Bridging the gap requires nurse intervention.
Individuals within underserved populations face many hurdles to healthcare. They lack access, experience disparities in health literacy, and must consider how they prioritize healthcare with limited resources. Included among these priorities are medications. This month’s CNE article discusses how nurse interventions—assessments, individualized interventions, and collaborative decision making—can help bridge the gap for patients who frequently must make difficult choices about their healthcare without adequate knowledge or access.
Other articles in this issue cover topics ranging from hospital at home, foot care nurse specialists, and palliative care in heart failure to optimizing electronic health records, building positive-thinking skills, and implementing a unique onboarding approach.
Learning Objectives
- Describe why underserved populations are at higher risk for medication nonadherence.
- Discuss medication adherence strategies that nurses can implement with patients.
- Describe advocacy measures to address medication nonadherence in underserved populations.
The authors and planners of this CNE activity have disclosed no relevant financial relationships with any commercial companies pertaining to this activity. See the last page of the article to learn how to earn CNE credit.
Expiration: 12/1/25
Takeaways
- Medication nonadherence, a substantial public health concern, results in morbidity, mortality, and healthcare expenditures.
- Medication nonadherence among underserved populations results from disparities in health literacy, lack of access, and different priorities for those with limited resources.
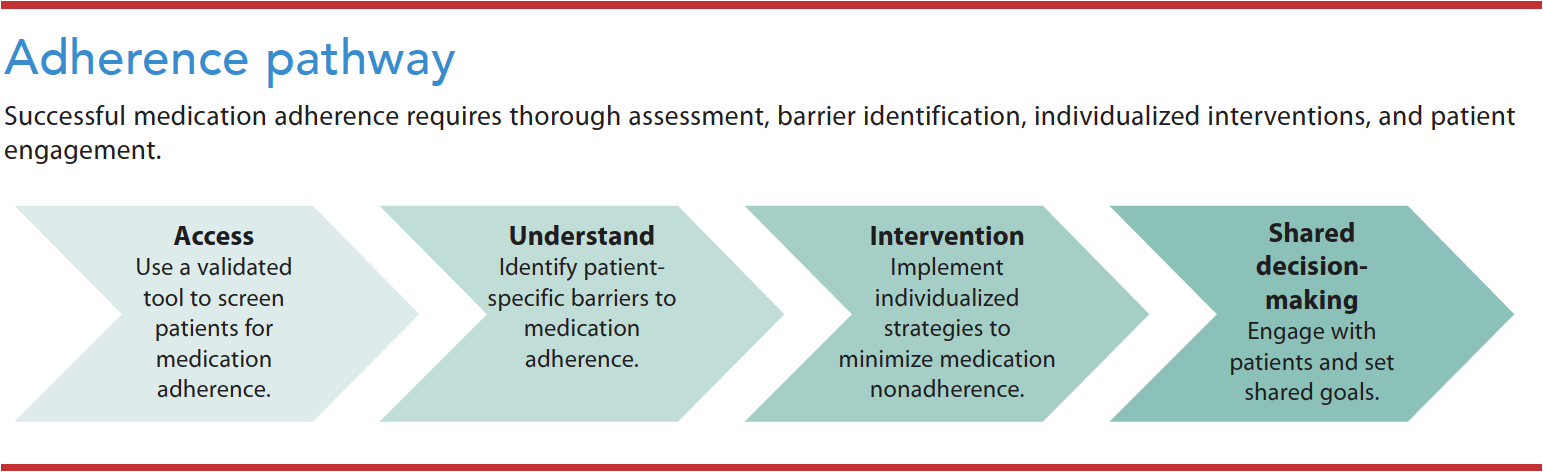
- Improving medication adherence requires thorough assessment, barrier identification, individualized interventions, and patient engagement.
