Jill Smith, a 58-year-old waitress in a local bar, comes to the clinic complaining of shortness of breath and a persistent cough for the last month. She reports she has lost 10 lbs recently, even though her eating habits (including a high meat intake and few green vegetables) haven’t changed.
Mrs. Smith states that she doesn’t smoke; she tried smoking one cigarette when she was 16. “That was enough for me,” she says. “I couldn’t stop coughing. I don’t get why people smoke. I was so glad my husband stopped smoking 6 months ago.”
Based on a complete history and physical examination, the practitioner orders a chest X-ray, which reveals a lung mass. Mrs. Smith subsequently is diagnosed with lung cancer. “I don’t understand it,” she says. “I’m not a smoker. How can this be?”
Like Mrs. Smith’s nurse, you might be surprised to encounter a patient who has lung cancer yet never smoked. Although lung cancer has long been considered a disease of smokers, rates have been rising in never-smokers. Worldwide, a surprising 25% of lung cancers occur in never-smokers, defined as people who’ve smoked fewer than 100 cigarettes in their lifetime.
According to the American Cancer Society, new cases of lung cancer in the United States during 2016 were estimated at 224,390; deaths from lung cancer numbered about 158,080, including about 56,000 deaths in never-smokers. Lung cancer in never-smokers (LCINS) is the seventh leading cause of cancer deaths in this country—enough to be considered a separate disease in itself. Epidemiologically, clinically, biologically, and psychosocially, LCINS differs from lung cancer in smokers.
The two main subgroups of lung cancer are non-small-cell lung cancer (NSCLC) and small-cell lung cancer (SCLC); the latter is rare in never-smokers. NSCLC has three primary histologic subtypes—squamous cell, adenocarcinoma, and large cell. Adenocarcinoma is the most common subtype in never-smokers.
Early-stage lung cancer carries a significantly lower mortality rate in never-smokers than in smokers. Unfortunately, most patients are diagnosed at an advanced stage; in never-smokers, the 5-year survival rate is a dismal 1%.
