
Learn more about this condition and advances aimed at relief.
- Atopic dermatitis (AD) is the most prevalent type of eczema (chronic inflammatory skin conditions).
- Nurses have the knowledge to educate and support patients and families and eliminate exacerbations.
- Dupilumab, the first biologic drug approved to treat AD, blocks a key source of inflammation inside the body that can cause AD.
- Explain the pathophysiology and risk factors for atopic dermatitis (AD).
- Identify physical and psychosocial symptoms of AD.
- Describe education considerations for patients with AD.
No relevant financial relationships were identified for any individuals with the ability to control content of the activity.
Expiration: 12/1/27
Alexander*, a healthy 4-month-old baby boy of Eurasian descent, is exclusively breastfed. This morning, his mother, Margaret, changes him and finds crusty, red oozing blisters covering his back. She calls the healthcare provider to schedule a visit. The provider diagnoses atopic dermatitis (AD) and prescribes oral and topical corticosteroids. Ramon, the clinic nurse, offers support to the family, provides education about the condition, and shares a handout they can take home to read.
AD defined
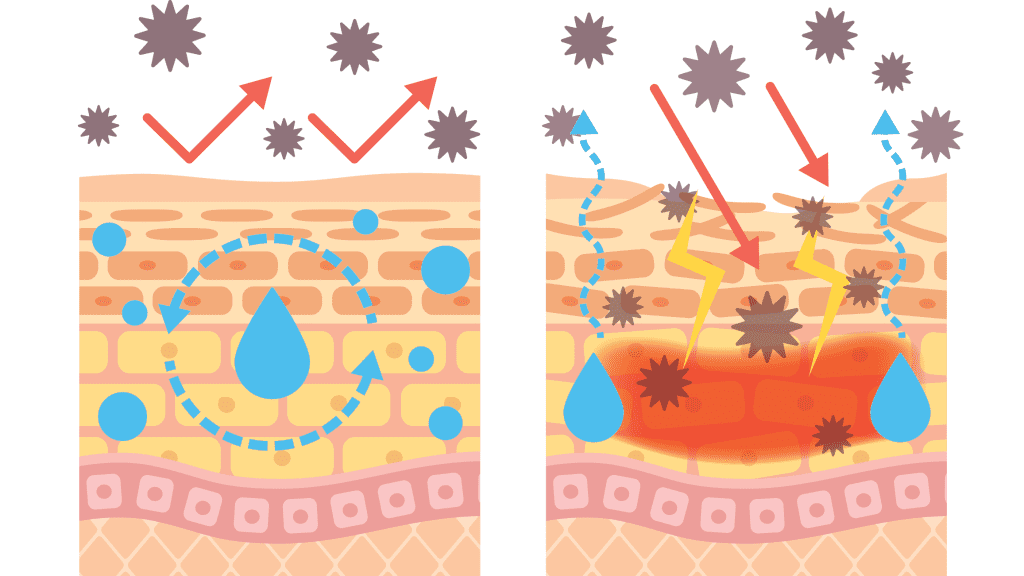
AD is the most prevalent type of eczema, which encompasses a group of chronic inflammatory skin conditions that result in irritation, rash, itching, and skin-barrier issues. Eczema (often used interchangeably with AD) features chronic pruritis (itchy skin) that activates the immune system with bouts of exacerbation and remission.
AD, an immunoglobulin E (IgE)-mediated condition, frequently occurs alongside other IgE conditions such as allergic rhinitis and asthma in individuals and familial lines. Most patients with AD exhibit notably elevated levels of serum IgE as well as peripheral eosinophilia (higher-than-normal levels of eosinophils, which are a type of white blood cell involved in the body’s defense against disease).
Who’s at risk?
AD affects both children and adults (15% to 30% of children and 2% to 10% of adults in developed countries). Those of Asian, African, and Latin descent experience a higher prevalence of AD. Exacerbations and remissions are common through 20 years of age. Those at highest risk for developing AD have a genetic predisposition based on a family history of IgE-mediated disorders. The strongest genetic risk factors are found in European and Asian patients.
Physical symptoms
AD symptoms vary in severity and duration. Pruritis, the most common symptom, involves itchy and hyperirritable skin due to increased histamine. This may manifest as dry, scaly skin that appears rough, red, or inflamed due to lipid content, sebaceous gland activity, and sweating. Intense itching leads to scratching and further aggravation of the condition. For this reason, eczema conditions frequently are called the itch that rashes, rather than the rash that itches.
