
A looming shortage of expert nurses requires strategies to accelerate knowledge transfer.
Takeaways:
- Healthcare organizations are facing the challenge of retaining expert knowledge as the nursing workforce transitions in the coming years.
- When expert nurses leave organizations, their critical knowledge of the workplace and the work they perform leaves with them.
- Taking a strategic approach to knowledge transfer can help healthcare organizations manage the risks of lost knowledge and reduce costly surprises.
The latest nursing workforce reports indicate that an adequate supply of RNs exists to meet growing demand. However, according to a 2019 survey of nurses conducted by AMN Healthcare, 20% plan to retire in the next 5 years and 27% plan to leave their current job in the next year. Although the demand for nurses can be met, employers can’t meet the need for experienced nurses. A new type of nursing shortage is emerging—a shortage of expert nurses.
Nursing is a knowledge-intensive profession, and knowledge is more than the accumulation of information. It’s defined as one’s capacity for effective action or decision-making based on information. However, not all knowledge is equal. Expert nurses possess a unique form of tacit knowledge that’s a mix of experiences, values, contextual information, and insight that enhances their decision-making skills. This type of knowledge, also known as “deep smarts,” contains subjective understandings, intuition, and hunches that nurses accrue over time. It’s the knowledge that expert nurses keep in their heads and find difficult to articulate to others.
The cost of lost knowledge
When expert nurses leave organizations, their critical knowledge of the workplace and the work they perform leaves with them. This loss of specialized knowledge is concerning because, according to a report from Panopto, employees spend an average of 8 hours per week re-creating institutional knowledge, resulting in delayed decisions and interventions or missed opportunities for growth or innovation.
Failing to capture departing employees’ knowledge can be costly for any organization. For example, according to Wang and Noe, Fortune 500 companies lose an estimated $31.5 billion annually because of this missed opportunity. Failing to capture the critical knowledge of expert nurses drains healthcare organizations of clinical expertise and institutional awareness that has important implications for innovation, quality, and patient safety. The result is efficiency reductions, innovation capacity limitations, growth strategy threats, and competitor vulnerabilities.
Knowledge transfer framework
Many healthcare organizations have focused their efforts on retaining experienced nurses in the workforce for longer periods, but strategies to accelerate critical knowledge transfer are sparse. Promoting a knowledge sharing culture, investing in appropriate technology and tools, and building a knowledge management infrastructure facilitate knowledge transfer.
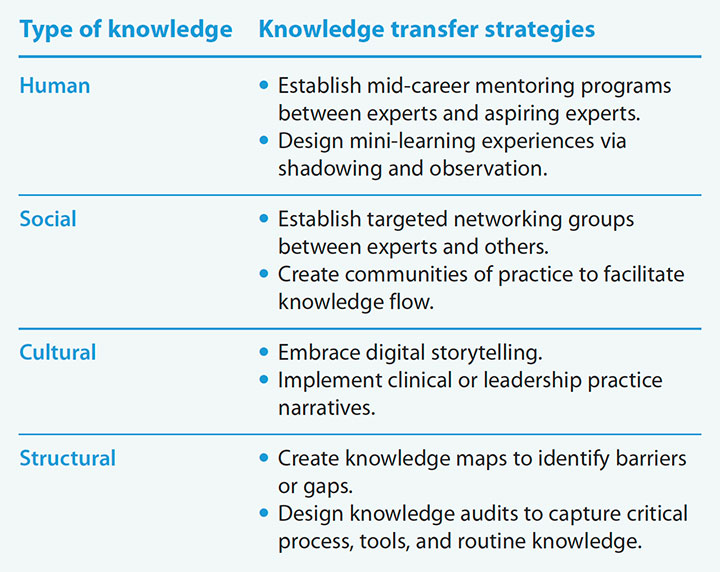
The notion of knowledge transfer in healthcare is in its infancy, but proven and practical strategies can be examined and adopted from other industries. Four distinct categories of tacit knowledge—human, social, cultural, and structural—are critical to performance and should be transferred to aspiring expert nurses. They provide a useful framework for exploring knowledge transfer strategies. (See Knowledge transfer strategies.)
