
Early detection and intervention is key for higher survival rates.
Takeaways:
- Late identification and recognition of melanoma lead to worsening health outcomes.
- Nursing patient education requires that nurses understand skin cancer risks, detection, and prevention.
- Nurses are in key positions to provide the education patients need to self-detect potential skin cancer and take preventive steps.
CNE
1.5 contact Hours
Learning Objectives
- Describe patient assessment for melanoma.
- Compare the subtypes of melanoma.
- Discuss strategies for skin cancer prevention.
The author and planners of this CNE activity have disclosed no relevant financial relationships with any commercial companies pertaining to this activity. See the last page of the article to learn how to earn CNE credit.
Expiration: 4/1/24
Skin cancer is the most commonly diagnosed cancer in the United States and around the world. According to the American Academy of Dermatology, approximately one in five Americans will develop a basal cell carcinoma (BCC), squamous cell carcinoma (SCC), or a melanoma skin cancer in their lifetime. Melanoma, which was once thought to be uncommon, is the most serious type of skin cancer. It accounts for 75% of deaths associated with cutaneous cancers. (See Melanoma facts.) The skin cancer burden in the United States continues to rise, creating a substantial annual cost for treatment and management.
Melanoma facts
Melanoma has been identified as a global health burden.
- Americans have experienced a 200% increase in melanoma diagnoses since the 1970s.
- New melanoma cases are estimated to grow by 2% annually, and an estimated 100,000 Americans received the diagnosis in 2020.
- Lifetime risk of melanoma is 1:40 for Whites, 1:200 for Hispanics, and 1:1,000 for Blacks.
- The estimated annual cost of treating cutaneous cancers in the United States is roughly $8 billion.
- 10% of individuals diagnosed with melanoma have a positive family history of the disease.
- Individuals who use a tanning bed before age 35 years have a 75% higher risk for melanoma.
- Among women, melanoma is more common in those who are younger than 50; among men, it’s more common in those who are older than 50.
- The National Cancer Institute ranks melanoma as the fourth most commonly diagnosed cancer among the general US population (63 is the average age at time of diagnosis).
- In the United States, melanoma ranks #1 in cancer diagnosis for individuals 25 to 29 years of age.
- The estimated U.S. death rate from melanoma is 4,600 for men and 2,200 for women.
Source: Melanoma Research Alliance
Prevention strategies and early recognition, diagnosis, and treatment of melanoma can lower the disease incidence. Nurses’ role in primary and secondary prevention measures—including assessments, risk screenings, and patient education—can improve patient outcomes and help reduce healthcare costs. In addition, advanced practice RNs who perform annual skin exams have an opportunity to identify, detect, and biopsy suspicious skin lesions; collaborate in care; and make timely referrals. Melanoma is easily treated when it’s identified at an early stage, making early diagnosis key to increased survival rates.
Skin
The skin is the largest organ in the body. It protects internal structures from the environment (including ultraviolet [UV] radiation) and harmful pathogens, and it helps the body regulate moisture, control temperature, and promote vitamin D synthesis.
The skin consists of three main layers: the epidermis (top layer), the dermis (middle layer), and the hypodermis (fat layer). Skin cancer is categorized as nonmelanoma (for example, BCC and SCC) and melanoma. When skin cancer occurs, it initially affects one of three types of cells (squamous, basal, and melanocytes) within the epidermis. In a patient with melanoma, cancer cells form in the melanocytes. Melanoma can arise from a current skin lesion or nevus that progressively changes or as a new lesion (de novo).
Skin cancer risk factors
According to the American Cancer Society, patient factors that influence the risk for skin cancer, including melanoma, are UV radiation exposure from natural (excessive sun exposure) and artificial (tanning bed) sources, personal history of blistering sunburns, family or personal history of skin cancer, genetic predisposition, and other hereditary factors including light skin and red or blonde hair.
Skin cancer signs
The most common sign of skin cancer is change, including changes to a current nevus; a skin lesion that’s bleeding, ulcerated, or won’t heal; a satellite mole; a new skin lesion that stands out on inspection of the skin; or a growth that meets the ABCDE mnemonic criteria, which describes clinical signs of melanoma: Asymmetry, Border irregularity, Color variation, Diameter, and Evolving. (See ABCDE mnemonic.)