The National Eczema Association reports that 85% of people with AD experience itching every day. Rashes can appear as patches of red, raised bumps or small fluid-filled blisters that weep, ooze, crust over, and bleed. Lesions can result from the trauma of scratching and may appear in areas of increased sweating and hypervascularity. When rubbed, the skin will appear red and then turn pale.
Over time, the chronic scratching and rubbing may discolor and thicken the skin; it may appear leathery. Constant scratching can break the skin, making it more susceptible to bacterial, viral, or fungal infections. The weakened skin barrier also may allow irritants and allergens to penetrate the skin more easily.
Psychosocial symptoms
Many patients also experience psychosocial symptoms. Some report disturbed sleep related to itching as well as behavioral changes due to the uncomfortable symptoms. This can lead to decreased concentration and energy levels. The skin’s appearance can affect the patient’s self-esteem and willingness to interact with others. The possibility of long-term scarring exists. AD isn’t contagious, although skin appearance may suggest otherwise, which can cause others to react negatively.
The patient and their support system must exercise vigilance to avoid triggers and irritants that may prompt an exacerbation and manage symptoms. This effort can prove psychologically exhausting. However, many valuable resources exist for patients and caregivers. In addition, nurses play an important role in promoting trust, therapeutic relationships, setting realistic treatment expectations, and engaging patients in self-management. (See Patient resources.)
Patient resources
Share these resources with patients to engage them in treatment and self-management.
- American Academy of Dermatology Association (aad.org/) supplies an overview of many skin diseases and conditions, including cosmetic treatments and relevant care for individuals with darker skin tones.
- American College of Allergy, Asthma & Immunology (acaai.org/resource/should-i-treat-my-allergies-with-immunotherapy/) offers patients an online tool to gather information about treating their allergy and asthma symptoms with immunotherapy. Patients rank their responses and can print the document to share with their provider as part of treatment planning.
- National Eczema Association (nationaleczema.org/) offers an overview of the different types of eczema and provides management resources, including a list of products that receive the association’s seal of acceptance. This seal indicates the product is free from ingredients that may cause irritation in patients with eczema and sensitive skin.
Pharmacologic treatment
AD treatment, individualized to each patient, aims to manage daily symptoms and flare-ups by avoiding contact with offending agents, eliminating inflammatory disorders and infections, preserving and restoring the skin, and managing itching. Prescription and over-the-counter (OTC) medications can help alleviate symptoms. Most OTC medications work to manage the itch, rash, irritation, and nighttime waking. (See Treatment options.)
Treatment options
Several treatment options exist to manage atopic dermatitis symptoms and exacerbations.
Topical
- Corticosteroids
- Hydrocortisone
- Janus kinase (JAK) inhibitors
- Prescription steroids
- Shampoos
- Topical calcineurin inhibitors
Oral
- Antibiotics
- Antihistamines
- Antipruritics
- Immunosuppressants
- JAK inhibitors
- Pain relievers, nonsteroidal anti-inflammatory drugs
- Prescription corticosteroids
Injectable
- Biologics (monoclonal antibodies)
Holistic
- Avoid long hot-water bathing.
- Seek counseling and support.
- Humidify dry heat.
- Take medicated baths.
- Perform proper nail care.
- Seek phototherapy.
- Wear cotton fabrics.
- Apply wet wrap therapy.
The recommended medications provide Alexander with temporary relief. However, as the oral corticosteroids are weaned, symptoms persist and begin to spread to his neck folds, antecubital area, ankles, feet, and behind the knees. Although only 6 months old now, Alexander rubs his body on the sheets and other surfaces in an attempt to scratch. Margaret continues breastfeeding, and she limits her diet to prevent flare-ups. Alexander doesn’t sleep through the night, his crib sheets are blood stained, and he’s often cranky throughout the day. Margaret applies topical ointments and administers oral medications as this itch–rash cycle continues. At a follow-up visit to the provider, Ramon discusses the importance of adhering to treatment recommendations and provides resources for online support groups.