This article describes risk factors, assessment, and treatment of lung cancer in never-smokers; addresses the physical and psychosocial impact of the disease; and discusses the nurse’s role in promoting positive outcomes, including lung cancer screening and patient education.
Risk factors
In never-smokers like Mrs. Smith, NSCLC incidence has increased steadily since 1990. One U.S. study found a twofold increase in NSCLC from 2001 to 2013; a United Kingdom study found lung cancer rates in never-smokers rose from 13% to 28% over a 6-year period.
Reasons for the increase remain speculative. Some experts believe that thanks to relentless education campaigns on the harmful effects of smoking, fewer Americans are smoking today, reflected in the all-time lowest smoking rates since 1965. Although more lung cancers seem to be occurring in never-smokers, scientists aren’t sure if the LCINS rate is falsely elevated due to the sharp decline in smoking or if it’s truly higher than before. Some experts propose that exposure to environmental tobacco smoke (ETS), radon, air pollution, diet, and genetic factors may contribute to higher lung cancer rates in never-smokers.
Environmental exposures
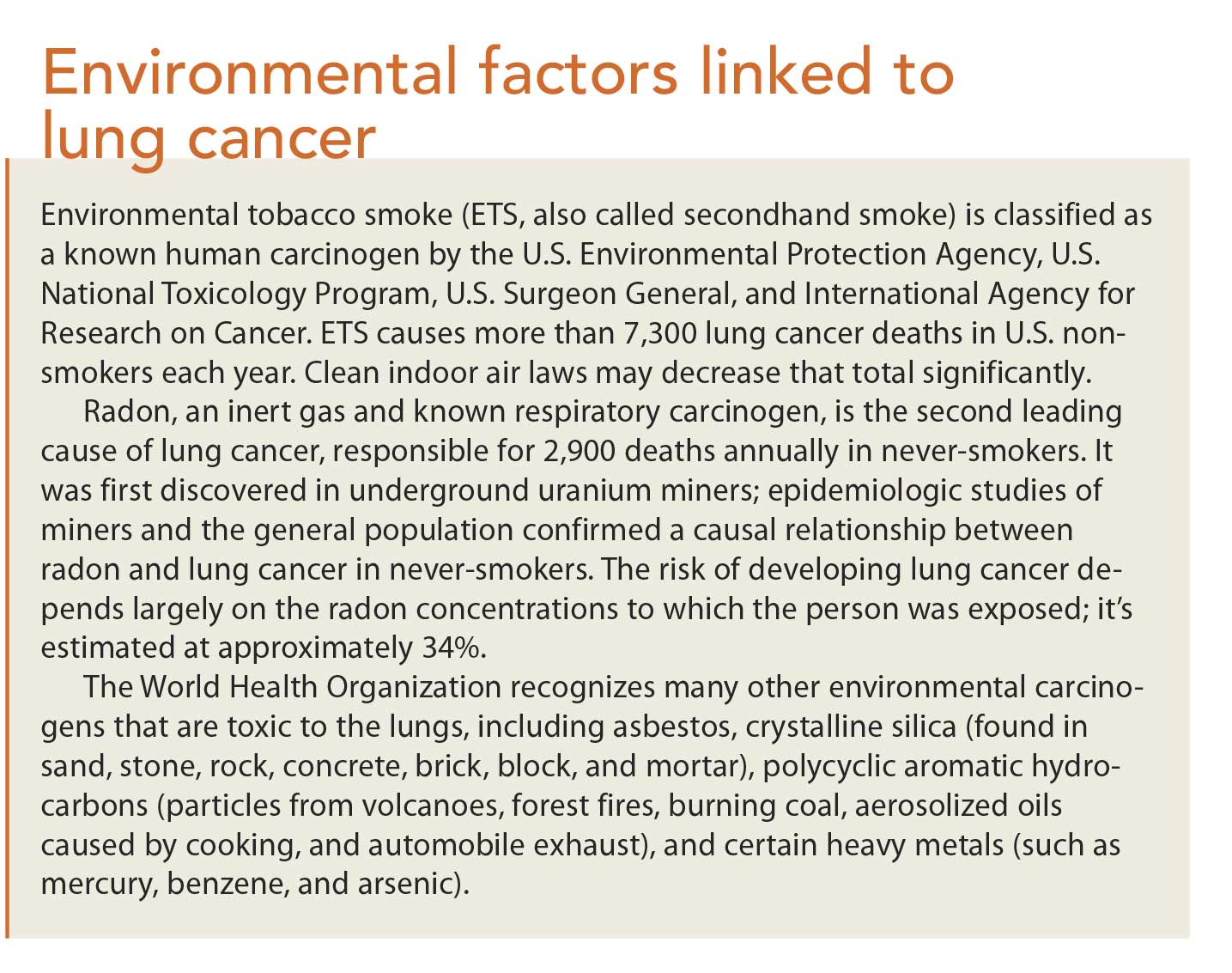
The link between ETS and lung cancer was established in 1981 when a large prospective study (n = 91,540) found that nonsmoking Japanese wives of heavy smokers had a higher risk of developing lung cancer than nonsmoking wives of nonsmoking men. Since then, dozens of studies have confirmed this connection. (See Environmental factors linked to lung cancer.)
Genetic alterations
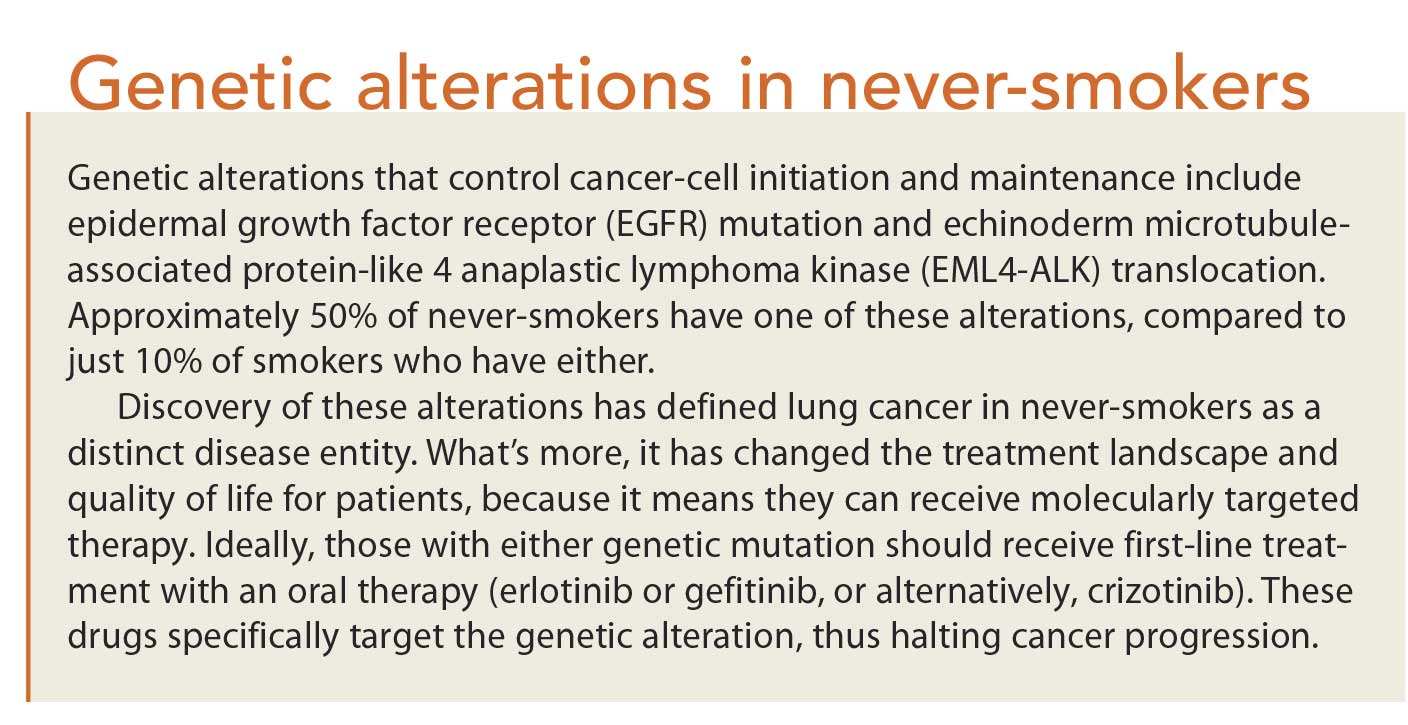
Certain genetic mutations are much more common in never-smokers with lung cancer than in smokers with lung cancer. (See Genetic alterations in never-smokers.)
Diet
A diet high in red meat, processed meats, high-fat foods, and butter significantly increases lung cancer risk in never-smokers. On the other hand, a diet high in vegetables, fruit, and fish has been shown to decrease lung cancer risk in never-smokers. Alcohol consumption and body mass index don’t affect risk.
Familial predisposition