ABCDE mnemonic
Nurses, providers, and patients can use this mnemonic to identify skin cancer.
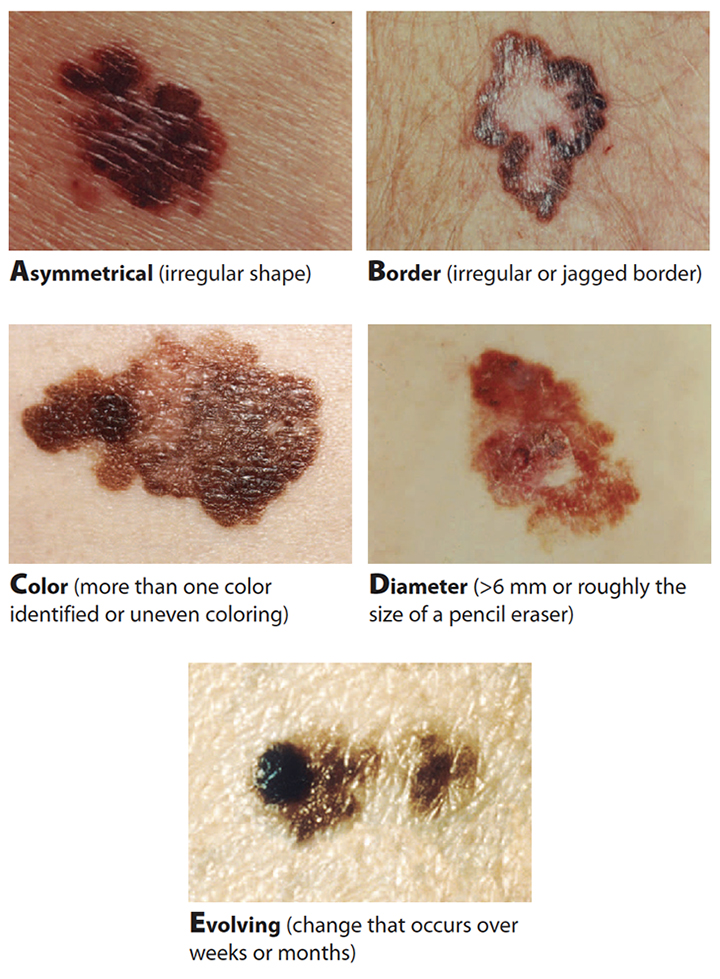
The mnemonic can be combined with the ugly duckling sign, which refers to a spot that’s different from other cutaneous lesions and should prompt suspicion of melanoma. Nurses can use these indicators to improve early melanoma detection and teach them to patients to increase awareness and identification of potential melanomas. Nurses also need to know the difference between nevi and the various subtypes of melanoma.
Nevi
A nevus (also referred to as a common mole) is a skin lesion made up of melanocyte clusters. These noncancerous lesions can range from pink to dark brown and can be either flat or raised.
Dysplastic nevus
 Dysplastic nevi have a 5% to 20% chance of developing into melanoma. They’re typically larger than 6 mm and have irregular or ill-defined fading borders. They can be pink, tan, brown, or black. Dysplastic nevi occur most frequently in sun-exposed areas, including the trunk and upper extremities; however, they also can develop in protected areas such as the scalp, breasts, buttocks, genitalia, palms, and soles of the feet. The lesions can occur throughout a person’s life, and their history frequently includes a first- or second-degree relative with a melanoma diagnosis.
Dysplastic nevi have a 5% to 20% chance of developing into melanoma. They’re typically larger than 6 mm and have irregular or ill-defined fading borders. They can be pink, tan, brown, or black. Dysplastic nevi occur most frequently in sun-exposed areas, including the trunk and upper extremities; however, they also can develop in protected areas such as the scalp, breasts, buttocks, genitalia, palms, and soles of the feet. The lesions can occur throughout a person’s life, and their history frequently includes a first- or second-degree relative with a melanoma diagnosis.