Topical treatments
OTC and prescription topical AD treatments come in various forms, including lotions, creams, ointments, gels, sprays, and shampoos. Application varies from once a day to up to four times a day for several days. The most commonly prescribed are topical steroids. Steroids vary in strength with ranges in class from least potent (Class 7) to most potent (Class 1). Steroids may cause side effects (such as skin reactions, irritations, and thinning) and should be stopped when advised by a provider. Patients and caregivers can apply moisturizers on top of steroids if they wait 10 to 20 minutes between applications. Steroids should be applied to affected areas of the skin, whereas moisturizers can be applied to broader areas of the body.
Newer topical medications stop pathways in the immune response that trigger AD symptoms. Topical Janus kinase (JAK) inhibitors block enzymes in cytokine pathways that contribute to inflammation and itch. Topical calcineurin inhibitors and nonsteroidal medications also block pathways of certain cells in the immune system that activate AD symptoms. Phosphodiesterase-4 inhibitors also act in this way to block triggering and resultant inflammation.
Oral medications
Common systemic oral medications include antihistamines, non-steroidal anti-inflammatory drugs, antipruritic agents, corticosteroids, antibiotics, and immunosuppressants.
A provider may order immunosuppressants for patients with moderate-to-severe AD. JAK inhibitors, such as high-dose abrocitinib and low-dose upadacitinib, also can be given orally, but they have increased adverse effects compared with other treatments (such as dupilumab). If providers prescribe immunosuppressants or systemic medications, they usually do so for a short period and then taper the dose.
Providers also may prescribe oral corticosteroids or immunosuppressants for severe cases. Although effective, these medications have a rebound effect when stopped, which can make the return of AD symptoms worse. Long-term use of corticosteroids carries many serious side effects, including increased blood glucose, muscle wasting, thin skin, peptic ulcers, and osteoporosis.
Injectable medications
Targeted biologic medications block interleukin, a protein chemical messenger that can overact and cause an immune response in individuals with AD. Included in this class of biologics are monoclonal antibodies (mAbs). Therapeutic mAbs are now available to treat an increasing number of conditions. They modulate immunity, kill cells, and neutralize infectious organisms. Dupilumab, the first biologic drug approved for AD, blocks IL-4 and IL-3 signaling, a key source of inflammation within the body. The drug was first approved and made available for adult patients in 2017. In July 2022, the results of ongoing clinical trials led the FDA to approve the treatment for patients as young as 6 months.
Over 25 new biologics to treat AD are in development and various stages of clinical trials. To date, only dupilumab has been approved for pediatric and adult use. The FDA has approved dupilumab to treat moderate-to-severe AD in adult and pediatric patients age 6 months and older whose disease isn’t adequately controlled with topical prescription therapies or when those therapies aren’t advisable.
Dupilumab is available only as a subcutaneous injection in pre-filled pens or syringes depending on the dose, which is based on the patient’s age and weight. It’s administered every 2 or 4 weeks. The manufacturer’s list price is $3,587.92 per carton (two syringes per carton). Commercial health plans and copay cards offer assistance with out-of-pocket costs and coordination with specialty pharmacies. According to the manufacturer, few patients pay the list price. The medication doesn’t require initial or ongoing lab testing or monitoring. Patients who receive dupilumab should discuss receiving live vaccines with their provider. It’s unknown whether concurrent administration while receiving dupilumab will impact vaccine safety or effectiveness.
Now 2 years old, Alexander has developed food allergies. His AD remains chronic, and he has frequent flare-ups. Oral and topical medications continue. He and his mother have visited several allergists and dermatologists, who classify Alexander’s AD as severe. Ramon collects subjective and objective assessments and has developed a rapport with the family. He frequently speaks with them and provides symptom management and care planning. He recommends some holistic approaches, such as wearing cotton fabrics and humidifying the home’s air, to alleviate symptoms.
Nursing implications
Patients and families may feel overwhelmed when confronted with an AD diagnosis. Using their advocacy skills, nurses provide quality patient-centered care and guidance to ensure patient and family understanding of the condition and treatment recommendations. In addition, nurses’ clinical skills help to eliminate exacerbations and their associated complications. Essential nursing tasks include assessments and knowledge of a range of interventions.
Nursing assessment
Nurses may encounter patients with AD in all care settings; however, most are managed in the primary care/community setting. Skin assessment, the focus for patients with AD, includes noting various characteristics, such as color, moisture, texture, and temperature. Document any skin alterations, including erythema, edema, tenderness, erosions, excoriations, and thickening. Rashes may appear in varying colors—purple, brown, or grayish—in individuals with darker skin tones. On lighter skin tones, rashes may appear red. Early recognition of signs of infection will facilitate prompt treatment and help prevent complications. Your assessment also should include recognizing emotional and psychological stressors.