Knowledge transfer strategies
Use these knowledge transfer strategies to develop aspiring nurse experts.
Human knowledge
Human knowledge is the know-how that expert nurses possess. They integrate experience-based patterns with information about the environment and make decisions swiftly and efficiently.
Human knowledge isn’t transferred in a top-down or bottom-up information sharing session. Instead, it’s transferred collaboratively via strategies such as mid-career and structured mentoring programs. In nursing, clinical mentoring commonly is used to transfer knowledge from preceptors to new graduate nurses. Focused mentoring between experts and proteges allows aspiring experts to extrapolate key knowledge. This routine engagement provides opportunities for proteges to learn how to reframe issues and identify alternative solutions to clinical and ethical dilemmas. In addition to focused mentorships, organizations also should consider creating mini-experiences through shadowing and observing to allow aspiring experts to build their capabilities. (See Focused mentoring.)
Focused mentoring
Several approaches to focused mentoring have shown promise in transferring knowledge among nurses. Here are two examples.
- The Legacy Mentors initiative, supported by several large Canadian health authorities and schools of nursing, provided opportunities for expert nurses to transfer knowledge to novices, new hires, and experienced staff. Nurses who were 55 years or older with a wealth of knowledge were selected as Legacy Mentors. They shared critical knowledge through mentorships, educational offerings, and resource materials. According to Clauson and colleagues, this year-long effort to transfer knowledge resulted in improved clinical decision-making and evidence-informed practice.
- The Clinical Mentor Delivery Model, initiated at Scripps Memorial Hospital, invited expert nurses to serve as clinical mentors to experienced and novice nurses. Burritt and colleagues reported that within a year, fiscal savings in patient complications avoidance and improved nurse satisfaction were noted.
Social knowledge
Social knowledge is grounded in relationships that build trust and collaboration between individuals and among teams. Knowledge isn’t developed in isolation but through dialogue. Thus, social knowledge, frequently called “social capital,” can only be developed by working together. The knowledge that resides in these relationships can be transferred by developing a community of practice (CoP) or targeted social networking. A CoP transcends roles and organizational boundaries and provides a structure to connect individuals, foster trust, and facilitate knowledge sharing. For example, a CoP across the Alberta Health Service in Canada allowed knowledge to flow throughout practice domains and programs. In this case, the CoP flourished when it became meaningful to members to grow, collaborate, and achieve goals. Experts also can serve as knowledge brokers to introduce new team members and foster key connections before they leave.
Cultural knowledge
Cultural knowledge is an understanding of the cultural norms and values of an organization. The loss of cultural knowledge is particularly at risk with high turnover among both staff and leadership because new employees aren’t familiar with how things are done in a specific organization. Stories are a powerful means of sharing information. They’re rich in context and can capture knowledge that’s difficult to document. Stacey and Hardy remind us that “stories allow us to step into the shoes of the storyteller and give insight into their journey.”
Experts like to share their knowledge about best practices and lessons learned; however, their stories aren’t preserved, accessible, or reusable. One solution is to capture this key knowledge through digital storytelling or video. Clinical narratives provide an opportunity to illuminate tacit knowledge and offer another strategy to enhance expertise. These narratives frequently are used to augment learning among students, but they also can be used to transfer knowledge.
Structural knowledge
Structural knowledge consists of processes, tools, and routines. Experts possess many techniques for dealing with a variety of situations. However, these techniques may not be formalized or documented. According to the Workplace Knowledge and Productivity Report, a survey of more than 1,000 employees conducted by Panopto (a video-sharing company for business and education) found that 60% of employees lose an average of 5 hours per week looking for information that hasn’t been formally documented. Structural knowledge can be captured and transferred via knowledge mapping, knowledge audits, and structured interviews. (See Mapping and auditing knowledge.)
Mapping an auditing knowledge
Knowledge mapping and auditing can be used to identify, collect, and review critical knowledge.