Individuals with a dysplastic nevus should have yearly skin exams that include baseline photography and updates. Lesions that change should be biopsied, and the patient should be referred to a dermatology specialist for removal.
Melanoma
Incidences of melanoma continue to increase among all age groups. Genetic predisposition can play a role in its development but accounts for only 15% of cases. UV radiation exposure continues to be the primary risk factor. According to the Centers for Disease Control and Prevention, when melanoma is recognized early and appropriately treated, the 5-year survival rate is 98% to 99%.
Melanoma subtypes include superficial spreading melanoma (SSM), nodular, lentigo maligna (LM), LM melanoma (LMM), acral lentiginous melanoma, and amelanotic melanoma.
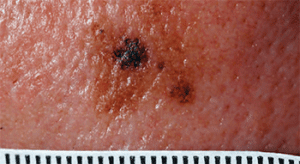
Superficial spreading melanoma
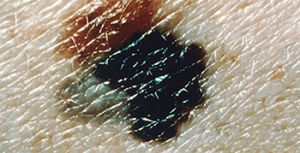 SSM accounts for 70% of melanoma diagnoses and can affect adults of all ages. It has a peak incidence during the fourth and fifth decade of life, but most commonly occurs in adults between 25 and 29 years old and among those with fair skin.
SSM accounts for 70% of melanoma diagnoses and can affect adults of all ages. It has a peak incidence during the fourth and fifth decade of life, but most commonly occurs in adults between 25 and 29 years old and among those with fair skin.
In men, the most common SSM location is the upper back; in women it’s the lower legs. In the early stages, SSM (which can arise from a current mole) appears flat or slightly raised with irregular color distribution and an asymmetric border. Late-stage SSM slowly expands peripherally, and color changes include tan, brown, black, red, pink, and white. Invasive SSM typically occurs on the trunk, head, or neck with vertical growth in the dermis. SSM can take several years to become invasive.
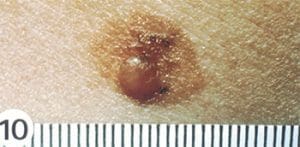
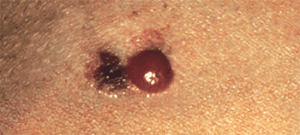
Nodular melanoma
 Nodular melanoma ranks as the second most common melanoma subtype, accounting for 10% to 15% of diagnoses. It’s aggressive, fast-growing, and invasive, thus having a higher chance of metastasis at the time of diagnosis.
Nodular melanoma ranks as the second most common melanoma subtype, accounting for 10% to 15% of diagnoses. It’s aggressive, fast-growing, and invasive, thus having a higher chance of metastasis at the time of diagnosis.
Nodular melanoma lesions are uniformly blue–black, blue–red, or pink–red; 5% lack pigment (amelanotic). The most common locations for these lesions are the trunk, head, and neck. They frequently occur de novo.
Lentigo maligna
LM is the most common melanoma subtype and is defined as in situ (confined to the epidermis). It’s frequently seen in adults over age 40 (with a peak in the seventh and eight decades of life [median age 65]) with fair, chronically sun-damaged skin. The most common lesion locations are the cheek, head, and neck, but they also can occur on the extremities (most commonly in women) and the back (most commonly in men).
LM typically appears as smooth, nonpalpable skin lesions with irregular light brown or tan color. When peripheral growth occurs, LM will have multiple brown and tan variations. LM lesions also may appear patchy and have a noncontiguous pattern. The slow progression of LM can range from 5 to 15 years before it becomes invasive. Most patients are asymptomatic, but advancing LM can cause pain, burning, itching, or bleeding.
Lentigo maligna melanoma
 LMM (invasive LM) is rare (4% to 15% of melanoma cases) and occurs almost exclusively on sun-exposed skin (head, neck, nose, cheeks). The median age for diagnosis is 65 years. The average LMM lesion size is 3 to 6 cm, but they can grow larger and typically have a 1 mm to 2 cm nodular component. The lesions are flat and irregular with mottled or variegated pigment patterns.