Carl Johnson*, a 74-year old Black man with a medical history of chronic systolic heart failure as a result of ischemic cardiomyopathy, arrives at the hospital via ambulance with acute-on-chronic heart failure. During the admissions process with the primary nurse, Mr. Johnson discusses the events that led him to the hospital as well as his medical, surgical, and social history. The nurse also performs a medication reconciliation.
Mr. Johnson, who lives alone in rural North Carolina about an hour from the hospital, lost his wife to breast cancer about 3 months ago. His wife helped him with his healthcare needs, including scheduling follow-up appointments, collecting his prescriptions from the pharmacy, placing medications in a pillbox, and reminding him when to take then. Mr. Johnson says that since his wife died, his health has taken a turn for the worse and that he’s sad. He can’t refill the pillbox because arthritis in his hands makes it difficult to open pill bottles. In addition, he can’t drive because of bilateral cataracts, so he relies on his daughter for transportation. His daughter, a single mother of three school-aged children, works two jobs. These family obligations prevent her from helping her father as much as she’d like. Mr. Johnson cooks for himself, but his meals primarily consist of frozen entrees from the grocery store. Mr. Johnson left high school in the 10th grade to work in a factory. He’s now retired with an income of about $19,000 per year from social security.
During the medication reconciliation, Mr. Johnson reports that he hasn’t taken his furosemide for the past week because he ran out, and he stopped taking lisinopril without consulting his provider because it caused dizziness. He says that he sometimes doesn’t take his nighttime medications, including carvedilol, rosuvastatin, and tamsulosin, because he falls asleep. He also frequently misses doses of his hydralazine and isosorbide dinitrate because they’re three times a day. Mr. Johnson wonders if he really needs these medications because his blood pressure has been “okay.” He states that his provider recently prescribed a new medication, empagliflozin, but he can’t afford it because his insurance won’t cover the drug. Otherwise, he reports taking medications as prescribed including aspirin, spironolactone, a multivitamin, ferrous sulfate, zinc, and coQ-10. He sees his primary care physician, who prescribes all of his medications, every 6 months.
Medication nonadherence, a substantial public health concern, results in morbidity, mortality, and healthcare expenditures. A global review of nonadherence suggests that, among developed countries with access to medications, most patients experience the ill effects of not taking them “in accordance with agreed-upon recommendations.” Methods for measuring adherence vary greatly and may not account for systematic failures in determining accuracy and specificity, but research by Neiman and colleagues suggests that the scope of the global problem reaches 40% to 50% of medications that aren’t taken as prescribed. In the United States alone, rates are reported to be as high as 50% to 60%.
Medication nonadherence among underserved populations—as a result of fundamental disparities in health literacy; medication access and the ability to pay, pick-up, and consistently renew prescriptions on time; and differences in health-related priorities for those with limited resources—presents unique challenges for nurses. According to Lam and Fresco, medication nonadherence results in ineffective treatment, costly diagnostic tests, and therapy escalation. These downstream effects create particular challenges for the underserved, who interact less frequently with providers and have fewer opportunities to engage in medication reconciliation, thus creating a patient safety issue. Improving medication adherence in underserved populations is essential to improving patient outcomes. (See Prevalence and significance.)
Prevalence and significance
Medication nonadherence, a common issue among many populations, places a considerable burden on the American healthcare system. Despite actions aimed at improving medication adherence, rates of nonadherence have remained stable over the past several decades. In a review supported by the Agency for Health and Research Quality, patients don’t fill almost one-third of initially prescribed medications and they don’t take half as prescribed by the healthcare provider. In general, medication adherence decreases over time with subsequent refills. Broadly cited literature estimates that, in the United States, 125,000 avoidable deaths and 30% of re-hospitalizations can be attributed to medication nonadherence annually, which results in an estimated $100 to $290 billion in wasted pharmacy, inpatient, outpatient, and emergency department resources. When compared to Europe and Australia, U.S. healthcare costs associated with medication nonadherence are 2- to 10-fold higher.