Nursing interventions
Dermatology nurse specialists play an important role in many aspects of care for patients with AD. They engage patients through education, guide self-management, and offer psychosocial support. Comprehensive management requires disease monitoring, interprofessional care, nurse consultations, and referrals to appropriate specialists as needed.
Nursing care of patients with AD involves clinical and interpersonal skills. Your empathy and active engagement will help build trust, keep patients motivated and informed, inspire confidence, and encourage personal responsibility. You’ll also be called on to provide reassurance and hope during AD exacerbations. To promote patient and family well-being, offer support and share resources to help manage psychosocial issues, foster self-esteem, reduce anxiety, mend relationships, address financial concerns related to treatment costs, and establish realistic expectations.
During active care of the patient with AD, your prompt nursing interventions can help prevent complications such as further itch/rash cycles and infection. Explaining this cycle to patients and family members by describing the link between the skin and the immune system will help them understand treatment and other interventions. Armed with this information, the patient can make autonomous care decisions.
Nursing interventions also include relieving symptoms and preventing further deterioration via holistic and pharmacologic treatment. Nurses in all settings assist with topical treatments such as applying moisturizers, which help provide a skin barrier and keep the skin hydrated to reduce dryness and itching. Wet wrap therapy, aimed at enhancing product absorption and soothing the skin, involves applying medication and moisturizer to wet skin and then covering it with wet cloth or bandages. For small children who can’t control itching, especially during sleep, apply gloves or socks to their hands.
Alexander is now 4 years old. Despite ongoing medications and treatment regimens, his condition remains severe with regular flare-ups. He develops normally but has interrupted sleep, itches in his sleep, and is generally uncomfortable most days. The provider mentions a newer treatment option with monoclonal antibodies (dupilumab) recently approved for younger patients. The provider believes Alexander’s severe diagnosis makes him a good candidate.
Dupilumab is an age- and weight-based subcutaneous injection administered once a month. Margaret, desperate for relief for her child, hopes this new medication will provide some symptom relief and help improve her son’s quality of life. Ramon teaches Margaret and other family members how to administer the subcutaneous injection at home. A nurse case manager helps Margaret apply for a medical co-pay card and a specialty pharmacy contacts her to arrange for medication delivery and payment. Through health insurance, the co-pay cards, and the specialty pharmacy, Margaret pays $70 for a two-syringe box. (See Subcutaneous injection technique.)
Subcutaneous injection technique
Use the following technique (and teach it to patients and caregivers) to administer dupilumab.
- Dupilumab comes in pre-filled pens or syringes with an attached shielded or covered injection needle.
- Keep the medication refrigerated and protected from direct sunlight and heat. Before administration, leave the medication at room temperature without removing the needle cap for 30 to 45 minutes depending on the dosage and preparation type. Don’t shake the medication.
- Take universal precaution steps for administering medication, including proper handwashing, personal protective equipment, identifying the patient, and medication safety. In patients between ages 6 months to 12 years, a trained caregiver should administer the medication.
- Inject the medication in the thigh, abdomen (2 inches or more away from the navel), or outer upper arm.
- Assess the selected site; avoid areas with tenderness, inflammation, bruising, scarring, or any other skin abnormalities.
- Clean the injection site with alcohol.
- Pinch a fold of skin and insert the needle at a 45-degree angle. Relax the pinch and push the plunger rod down slowly and steadily as far as it will go until the syringe is empty.
- When releasing the plunger rod, the shield will cover the needle. Don’t attempt to recap the needle. Don’t rub the skin after the injection.
- Rotate injection sites regularly.
- Don’t perform the injection if the medication appears cloudy or contains visible particulate matter.
- After administration, follow sharps disposal recommendations.
Patient education
In addition to providing valuable information related to AD management, you also can facilitate patients’ and family members’ decision-making, specifically with regard to treatment options, and develop problem-solving skills to navigate care strategies. Use your understanding of potential exacerbation triggers to teach patients and family members about these triggers and how to incorporate preventive measures and treatments into their daily lives. For example, explain that keeping nails short and clean with no sharp edges can help prevent cuts to skin in the event of scratching. Advise them to look for products with the National Eczema Association seal of acceptance and to avoid rough fabrics, perfumes, dyes, and harsh chemicals. In addition, recommend that they run air conditioning during allergen seasons and to avoid excessive sweating.