LMM (invasive LM) is rare (4% to 15% of melanoma cases) and occurs almost exclusively on sun-exposed skin (head, neck, nose, cheeks). The median age for diagnosis is 65 years. The average LMM lesion size is 3 to 6 cm, but they can grow larger and typically have a 1 mm to 2 cm nodular component. The lesions are flat and irregular with mottled or variegated pigment patterns.
Chronic UV exposure causes high mutation rates in LMM, which leads to an estimated 30% life-time risk of progression from LM to LMM. The rate of LMM progression to invasive melanoma is 5%.
Acral lentiginous melanoma
 In the United States, acral lentiginous melanoma is the most common type of melanoma in Black, Hispanic, Native American, and Japanese populations. Median age for occurrence is 65 years, and it affects men and women at the same rate. Sun exposure and UV radiation aren’t believed to be a factor for developing acral lentiginous melanoma.
In the United States, acral lentiginous melanoma is the most common type of melanoma in Black, Hispanic, Native American, and Japanese populations. Median age for occurrence is 65 years, and it affects men and women at the same rate. Sun exposure and UV radiation aren’t believed to be a factor for developing acral lentiginous melanoma.
Lesions appear as black or brown discolorations on the soles of the feet (the most common site), palms of the hands, and under the fingernails and toenails; 60% of patients have subungual (under the fingernail) or plantar lesions. The lesions spread peripherally before deep-tissue invasion occurs. Because acral lentiginous melanoma diagnosis isn’t common, it’s frequently discovered in the late stages.
A variant of acral lentiginous melanoma is subungual melanoma, which involves the great toe or thumb. It arises from the nail matrix and has a positive Hutchinson’s sign (pigmentation on the proximal nail fold and nail plate).
Amelanotic melanoma
 Amelanotic melanoma (1% to 8% of melanoma diagnoses) occurs from genetic changes in DNA that form malignant melanocytes. The reasons for these changes aren’t well understood, but amelanotic melanoma cells lack pigments seen in other types of melanoma. Lack of pigmentation occurs when cells can’t produce mature melanin clusters. Risks for amelanotic melanoma include light skin, chronic photodamage from sun-exposed skin, and increased age; however, it also occurs in young children.
Amelanotic melanoma (1% to 8% of melanoma diagnoses) occurs from genetic changes in DNA that form malignant melanocytes. The reasons for these changes aren’t well understood, but amelanotic melanoma cells lack pigments seen in other types of melanoma. Lack of pigmentation occurs when cells can’t produce mature melanin clusters. Risks for amelanotic melanoma include light skin, chronic photodamage from sun-exposed skin, and increased age; however, it also occurs in young children.
Amelanotic melanoma lesions appear as enlarging pink to red macules, papules, or nodules with well- or ill-defined borders. Any subtype of melanoma can become amelanotic.
Melanoma staging
Melanoma staging is based on the American Joint Committee on Cancer staging system, which includes tumor size, lymph node involvement, and metastasis. In 2016, the guidelines incorporated evidence-based prognostic factors, including the Breslow Depth and the Clark Level.
The Breslow Depth measures how far melanoma has invaded the cutaneous tissue. It also directly correlates with the risk of death associated with the melanoma tumor. It’s vertically measured in millimeters from the top of the superficial ulceration (granular layer) to the deepest point of tumor involvement. This measurement is a strong predictor of patient outcome; thicker melanomas have a higher chance of metastasizing.
The Clark Level describes the melanoma depth and can help predict the outcome for thin tumors. The levels range from 1 to 5 (in situ, invading the papillary dermis, filling the papillary dermis, invading the reticular dermis, and invading the subcutaneous tissue). The higher the level, the greater the risk of metastasis.
Nursing implications
Nurses play a key role in preventing and detecting melanoma and other types of skin cancer, as well as in caring for patients who’ve been diagnosed with the condition.
Prevention
Counseling patients can help them understand the steps they can take to keep themselves safe and increase adherence to skin cancer prevention practices. (See Protection for prevention.) The education you provide about sun protection and skin self-exams can help reduce a patient’s risk of skin cancer and increases the chances of early detection.
Protection for prevention
Skin protection measures can help reduce the risk of skin cancer, including melanoma. Advise patients to take these precautions to reduce their exposure to ultraviolet radiation when outdoors.