Medication adherence and nonadherence defined
Medication nonadherence, a complex, multidimensional patient issue, can occur at any point along the healthcare continuum. The World Health Organization (WHO) defines adherence as “the degree to which a person’s behavior corresponds with the agreed recommendations from a healthcare provider.” Agreement to recommendations, a key component of patient education, includes shared decision-making and innovative strategies focused on person-centered goal-setting for up-titration to guideline-directed medication doses designed to achieve optimal therapy benefits. (See Phases of medication adherence.)
Phases of medication adherence
According to Vrijens and colleagues, the process of medication adherence involves three phases: initiation, implementation, and discontinuation. Adherence, from initiation to discontinuation, requires persistence.
- Initiation begins with the first dose taken by the patient. In nonadherence, the patient fails to take the first dose.
- Implementation entails a continuous act in which the patient takes the medication as prescribed by the healthcare provider. Hesitating, omitting, or additional dosing represent nonadherence.
- Discontinuation, the conclusion of adherence, ends therapy.
Medication nonadherence can be intentional or unintentional. Intentional nonadherence results when patients deliberately choose not to take a medication and poses a higher risk due to probable non-modifiable inherent patient beliefs. Unintentional nonadherence typically is associated with carelessness, forgetfulness, or confusing instructions. Among underserved populations, unintentional medication nonadherence is more prevalent and discrete and may result from the inability to secure medications because of lack of access and resources.
In most cases, medication nonadherence is multifactorial and influenced by several factors. According to the WHO, medication nonadherence can exist at the patient, provider, and health system levels. (See Barriers to adherence.)

Barriers to adherence
Barriers to medication adherence include patient, provider, and healthcare system factors.
Patient factors
Patient factors play a significant role in medication nonadherence, with those related to socioeconomics being the most prevalent, especially among underserved populations. Patient factors that can disproportionately affect the underserved include the following:
- Distance to healthcare
- Health literacy
- Homelessness
- Lack of social support or family dysfunction
- Lack of transportation
- Medication costs
- Medication dispensing device or method
- Poverty
- Unemployment
Provider factors
Provider-related factors that increase the risk for medication nonadherence include the following:
- High rates of provider burnout resulting in inadequate continuity
of care - Lack of providers located in areas of greatest need
- Lack of training to assess social determinants of health
Health system factors
Health system factors include the following:
- Insufficient funding for charity care
- Lack of reimbursement
Underserved populations at risk
Underserved populations include individuals in the community who experience health disparities and inequities, including limited accessibility to healthcare with fewer services and resources and little awareness of the healthcare delivery system. Underserved populations include older adults, some ethnic minorities, non-native English speakers, those who live in rural areas, individuals with low incomes, and those with low literacy. Social determinants of health—such as housing, income, access, and literacy—directly impact an individual’s health and contribute to health disparities and inequities. Medication nonadherence results in poor health outcomes, including disease progression, increased healthcare costs, and high morbidity and mortality.
Medication adherence strategies
Nurses can help close the health disparity gap for patients in underserved populations by promoting action and intervention to improve characteristics amenable to change. Collaboration with other healthcare providers can aid in creating interprofessional care pathways that incorporate strategies to minimize medication nonadherence.
Practice
Medication adherence is modifiable with the implementation of appropriate interventions. In a systematic review and meta-analysis of randomized controlled trials by Santo and colleagues, implementation of nonadherence interventions indicated improved future adherence. Nurses should use patient-centered interventions to create individualized care plans. Researchers have proposed several interventions based on identified barriers. Conn and colleagues reported that implementing a combination of interventions, rather than a single intervention in isolation, can help overcome barriers more effectively. (See Adherence pathway.)
Nurses practice in various settings and roles in which medication adherence can be addressed. They can use their specialized skills (including assessment) and appropriate technology to develop a sophisticated plan of care that promotes medication adherence.
