

A comprehensive ambulatory cancer center’s journey to implementing tiered huddles
- Tiered huddles are brief conversations that occur throughout levels of an organization or across health systems to improve patient safety, communication, situational awareness, care coordination, resource utilization, patient outcomes, and service.
- Using an inclusive approach, this organization constructed a meaningful process with measurable operational and patient-centered metrics.
Tiered huddles, brief conversations that occur throughout levels of an organization or across health systems, move up and back down the organizational structure to improve patient safety, communication, situational awareness, care coordination, resource utilization, patient outcomes, and service. The implementation and outcomes associated with tiered huddles align with organizational goals of patient safety; patient, employee, and provider satisfaction; and high reliability. Using an inclusive approach to designing and implementing tiered huddles at the Miami Cancer Institute (MCI), leaders and executives constructed a meaningful process with measurable operational and patient-centered metrics, which had a positive impact on cross-functional teams and departments.
Some background
MCI began evaluating the use of huddles during the COVID-19 pandemic after establishing routine executive and leadership calls to discuss and share operational and staffing information related to the pandemic’s impact. During these calls, leaders, clinical staff, and providers acquired accurate and timely information to stay informed, reduce anxiety, and effectively care for patients.
Interprofessional collaboration made easy
Using audit and feedback to improve compliance with evidence-based practices
In December 2021, as the last wave of the pandemic for the year started to decline, MCI executive leaders reached out to the executive leadership at Baptist Hospital of Miami (BHM) to learn about and observe their daily huddle process. BHM’s two-tiered process includes sophisticated reporting and tracking conducted between 0900 and 0945 daily. The MCI team observed each tier and met with BHM’s data analyst, who’s dedicated to managing and developing the daily huddle reports. The team also conducted literature reviews of published articles on huddle implementation in other healthcare institutions.
During an executive operations meeting and after the initial research and observations, as the assistant vice president of nursing lead for our huddle initiative, I provided a comprehensive overview of tiered huddles. The presentation covered the huddle definition as well as its purpose, design concepts, benefits, and value to the organization. I also introduced the BHM model, along with practical recommendations for successful implementation and relevant references for further consideration. The executive team agreed to move forward with designing and implementing tiered huddles at MCI.
The planning phase
MCI aimed to replicate, demonstrate, and achieve the published benefits of daily tiered huddles within the first year of implementation. The tiered huddle team (which included executive and operational leaders and staff) began designing tiered huddles in January 2022 and decided to make the launch an inclusive process. The aim was to add value to the work environment and not be seen as another task or become the flavor of the month and soon forgotten.
The team started by sharing searched articles with clinical, operational, and quality leaders. We then invited them to a series of meetings to discuss operationalizing tiered huddles and how to make them meaningful, efficient, and worth attending. In addition, we discussed the best times for the huddles, relevant topics, and who should report and conduct the huddles. To ensure efficiency, operational leaders requested that we start with two tiers at no more than 30 minutes each. Leadership agreed to keeping documentation requirements to a minimum and that all supervisors, managers, directors, and executives (clinical and nonclinical) should attend (but daily attendance wasn’t mandatory). They also decided that the leader presenting at the second tier, which included executives, need not be a director.
Over the next 2 months, we designed MCI’s tiered huddle structure, agenda, reports, and documentation template. We provided education at staff meetings, leadership forums, and operational leadership meetings. (See Tiered huddle design.)
Tiered huddle design
Miami Cancer Center’s tiered huddle structure includes a bi-directional communication flow.