- Avoid sun exposure at peak times (10 am to 4 pm).
- Decrease the amount of time spent in the sun.
- Seek shade while outdoors.
- Wear sunscreen (at least 30 SPF).
- Reapply sunscreen every 2 hours with heavy sweating or swimming.
- Wear protective clothing, including hat, sunglasses, long sleeve shirts, and pants.
- Avoid tanning beds.
Epidemiologic data suggest that using sun protection and reducing sun exposure have the greatest impact on reducing the incidence of melanoma.
Advise patients to perform monthly skin self-exams, especially if they’re at risk for skin cancer (for example, if they have a compromised immune system, family history of skin cancer, excessive tanning, or repeated sunburns). All they need is a well-lit room and a mirror. (See Skin self-exam: Step-by-step.)
Skin self-exam: Step-by-step
Because skin cancer comes in many shapes and sizes, patients should learn to recognize skin changes and new spots and to contact their provider about any concerns. Instruct patients in skin self-exam best practices, and explain that examining their skin regularly will help in early cancer identification.
- The best time to perform a skin self-exam is after a bath or shower.
- Check for moles, blemishes, or birthmarks from the top of the head to the toes.
Step 1: Do the following while standing and facing a mirror.
- Check face, ears, neck, chest, and belly (women should lift their breasts to check underneath).
- Check underarm areas, both sides of the arms, tops and palms of hands, in between fingers, and under fingernails.
Step 2: Do the following while sitting down.
- Check the front of thighs, shins, tops of feet, in between toes, and under toenails.
- Use a hand mirror to look at the bottoms of the feet, calves, and backs of thighs (first checking one leg and then the other).
- Use a hand mirror to check buttocks, genital area, lower and upper back, and the back of neck and ears (it may be easier to look at the back in a wall mirror using a hand mirror).
- Use a comb or hair dryer to part hair and check the scalp.
Patient care
An estimated 5% to 10% of patients who’ve been diagnosed with melanoma will develop a second invasive melanoma in their lifetime. For that reason, nursing care focuses on education, regular follow-up appointments, and collaboration with a dermatology specialist.
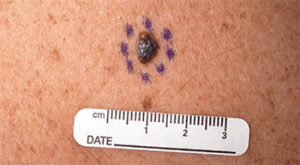
Your exam of a patient who’s been diagnosed with skin cancer should include a full health history, focusing on risk and detection, and a complete skin exam. Document all lesions (including their location, color, size, and pattern), photograph them, and note local landmarks. In addition, palpate the patient’s lymph nodes.
Providers will order a punch biopsy (extending into subcutaneous tissue) of suspicious lesions. A Breslow Depth >1 mm requires an immediate referral to a dermatologic, plastic, or general surgeon for large margin dissection and lymph node biopsy.
Patient role and barriers
Patients play a role in their own healthcare outcomes, and nurses can directly impact a patient’s knowledge and influence their behavior. Patient-related skin cancer treatment delays include patient behavior; an inability to see lesions; inadequate knowledge of melanoma signs, symptoms, and risks; and not performing skin self-exams. According to Avilés-Izquierdo and colleagues, patients without adequate education about skin cancer risk factors and prevention measures who self-detected melanoma were found to seek care with late-stage disease. The relative 5-year survival rate for melanoma found in early, local stages is 98%, but for melanoma that’s metastasized, survival rates drop to roughly 25%. Education that targets primary and secondary prevention measures (sun protection, ABCDE mnemonic, ugly duckling sign, and skin self-exams) can improve early detection of melanoma.
Influence change
Nurses, patients, and communities must support initiatives to inform the public about melanoma and other skin cancers to increase awareness and positively influence changes in sun protective behaviors. Healthcare interventions that reduce patient barriers will improve early detection and treatment, reduce morbidity, and increase survival rates of patients diagnosed with melanoma.
Editor’s note: All photography is courtesy of the National Cancer Institute.
Access references at myamericannurse.com/?p=74425.
Kathileen Boozer is an assistant clinical professor at Louise Herrington School of Nursing at Baylor University in Waco, Texas.