Growing evidence indicates a family history of lung cancer increases a person’s lung cancer risk. A classic study by Tokuhta and Lilienfeld (1963) reported a 2.5-fold higher lung cancer risk in individuals who had a first-degree relative with a history of lung cancer. More recent epidemiologic studies confirm this risk level. Risk increases even more in people whose relatives were diagnosed with lung cancer before age 40 or who had multiple family members with lung cancer.
Age
As with all cancers, lung cancer risk increases with age. In never-smokers, the average age at diagnosis is controversial. Some studies report lung cancer is more likely in persons older than 65; others report just the opposite. One reason for the opposing data is that just 2% to 3% of patients with lung cancer are younger than 40, so obtaining a cohort large enough to study is challenging.
Gender
Research repeatedly has shown that LCINS is more common in women than men. Although this may result from women’s greater susceptibility to risk factors, it also may reflect the fact that twice as many women as men are never-smokers. Due to this higher proportion of female never-smokers, evidence suggests hormones, specifically estrogen, may play a role in lung carcinogenesis by stimulating NSCLC cell proliferation. Two estrogen receptors, ERα and ERβ, are expressed in lung tissue. ERβ is more commonly expressed and correlated with improved survival; ERα is a poor prognostic indicator for lung cancer. Hormone replacement therapy and hormonal contraceptives remain controversial in reducing lung cancer risk.
Geographic factors
Asia has a higher proportion of never-smokers with lung cancer than the United States. Among Asian females with the disease, 80% are never-smokers, compared to 10% or 15% of Western women. This most likely reflects a higher prevalence of smoking in Asian countries than in Western countries.
Clinical presentation
The patient may present to the primary healthcare provider with complaints of a cough or another sign or symptom that suggests an infection. Clinicians should always consider lung cancer as a differential diagnosis, even in never-smokers.