Assessment. Several leading organizations, including the American Heart Association and the American College of Cardiology, support assessment to identify medication nonadherence among underserved populations and implement patient strategies to address it. Nurses can easily integrate standardized assessment using validated and feasible tools to support critical clinical decisions. Stirratt and colleagues identified several tools, including direct observation, rapid point-of-care assay, drug concentration or biomarker levels, self-report, pill-counting, pharmacy refill data, electronic monitoring (such as ingestible sensors or wireless monitors), and clinical response.
No gold standard for medication adherence assessment exists, but self-report remains the most commonly used strategy. Self-report measures can be applied in different populations and settings and provide real-time feedback. Experts have proposed over 40 self-report measures, with each demonstrating specific advantages and limitations. Although subjective, self-report can accurately differentiate between adherence and nonadherence, and can be replicated during each patient interaction to provide substantiated evidence of adherence. Nurses must then determine unique underlying barriers to adherence, and successively intervene with appropriate and tailored clinical interventions. (See Targeted interventions.)
Targeted interventions
Based on individual patient need, the following interventions can help address medication nonadherence.
- Consider alternative treatment options.
- Decrease medication frequency to daily dosing.
- Discontinue unnecessary medications.
- Implement prescription drug coupons and medication sponsorships.
- Investigate low-cost pharmacy programs.
- Involve family and other caregivers in medication education.
- Make referrals to community social work and other community
resources. - Make referrals to home health for medication adherence education.
- Obtain pharmacy costs before prescribing medications.
- Provide a written medication list with schedule grid.
- Provide medication education appropriate to the patient’s health literacy.
- Request blister packaging.
- Schedule in-person follow-up within 7 days of discharge.
- Schedule pharmacy home medication delivery.
- Share care summary with other care providers.
- Schedule telephone follow-up within 3 days of discharge.
Technology. Current healthcare technology continues to advance. Specifically, the ability of the electronic health record (EHR) to positively impact health management, decision-making, care coordination, and patient satisfaction and outcomes can be applied to medication adherence. Documenting the medication adherence assessment in the EHR enhances coordination among providers and facilitates communication of existing issues related to medication adherence. Beyond assessment, the EHR allows the use of decision-making tools such as pharmacy fill data and personalized patient data, which may provide intervention guidance.
Advocacy
As stated in the American Nurses Association Code of Ethics for Nurses with Interpretive Statements, “The nurse promotes, advocates for and protects the rights, health, and safety of the patient.” Nurses have the knowledge and experience to investigate patient issues and propose options to improve outcomes. From the organizational to the national level, nurses should be aware of health policy related to medication adherence in underserved populations. Through advocacy, nurses can support laws and regulations that provide substantial and validated services for the underserved, thereby reducing health disparities and inequities. In addition, nurses should urge policymakers to consider the consequences of poor medication adherence and support advancing policy change to overcome systemic barriers to adherence.
Professional organizations. Professional nursing organizations provide nurses with support for education, networking, and practice. With regard to advocacy, professional organizations aid nurses in collaborating with other nursing professionals who share common interests. By actively participating in professional organizations, nurses can use their leadership skills to influence health policy.
Access to healthcare. All patients should have access to affordable healthcare. In underserved populations, greater demand exists to address healthcare accessibility. Strategies that can increase access include preemptively scheduling appointments, providing referrals to local outpatient providers and services that may assist with medication adherence, synchronizing medication refills, and increasing home support using a caregiver or transitional health support. In addition, telemonitoring or other systems can help maintain open two-way communication between the provider and the patient to enhance interaction and promote patient comfort to express concerns about medication-taking behaviors.
Other medication management interventions include simplifying medication regimens or providing polypills (which contain a combination of several medications), offering 90-day medication supplies, providing prescription delivery services, using generic forms of medications and samples, and connecting patients with financial assistance (such as prescription assistance programs, vouchers, and coupons to reduce medication costs). Advocating for affordability and access in underserved populations is invaluable to medication adherence.