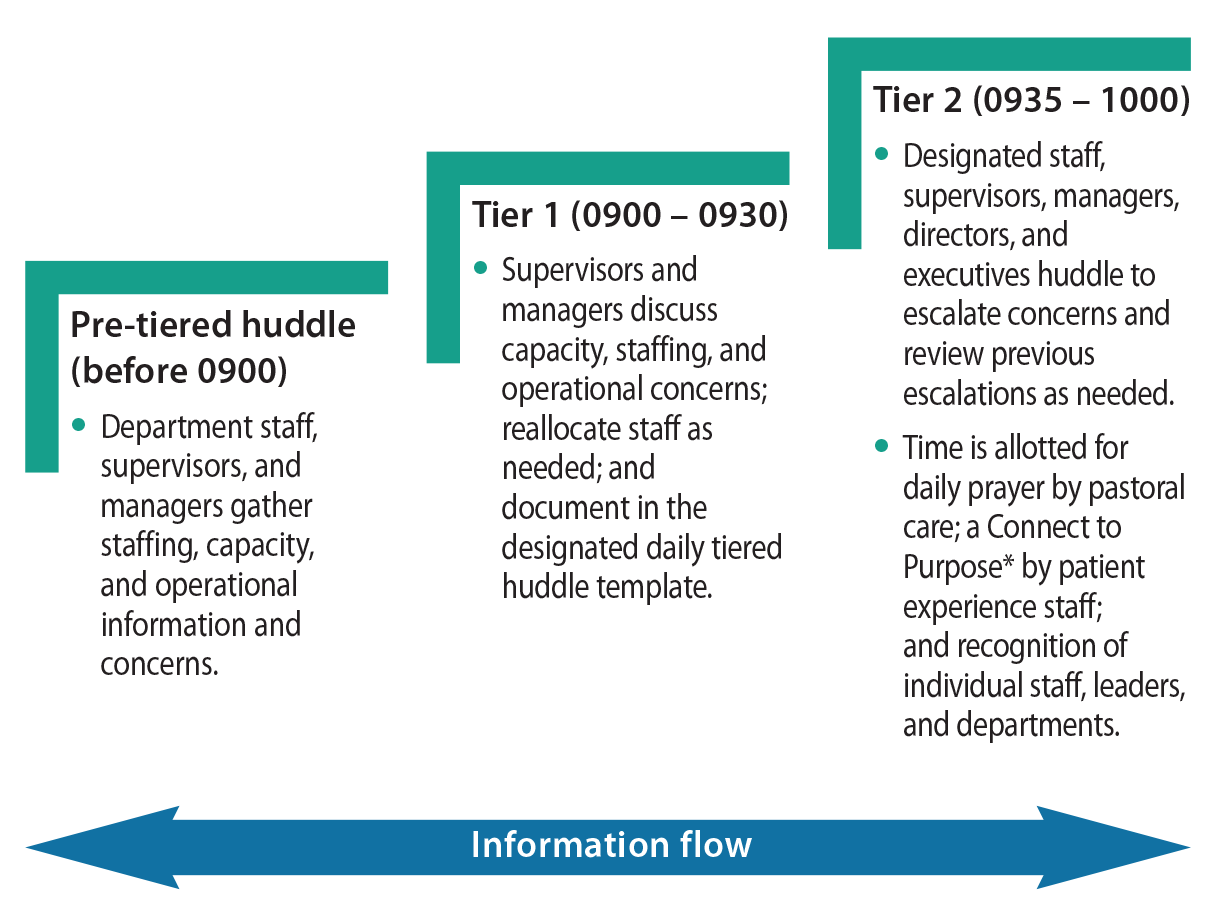
*Connect to Purpose is a pause in a routine meeting agenda to read a letter from a patient, family member, or staff that allows those in the meeting to reflect and connect to the mission and vision of the organization.
In keeping with leadership feedback regarding tiered huddle design, we created a simple Excel report template with drop-down fields to reduce documentation variation and simplify report generation and analysis. Each department leader or their staff designee completed one section, labeled with their name, department, and floor location. We placed the monthly report template and agenda in Microsoft Teams, to which all clinical and operational leaders, their staff designees, and executives had access.
At the time of implementation, we prioritized topics around areas affected by COVID-19 (volume, staffing, providers on shift, operational safety, quality or patient care concerns, and escalation resolution reviews). The long-term goal of the daily huddle report was to trend the information entered over time to streamline operations and improve patient care and service. Leaders or their designees documented their report before the second tiered huddle session. We used a standardized agenda template at every second tier huddle to structure the conversation, organize the reporting, and guide the huddle leader through the meeting.
Huddle launch
In April 2022, MCI launched daily tiered huddles. We sent a meeting invitation for second tier huddles to all applicable clinical and operational leaders, including executives. The invitation included a Zoom and in-person location. Typically, 15 to 25 people (leaders, staff, and executives) attended in-person. However, as COVID-19 numbers rose, we transitioned to Zoom only and remain on Zoom as of January 2024.
For the first week of implementation, we called the tiered huddles “Mock Daily Huddles” to reduce anxiety and stress about attending or reporting. An executive led the first two mock huddles and asked for director-level champions to preside over second tier huddles in preparation for the remainder of the first month. Six directors volunteered to serve as huddle leads. Administrative assistants took responsibility for obtaining a meeting room, ensuring functioning media equipment, displaying the huddle report and agenda, and documenting any additional notes and escalations not entered in the report. The administrative assistants also ensured that leaders entered their escalation resolutions promptly to close the issue and note the resolution date.