In both smokers and never-smokers, lung cancer signs and symptoms vary with tumor location and disease extent. Some patients lack symptoms and are diagnosed incidentally from a routine chest X-ray. Unfortunately, most are diagnosed late and have signs and symptoms of advanced disease. These manifestations may stem from:
• the tumor itself, which may cause cough, shortness of breath, wheezing, hemoptysis, chest pain, weight loss, hoarseness, and fatigue
• metastasis, which can lead to blurred vision, headaches, and pain
• paraneoplastic syndrome, which may cause hypercalcemia, confusion, nausea, vomiting, constipation, excessive thirst or urination, fatigue, seizures, coma, and syndrome of inappropriate antidiuretic hormone secretion.
Because never-smokers lack a history of smoking, many are misdiagnosed and treated for upper respiratory infection or allergies. Prompt, accurate identification of signs and symptoms is crucial for promoting a timely diagnosis and improving both outcome and quality of life.
Treatment
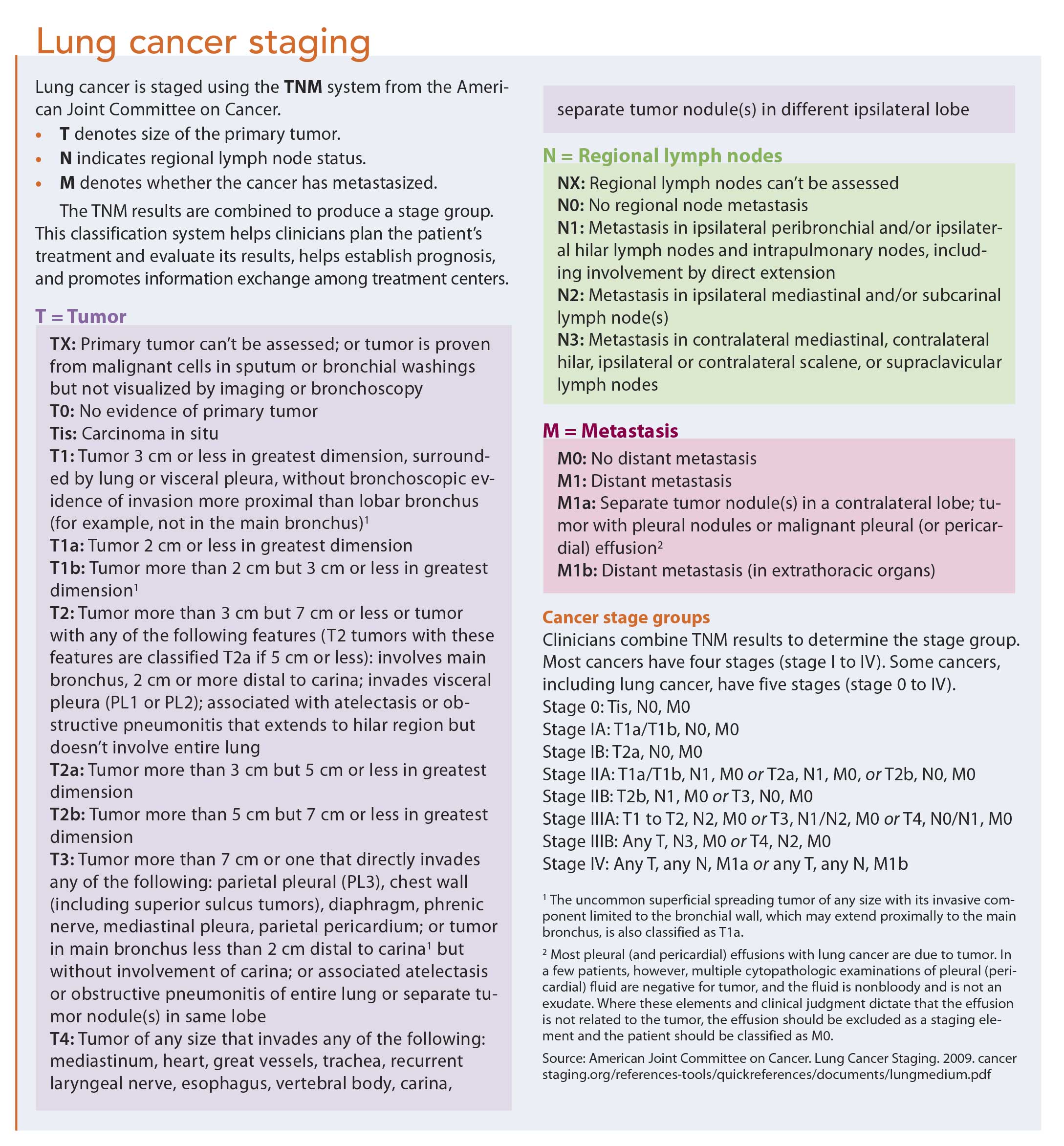
Treatment is based on cancer stage, which hinges on assessment of the tumor, whether it has metastasized, and the status of regional lymph nodes. (See Lung cancer staging.) Treatment of curable lung cancer (stages I, II, or III) may involve surgery, radiation, chemotherapy, or a combination. Incurable or metastatic lung cancer (stage IV) warrants chemotherapy, targeted therapy, or immunotherapy.