Position statements. Position statements developed by nursing organizations draw attention to significant practice, policy, and social patient issues. Large medical organizations have issued position statements on medication adherence; however, to date, few nursing organizations have issued statements on the topic or how to address its prevalence among underserved populations. The nursing profession must engage others and create awareness among colleagues, key stakeholders, patients, and the general public to improve medication adherence. Greater attention dedicated to nonadherence in underserved populations can help address this public health issue.
Clinical practice guidelines. Clinical practice guidelines can help bridge the gap between research and practice, but currently no such guidelines exist for medication adherence. Providers and nurses must develop clinical practice guidelines that address the specific needs and care of patients within underserved populations, with a focus on assessment, prevention, and management. Guidelines should be structured to provide nurses with easily accessible and relevant strategies for tackling nonadherence.
Patient education
In select populations, nurse-led patient education has been associated with improved patient outcomes, including fostering medication adherence. Studies support the need for patient education to counter suboptimal medication adherence that results from low health literacy (an inability to comprehend healthcare information). Patient education increases engagement and independence, improves chronic disease management, provides information for preventive care, enhances provider–patient relationships, and improves patient satisfaction.
All patient education should be individualized based on identified needs. Structured educational programs for medication adherence, including multimedia or interactive tools and motivational interviewing, can enhance learning in underserved populations. It should include instruction in how to take medications as prescribed, as well as potential negative outcomes of nonadherence.
Nurses also play an important role in promoting medication self-management. Randomized controlled trials have demonstrated that self-management education provides patients with the knowledge and skills to handle their long-term plan of care, and can improve quality of life, help alleviate mental health issues, improve social and economic conditions, and decrease hospitalizations. To promote medication management independence, nurses should work to empower patients to take ownership of their health, including taking medications as prescribed.
Nurse education
Education serves as an effective means for increasing nurse knowledge and skills, and promotes the acceptance and implementation of current evidence-based practice designed to ensure safe, quality patient care aimed at improving outcomes. Medication adherence education and training should begin in nursing school and continue in the clinical setting. Healthcare organizations have an important role to play, including providing nurses with the necessary training and tools to implement strategies that aid nonadherence reduction among patients from underserved populations.
Research
Nurses are instrumental in facilitating engagement and collaboration with others, evaluating current practice protocols, identifying the need for change, organizing evidenced-based research, formulating new practice protocols based on that research, and incorporating research into clinical decision-making. Solutions to medication nonadherence in underserved populations requires further examination. Nurses can conduct this research, focusing on the extent and causes of nonadherence and appropriate interventions for this unique patient population.
Solving a problem
Mr. Johnson has many characteristics that create barriers to medication adherence, including his race, age, comorbidities, multiple medications, low health literacy, inability to pay for medications, and limited access to care. During interprofessional rounding, the nurse shares her assessment with the rest of Mr. Johnson’s primary care team. In response, they implement several interventions during hospitalization to ensure he’s success after discharge.
The provider prescribes once-a-day medications and removes unnecessary medications. To help Mr. Johnson afford empagliflozin, he’s enrolled in a prescription program. The total cost of his medications is now $18 per month.
The nurse and pharmacist conduct medication education, with Mr. Johnson’s daughter joining via telephone. The case manager arranges home health services for medication adherence education and connects Mr. Johnson with community resources through his local church. The local pharmacy provides Mr. Johnson with blister packaging, which is easier to open, and delivers medications to his home.
The discharge nurse gives Mr. Johnson a summary of his medications with a medication schedule grid. She schedules him for follow-up with his primary care physician 5 days after discharge and sends an electronic discharge summary to the primary care physician that outlines the hospital course with pertinent interventions regarding his medication regimen. As part of routine hospital follow-up, a transitional care nurse will call Mr. Johnson 3 days after discharge to address any issues.
