
Perfecting protocols to support patients with COVID-19
Research on the benefits of prone positioning for acute respiratory distress syndrome—and now COVID-19—has increased an awareness and urgency to initiate prone positioning earlier in the course of treatment and for longer durations. The Intensive Care Society suggests that proning may benefit patients by improving oxygenation and possibly delaying the need for mechanical ventilation before ICU admission. Mt Sinai Hospital in New York City examined its current protocol for prone positioning and optimized its practice to create efficiencies during the COVID-19 crisis and while in disaster mode.
Patient safety remains the top priority, but care team safety must be balanced in the equation. So, is prone positioning safe for both? Let’s consider the evidence and outcomes as nurses seek to adopt protocols and solutions to support the practice.
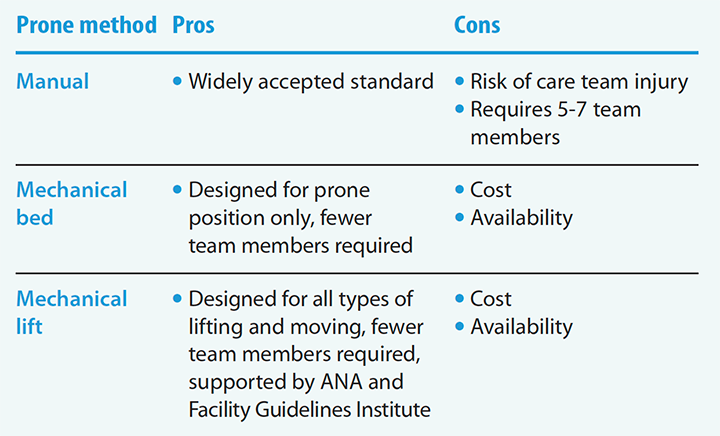
Currently, three methods are recognized and used to facilitate prone positioning.
Manual prone positioning is the most widely known practice and involves several team members moving the patient from supine to prone. The American Nurses Association and the Occupational Safety and Health Administration recognize that manual lifting is associated with musculoskeletal injuries, so caution must be taken to protect the care team when using this method.
The mechanical prone bed is designed specifically to rotate the patient from supine to prone. This technology requires fewer care team members but these specialized beds can be cost prohibitive and difficult to obtain, especially during episodes of high ICU census, such as we faced in 2020.
Mechanical lifts, either ceiling or mobile lifts, have been introduced successfully at several facilities to reduce the physical load and prevent care team injury. Using a lift also can decrease the number of care team members required to perform the task and thereby reduce their risk of exposure to COVID-19. The team’s confidence level in using the lift equipment can only be improved with practice and protocols that support using technology to aid in positioning.
Prone positioning
As with all practice changes, we must first recognize the problem exists and know that change is required. Next, we must understand that the need is urgent, especially to respond to the rise in COVID-19 admissions to our ICUs and the importance of introducing the prone position early in the treatment plan. Finally, we must overcome common barriers that prevent innovation and improvements that impact patient and care team safety. If anyone can make this change happen, it’s our nurses and frontline workers who possess the knowledge and skill to transform research into practice.
Access references and prone positioning method pros and cons at myamericannurse.com/?p=73771.
Dee Kumpar, MBA, BSN, RN, is vice president of clinical marketing at HD Nursing based in Benton, Arkansas, and a member of ANA-Michigan.
References
American Nurses Association. Safe Patient Handling and Mobility: Interprofessional National Standards Across the Care Continuum. Silver Spring, MD: American Nurses Association; 2013.
Intensive Care Society. ICS Guidance for Prone Positioning of the Conscious COVID Patient 2020. static1.squarespace.com/static/5e6613a1dc75b87df82b78e1/t/5e99e7f60755047b87934d6e/1587144697447/2020-04-12+Guidance+for+conscious+proning.pdf
The Joint Commission. Improving Patient and Worker Safety: Opportunities for Synergy, Collaboration and Innovation. 2012. jointcommission.org/-/media/tjc/documents/resources/patient-safety-topics/patient-safety/tjc-improvingpatientandworkersafety-monograph.pdf
Montanaro, J. Using in situ simulation to develop a prone positioning protocol for patients with ARDS. Crit Care Nurse. 2020;23(e1-13). doi:10.4037/ccn2020830
Wiggermann N, Zhou J, Kumpar D. Proning patients with COVID-19: A review of equipment and methods. Hum Factors. 2020;62(7):1069-76. doi:10.1177/0018720820950532
