If a genetic mutation goes undetected but the tumor expresses more than 50% of the programmed cell death ligand 1 (PD-L1) receptor, the patient should receive the immunotherapy agent pembrolizumab as first-line treatment. Patients with neither genetic mutations nor PDL-1 expression typically receive standard treatment with I.V. chemotherapy, consisting of cisplatin or carboplatin in combination with pemetrexed or a taxane (paclitaxel or docetaxel) and, in some cases, bevacizumab (an angiogenesis inhibitor). Bevacizumab is contraindicated in patients with a history of a thromboembolic event, hemoptysis, or untreated brain metastases.
Physical and psychosocial impact of lung cancer
Patients with lung cancer, especially metastatic lung cancer, have a high symptom burden and high levels of distress due to signs and symptoms, treatment, and financial, spiritual, emotional, and psychosocial effects. Distress that goes undetected can reduce quality of life, decrease treatment adherence, lead to poorer clinical outcomes, and increase healthcare costs.
Most never-smokers are surprised by their diagnosis. Like smokers who have lung cancer, many neversmokers feel the social stigma asso ciated with this disease. The general perception that lung cancer is preventable and therefore self-inflicted makes never-smokers feel they’re being blamed for their illness. In a study of nearly 1,800 people in a 10-minute online test, 74% said they were biased against people with lung cancer. Lung cancer stigma can lead to anxiety, depression, and isolation, which affects the patient’s health and quality of life.
Nurses’ role
Nurses can play a key role in improving patient outcomes by screening and identifying patients— not just those at high risk for lung cancer but also those with few or no risk factors. Recognizing signs and symptoms regardless of smoking status and expediting the initial workup through appropriate diagnostic tests and referrals help ensure a prompt diagnosis and may improve prognosis.
When assessing a patient for possible lung cancer, be sure to take a thorough medical history, family history, environmental exposure history, and social history. These may reveal risk factors that clinicians might otherwise overlook. The National Comprehensive Cancer Network (NCCN) and the U.S. Preventive Services Task Force (USPSTF) have developed evidence-based screening guidelines. USPSTF recommends annual lung cancer screening with low-dose computed tomography in adults ages 55 to 80 who have a 30 pack-year smoking history and currently smoke or have stopped smoking within the past 15 years; NCCN recommends such screening for people ages 55 to 74. However, screening guidelines for never-smokers don’t exist.
Patient education
Educate patients about lung cancer risk factors besides smoking. Like Mrs. Smith, never-smokers who are diagnosed with lung cancer may ask, “Why me?” or “How did this happen?” Teaching them that lung cancer isn’t just a disease of smokers and exploring their medical and exposure histories in detail can offer insight into why and how they got lung cancer. As needed, initiate referrals for counseling to help mitigate the anger, guilt, and stigma they may be experiencing.
Early diagnosis is key
LCINS is a rapidly growing disease that’s not fully understood. Unless detected early, it carries a poor prognosis. Screening methods for LCINS haven’t been identified, so healthcare providers must be vigilant and recognize that people with no smoking history are still at risk for lung cancer. Research aimed at understanding this growing at-risk population needs to be a top priority.
Mrs. Smith is diagnosed with stage IIB cancer. She undergoes surgery followed by radiation treatment. Six months later, she is able to return to her job and her usual activities.
Victoria Sherry is an oncology nurse practitioner at the Abramson Cancer Center of the Hospital of the University of Pennsylvania in Philadelphia. (Note: Names in the clinical scenario are fictitious.)
Selected references
American Cancer Society. Cancer Facts and Figures 2016.
American Joint Committee on Cancer. Lung Cancer Staging. 2009.