- Knowledge maps are visual representations of where an organization’s critical knowledge can be found, and they offer insight into strengths and weaknesses. Engineering companies use them to locate expertise and develop mid-career employees into experts.
- Knowledge audits are well-defined technical reports that identify and capture key knowledge. They can be useful tools for gathering critical information that expert nurses don’t perceive as important but may help a unit or organization in the long term.
Take a strategic approach
Healthcare organizations and nurses are rich in knowledge. The loss of expert knowledge through turnover and retirement is widespread. Too frequently, healthcare organizations underestimate the costs associated with the loss of expert nurses’ knowledge. Taking a strategic approach to knowledge transfer can help manage the risks of lost knowledge by reducing costly surprises. AN
Terri Gaffney is an assistant professor at Marymount University in Arlington, Virginia.
References
AMN Healthcare. Survey of registered nurses. 2019. amnhealthcare.com/2019-survey-of-registered-nurses-a-challenging-decade-ahead
Auer AM, Hanson P, Brady-Fryer B, Alati-it J, Johnson AL. Communities of practice in Alberta health services: Advancing a learning organisation. Health Res Policy Syst. 2020. prism.ucalgary.ca/bitstream/handle/1880/112370/12961_2020_Article_603.pdf?sequence=1&isAllowed=y
Burritt JE, Wallace P, Steckel C, Hunter A. Achieving quality and fiscal outcomes in patient care: The clinical mentor care delivery model. J Nurs Adm. 2007;37(12):558-63.
Cathcart EB, Greenspan M. The role of practical wisdom in nurse manager practice: Why experience matters. J Nurs Manag. 2013;21(7):964-70.
Clauson M, Wejr P, Frost L, McRae C, Straight H. Legacy Mentors: Translating the wisdom of our senior nurses. Nurse Educ Pract. 2011;11(2):153-8.
DeLong DW. Lost Knowledge: Confronting the Threat of an Aging Workforce. London: Oxford University Press; 2004.
Gaul P. Shut the door on lost knowledge. TD. 2017;2:20. td.org/magazines/td-magazine/shut-the-door-on-lost-knowledge
Jacobs S. Developing a strategy to facilitate knowledge transfer. Learning Solutions. August 24, 2018. learningsolutionsmag.com/articles/developing-a-strategy-to-facilitate-knowledge-transfer
Leonard D, Swap WC, Barton G. Critical Knowledge Transfer: Tools for Managing Your Company’s Deep Smarts. Boston, MA: Harvard Business Review Press; 2014.
Panopto. 2018. The workplace knowledge and productivity report. panopto.com/resource/valuing-workplace-knowledge/#Report
Stacey G, Hardy P. Challenging the shock of reality through digital storytelling. Nurse Educ Pract. 2011;11(2);159-64.
Starks A. The forthcoming generational workforce transition and rethinking organizational knowledge transfer. J Intergener Relationsh. 2013;11(3):223-37.
Thew J. Chief nursing officers’ view of nurse supply and demand. Health Leaders. August 16, 2019. healthleadersmedia.com/nursing/chief-nursing-officers-view-nurse-supply-and-demand
Wang S, Noe RA. Knowledge sharing: A review and directions for future research. Hum Resour Manage Rev. 2010;20(2):115-31.
















1 Comment.
This is a great topic. I retired 7/31/21 after 48 years as a RN. My employer had no interest in what I know. Sadly. I’m not done with working. Starting my business as coach. I’ll be circulating. That said, there will be many of my colleagues moving on or retiring in the coming years. We have a reputation for “eating our young.” That has to stop. We need mentoring, buddy systems from the get-go. We all need mentors and we all need to be mentors to whatever capacity we can. We can’t even agree on credential for entry into practice. We were arguing about that in 1971. As nurses, we have so much knowledge. Medicine could not run without us. Let’s blossom collaborative relationships with each other, patients and with employers. It is worth the effort and could possible make working more fun! Thank you for this timely article