References
Aleo G, Bagnasco A, Cozzani E, et al. Sun-safe behaviours, personal risk, level of concern, and knowledge about cutaneous melanoma in Italy: Time for social marketing? J Prev Med Hyg. 2020;61(2):E246-58. doi:10.15167/2421-4248/jpmh2020.61.2.1484.
American Academy of Dermatology Association. Melanoma. aad.org/media/stats-melanoma
American Cancer Society. Melanoma of the skin. 2020. https://cancerstatisticscenter.cancer.org/?_ga=2.152466873.1874507167.1610237796-1035398239.1590779879#!/cancer-site/Melanoma%20of%20the%20skin
Avilés-Izquierdo JA, Molina-López I, Rodríguez-Lomba E, Marquez-Rodas I, Suarez-Fernandez R, Lazaro-Ochaita P. Who detects melanoma? Impact of detection patterns on characteristics and prognosis of patients with melanoma. J Am Acad Dermatol. 2016;75(5):967-74. doi:10.1016/j.jaad.2016.07.009
Centers for Disease Control and Prevention. Melanoma of the skin statistics. January 21, 2021. cdc.gov/cancer/skin/statistics/
Goodman H, Pacheco C, Loescher L. An online intervention to enhance nurse practitioners’ skin cancer knowledge, attitudes, and counseling behaviors: A pilot study. J Dermatol Nurses Assoc. 2018; 10(1):20-8. doi:10.1097/JDN.0000000000000367
Guerra KC, Zafar N, Crane JS. Skin cancer prevention. StatPearls. August 22, 2020. ncbi.nlm.nih.gov/books/NBK519527
Hartnett PD, O’Keefe C. Improving skin cancer knowledge among nurse practitioners. J Dermatol Nurses Assoc. 2016;8(2):123-8. doi:10.1097/JDN.0000000000000206
Linos E, Katz KA, Colditz GA. Skin cancer—The importance of prevention. JAMA Intern Med. 2016;176(10):1435-6. doi:10.1001/jamainternmed.2016.5008
Lucas AS, Chung E, Marchetti MA, Marghoob AA. A guide for dermatology nurses to assist in the early detection of skin cancer. J Nurs Educ. 2016;6(10). doi:10.5430/jnep.v6n10p71
Melanoma Research Alliance. Melanoma statistics. curemelanoma.org/about-melanoma/melanoma-statistics-2
National Association of School Nurses. Prevention of skin cancer due to ultraviolet exposure – The role of the school nurse. January 2018. www.nasn.org/advocacy/professional-practice-documents/position-statements/ps-skin-cancer
National Cancer Institute. Melanoma Treatment. December 1, 2020. ncbi.nlm.nih.gov/books/NBK65950
Perry M. Assessing and managing malignant melanoma in primary care. Independent Nurse. July 17, 2019. independentnurse.co.uk/clinical-article/assessing-and-managing-malignant-melanoma-in-primary-care/217486/
Seité S, del Marmol V, Moyal D, Friedman AJ. Public primary and secondary skin cancer prevention, perceptions and knowledge: An international cross-sectional survey. J Eur Acad Dermatol Venereol. 2017;31(5):815-20. doi:10.1111/jdv.14104
Sideris E, Thomas SJ. Patients’ sun practices, perceptions of skin cancer and their risk of skin cancer in rural Australia. Health Promot J Austr. 2020;31(1):84-92. doi:10.1002/hpja.253.
Skin Cancer Foundation. Skin cancer facts & statistics. January 13, 2021. skincancer.org/skin-cancer-information/skin-cancer-facts
Vij A. Disease management: Melanoma. Cleveland Clinic Center for Continuing Education. September 2018. clevelandclinicmeded.com/medicalpubs/diseasemanagement/dermatology/cutaneous-malignant-melanoma
Ward WH, Farma JM, eds. Cutaneous melanoma: Etiology and therapy. December 21, 2017. ncbi.nlm.nih.gov/books/NBK481860
Yousef H, Alhajj M, Sharma S. Anatomy, skin (integument), epidermis. StatPearls. July 27, 2020. ncbi.nlm.nih.gov/books/NBK470464

