Cataldo JK, Jahan TM, Pongquan VL. Lung cancer stigma, depression, and quality of life among ever and never smokers. Eur J Oncol Nurs. 2012;16(3):264-9.
Centers for Disease Control and Prevention. 2014 Surgeon General’s Report: The Health Consequences of Smoking—50 Years of Progress.
Centers for Disease Control and Prevention. National Center for Health Statistics. Adult Tobacco Use Information. Glossary. Last reviewed November 6, 2015.
Centers for Disease Control and Prevention; Office on Smoking and Health. How Tobacco Smoke Causes Disease: The Biology and Behavioral Basis for Smoking-Attributable Disease: A Report of the Surgeon General. 2010.
Couraud S, Zalcman G, Milleron B, Morin F, Soquet PJ. Lung cancer in never smokers—a review. Eur J Cancer. 2012;48 (9):1299-311.
Cufari ME, Proli C, Phull M, et al. Increasing incidence of non-smoking lung cancer: presentation of patients with early disease to a tertiary institution in the UK. Lung Cancer. 2016;91(suppl 1):S17-S18.
Garcia-Lavandeira JA, Ruano-Ravina A, Barros-Dios JM. Alcohol consumption and lung cancer risk in never smokers. Gac Sanit. 2016;30(4):311-7.
Gaughan EM, Cryer SK, Yeap BY, Jackman DM, Costa DB. Family history of lung cancer in never smokers with non-small-cell lung cancer and its association with tumors harboring EGFR mutations. Lung Cancer. 2013; 79(3):193-7.
Hamaan HA, Ostroff JS, Marks EG, Gerber DE, Schiller JH, Lee SJ. Stigma among patients with lung cancer: a patient-reported measurement model. Psychooncology. 2014; 23(1):81-92.
McCarthy WJ, Meza R, Jeon J, Moolgavkar SH. Lung cancer in never smokers: epidemiology and risk prediction models. Risk Anal. 2012;32(suppl 1):S69-84.
Melloni BB. Lung cancer in never-smokers: radon exposure and environmental tobacco smoke. Eur Respir J. 2014;44(4):850-2. National Comprehensive Cancer Network.
Recent updates to NCCN clinical practice guidelines in oncology. Non-small cell lung cancer, version 3.2017.
Pallis AG, Syrigos KN. Lung cancer in never smokers: disease characteristics and risk factors. Crit Rev Oncol Hematol. 2013;88(3):494-503.
Planchard D, Besse B. Lung cancer in neversmokers. Eur Respir J. 2015;45(5):1214-7.
Santoro IL, Ramos RP, Franceschini J, Jamnik S, Fernandes AL. Non-small cell lung cancer in never smokers: a clinical entity to be identified. Clinics (Sao Paulo). 2011;66(11): 1873-7.
Sethi TK, El-Ghamry MN, Kloecker GH. Radon and lung cancer. Clin Adv Hematol Oncol. 2012;10(3):157-64.
Sriram N, Mills J, Lang E, et al. Attitudes and stereotypes in lung cancer versus breast cancer. PLoS One. 2015;10(12):e0145715.
Subramanian J, Govindan R. Molecular profile of lung cancer in never smokers. EJC Suppl. 2013;11(2):248-53.
Tokuhata GK, Lilienfeld AM. Familial aggregation of lung cancer in humans. J Natl Cancer Inst. 1963;30:289-312.
U.S. Department of Health and Human Services. National Toxicology Program. 14th Report on Carcinogens 2016.
U.S. Environmental Protection Agency. Health risk of radon. Updated September 22, 2016.
U.S. Environmental Protection Agency. Respiratory Health Effects of Passive Smoking: Lung Cancer and Other Disorders. December 1992.
U.S. Preventive Services Task Force. Lung cancer: Screening. December 2013. Updated July 2015.
World Health Organization. Exposure to Benzene: A Major Public Health Concern. 2010. World Health Organization; International
Agency for Research on Cancer. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans. Tobacco Smoke and Involuntary Smoking. Vol. 83; 2004.

















{kind=link}
{kind=link}
{kind=link}
1 Comment.
I never knew that lung cancer is the seventh leading cause of cancer deaths in America! My brother-in-law was recently diagnosed with lung cancer. Hopefully he can find a great oncologist and treatment!