If the patient’s AD is associated with allergic reactions, they should consider wearing an alert tag. If ordered because of severe allergic reactions, provide education regarding administration of epinephrine using an autoinjector pen.
Successful patient and family education requires understanding the role of health literacy, including the patient’s or family member’s cognitive level, how they process and interpret information, and their motivation for behavior change. In addition, support and counseling can enhance coping skills and management of psychosocial concerns.
Best practices for an engaged learning process include listening to the parent and child about their AD journey. This will help you identify their knowledge of the condition, current disease-management skills, learning needs, and readiness to learn. By establishing this therapeutic relationship, you can advance the nurse–patient relationship to connection, understanding, and goal setting. Create small goals to help break down information into less-overwhelming, more successfully attainable parts. Your expertise reinforces learning so patients and family members can apply their knowledge and skills, build confidence, and feel motivated to manage the complicated cycles of AD.
Life-altering condition
Soon after beginning injection treatment with dupilumab, Alexander’s skin dramatically improves. The irritated areas begin to resolve, and his skin appears clearer. He sleeps through the night, and the sheets are clean in the morning. His quality of life also improves. As needed, holistic and topical treatments continue to address mild symptoms that flare in response to unavoidable seasonal triggers. Alexander frequently comments on the relief he experiences since beginning treatment.
Depending on severity, AD can prove life-altering. Patients and their support systems need an all-encompassing healthcare team, which includes nurses playing a vital role in helping patients manage their disease. Nursing care and comfort will prove invaluable to these patients and their families.
*Names are fictitious.
Stephanie M. Chung is an associate professor of nursing at Georgian Court University in Lakewood, New Jersey.
American Nurse Journal. 2024; 19(12). Doi: 10.51256/ANJ122414
References
American Academy of Dermatology Association. Eczema resource center. aad.org/public/diseases/eczema
Chiricozzi A, Maurelli M, Calabrese L, Peris K, Girolomoni G. Overview of atopic dermatitis in different ethnic groups. J Clin Med. 2023;12(7):2701. doi:10.3390/jcm12072701
Chu AWL, Wong MW, Rayner DG, et al. Systemic treatments for atopic dermatitis (eczema): Systematic review and network meta-analysis of randomized trials. J Allergy Clin Immunol. 2023;152(6):1470-92. doi:10.1016/j.jaci.2023.08.029
Grossman J. Steroid cream or moisturizer: Which should I apply first? My Eczema Team. September 12, 2023. bit.ly/3zT9loq
Hinkle J, Cheever KH, Overbaugh K. Assessment and management of patients with allergic disorders. In: Brunner & Suddarth’s Textbook of Medical-Surgical Nursing. 15th ed. Waltham, MA: Wolters Kluwer Health, Inc.; 2021.
National Eczema Association. Atopic dermatitis. nationaleczema.org/eczema/types-of-eczema/atopic-dermatitis
National Eczema Association. Biologics are changing the landscape of eczema treatment. March 15, 2022. nationaleczema.org/blog/biologics-eczema-treatment
National Eczema Association. Eczema treatments. National eczema.org/eczema/treatment
Sanofi and Regeneron Pharmaceuticals. Dupixent: MOA: Mechanism of action. dupixenthcp.com/atopicdermatitis/about/mechanism-of-action
Sanofi and Regeneron Pharmaceuticals. Dupixent: Pricing and insurance. dupixent.com/support-savings/cost-insurance
Sanofi and Regeneron Pharmaceuticals. Instructions for use: Dupixent injection. July 2023. regeneron.com/downloads/dupixent_ifu.pdf
Thompson D. Best practice guidelines: Integrating person and family centred care and client centred learning into practice in a nurse-led eczema clinic. Aust Nurs Midwifery J.2019;26(8):30-3.
van Os-Medendorp H, Deprez E, Maes N, et al. The role of the nurse in the care and management of patients with atopic dermatitis. BMC Nurs. 2020;19(1):102. doi:10.1186/s12912-020-00494-y
Key words: Atopic dermatitis, dermatology nursing, monoclonal antibodies















1 Comment. Leave new
Thank you for this education on Atopic Dermatitis. I appreciate all evidence based clinical information that is in an organized format to up-date my knowledge and add to the practice in caring for my patients. This was great!