Bridge the gap
Medication nonadherence is a complex and costly issue that results in unfavorable outcomes for patients, providers, and the healthcare system. Despite healthcare advances, medication nonadherence remains steady and widespread, and underserved populations are at greatest risk. Adherence requires active and conscious patient participation and collaboration with healthcare providers and the healthcare system. Through practice, advocacy, education, and research, nurses have an opportunity to bridge this healthcare gap.
*Name is fictitious.
Jaime McDermott is an advance practice provider in the division of cardiology at Duke University Hospital in Durham, North Carolina. Bradi B. Granger is a professor at Duke University School of Nursing and director of the Duke Heart Nursing Research Program at Duke University Hospital.
Key words
medication adherence, medication nonadherence, underserved populations, evidence-based guidelines
American Nurse Journal. 2022; 17(12). Doi: 10.51256/ANJ122208
References
Abbasi A, Ghezeljeh TN, Farahani MA. Effect of the self-management education program on the quality of life in people with chronic heart failure: A randomized controlled trial. Electron Physician. 2018;10(7):7028-37. doi:10.19082/7082
American Nurses Association. Code of Ethics for Nurses with Interpretive Statements. American Nurses Association; January 2015.
Cutler RL, Fernandez-Llimos F, Frommer M, Benrimoj C, Garcia-Cardenas V. Economic impact of medication non-adherence by disease groups: a systematic review. BMJ open. 2018;8(1):e016982. doi:10.1136/bmjopen-2017-016982
Fuller RH, Perel P, Navarro-Ruan T, Nieuwlaat R, Haynes RB, Huffman MD. Improving medication adherence in patients with cardiovascular disease: A systematic review. Heart. 2018;104(15):1238-43. doi:10.1136/heartjnl-2017-312571
Kini V, Ho PM. Interventions to improve medication adherence: A review. JAMA. 2018;320(23):2461-73. doi:10.1001/jama.2018.19271
Kleingsinger F. The unmet challenge of medication nonadherence. Perm J. 2018;22:18-033. doi:10/7812/TPP/18-033
Lam WY, Fresco P. Medication adherence measures: An overview. BioMed Res Int. 2015;2015:217027. doi:10.1155/2015/217047
Neiman AB, Ruppar T, Ho M, et al. CDC Grand Rounds: Improving medication adherence for chronic disease management—Innovations and opportunities. Am J Transplant. 2018;18(2):514-7. doi:10.1111/ajt.14649
Stirratt MJ, Curtis JR, Danila MI, et al. Advancing the science and practice of medication adherence. J Gen Intern Med. 2018;33(2):216-22. doi:10.1007/s11606-017-4198-4
Viswanathan M, Golin, CE, Jones CD, et al. Medication adherence interventions: Comparative effectiveness. Closing the quality Gap: Revisiting the state of the science. Evidence Report/Technology Assessment No. 208. Agency for Healthcare Research and Quality. September 2012. effectivehealthcare.ahrq.gov/sites/default/files/pdf/medication-adherence-interventions_research.pdf
Vrijens B, De Geest S, Hughes DA, et al. A new taxonomy for describing and defining adherence to medications. Br J Clin Pharmacol. 2012;73(5):691-705. doi:10.1111/j.1365-2125.2012.04167.x
World Health Organization. Adherence to long-term therapies: Evidence for action. 2003. apps.who.int/iris/bitstream/handle/10665/42682/9241545992.pdf;jsessionid=B333A993575A3557E69BEDCA71F73BAD?sequence=1
Zhao Q, Chen C, Zhang J, Ye Y, Fan X. Effects of self-management interventions on heart failure: Systematic review and meta-analysis of randomized controlled trials. Int J Nurs Stud. 2021;110:103909. doi:10.1016/j.ijnurstu.2021.103909

















3 Comments. Leave new
This article is informative and helpful to my practice.
Thank you for your feedback!
This article is very informative I will recommend to my colleagues.