly but has since stabilized, even in the states with the highest number of reported cases. Prompt information campaigns to the MSM community and vaccination efforts have helped healthcare providers gain control of the outbreak and limit its spread. In states with high numbers of Mpox cases, providers became comfortable with treatment modalities more quickly than those in states with fewer cases did. We still have much to learn about this orthopoxvirus and information to gather from the reported cases and treatment responses to understand the full efficacy of vaccination.
*Names are fictitious.
Cathy Jo Soden is a public health nurse at the Mercer County Division of Public Health in Trenton, New Jersey.
American Nurse Journal. 2023; 18(3). Doi: 10.51256/ANJ032306
Key words: Mpox, monkey pox, prophylactic vaccination, antiviral medication, antibody treatment, stigmatization
References
Centers for Disease Control and Prevention. 2022 Mpox outbreak global map. January 11, 2023. cdc.gov/poxvirus/monkeypox/response/2022/world-map.html
Centers for Disease Control and Prevention. 2022 U.S. map and case count. January 11, 2023. cdc.gov/poxvirus/monkeypox/response/2022/us-map.html
Centers for Disease Control and Prevention. Monkeypox: Updates about clinical diagnosis and treatment. June 24, 2022. emergency.cdc.gov/coca/calls/2022/callinfo_062922.asp
Centers for Disease Control and Prevention. Past US cases and outbreaks. June 6, 2022. cdc.gov/poxvirus/monkeypox/outbreak/us-outbreaks.html
Durski KN, McCollum AM, Nakazawa Y, et al. Emergence of Monkeypox—West and Central Africa, 1970-2017. MMWR. 2018;67(10):306-10. doi:10.15585/mmwr.mm6710a5
Halani S, Mishra S, Bogoch, II. The monkeypox virus. CMAJ. 2022;194(24):E844. doi:10.1503/cmaj.220795
Harris E. What to know about monkeypox. JAMA. 2022;372(23):2278-9. doi:10.1001/jama.2022.9499
New Jersey Department of Health. Monkeypox (mpox). nj.gov/health/monkeypox
Petersen E, Abubakar I, Ihekweazu, C, et al. Monkeypox—Enhancing public health preparedness for an emerging lethal human zoonotic epidemic threat in the wake of the smallpox post-eradication era. Int J Infect Dis. 2019;78:78-84. doi:10.1016/j.ijid.2018.11.008
Rodriquez-Morales AJ, Lopardo G. Monkeypox: Another sexually transmitted infection? Pathogens. 2022;11(7):713. doi:10.3390/pathogens11070713
Simpson K, Heymann D, Brown CS, et al. Human monkeypox—After 40 years, an unintended consequence of smallpox eradication. Vaccine. 2020;38(33):5077-81. doi: 10.1016/j.vaccine.2020.04.062
Tabarsi P. Human monkeypox. Iranian J Med Sci. 2022;47(4)289-90. doi:10.30476/ijms.2022.48507
Walter K, Malani PN. What is monkeypox? JAMA. 2022;328(2):222. doi:10.1001/jama.2022.10259
World Health Organization. Mpox (monkeypox). who.int/health-topics/monkeypox#tab=tab_1

















7 Comments. Leave new
Well written article on a subject I had no information on.
Thank you for your kind comment!
Thank you so much.
Factual information excellent in education and useful future resources.
Factual information on a disease and it’s treatment plan.
Thank you so much.
Great educational site with variety of resources for various jobs.