Results and adjustments
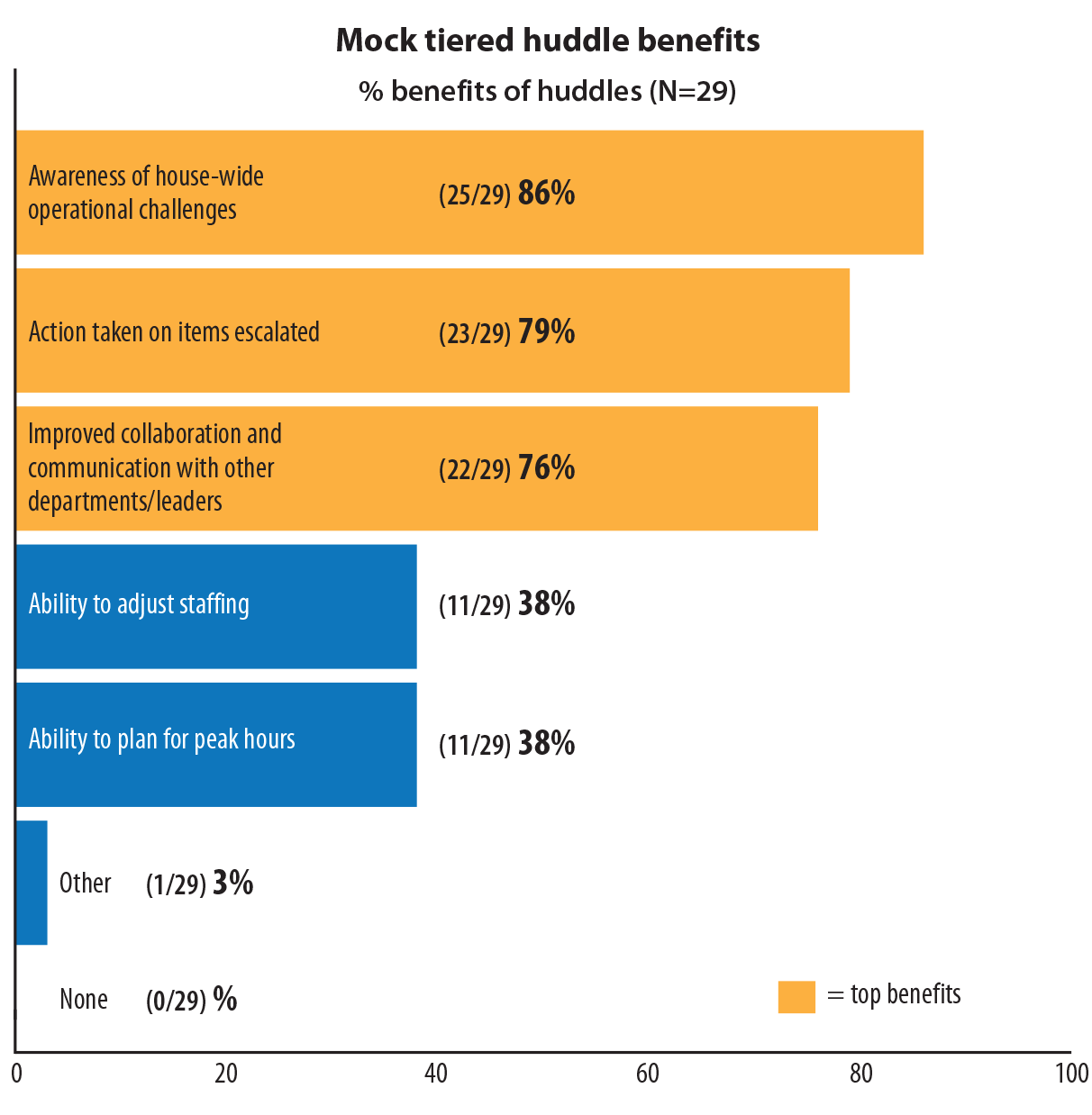
Within a week of implementing the mock huddles, we emailed a short three-question survey to 54 leaders and staff who attended the second tier huddle to gather feedback regarding format, reporting, and agendas. Twenty-nine (54%) respondents completed the survey. They rated their overall satisfaction with the mock tiered huddles as 4 out of 5. (See Survey results: Mock tiered huddles.)
Survey results: Mock tiered huddles
Of the 54 attendees to the mock second tier huddles, 29 responded to the survey requesting feedback. They were asked how satisfied they were with the mock huddle sessions. Respondents also were asked to rate the following benefits on a 1 to 5 scale (they could select as many as they wanted).
Over the following months, the data analytics team and operational leaders worked together to improve the huddle report. They aimed to create a simple and efficient report for leaders to use for generating trending metrics, which the organization could analyze over time. By the end of June 2022, we completed the final version of the report, which offers additional drop-down options for standardized reporting and faster documentation. Operational leaders agreed that it captured the necessary information and that it was easy to use. The analytics team developed a tutorial video and standard operating procedures for huddle documentation. Over 43 leaders and staff viewed the tutorial. The huddle template also includes a peak times section and colors (red, yellow, or green) denoting staffing or volume levels.
At the end of each month, the new tiered huddle report rolls into an organization summary that trends volume, staffing status, and escalations. In addition to an organizational summary view, the team decided that summaries for pharmacy, patient intake services, and the business office would prove vital to analyzing MCI preparedness.
For example, the pharmacy summary report monitors the volume of patients receiving infusions and chemotherapy and the percentage of early compounding. The patient intake services summary reports intake readiness for the day and at 24, 48, and 72 hours. The business office summary tracks the reasons for authorization delays (for example, primary care physician [PCP] referrals, insurance peer-to-peer conversations, patient waiting to see their PCP, and lack of clinical documentation). The summary also tracks the type and number of pending authorizations (such as infusions, radiation, and diagnostics) and those rescheduled due to lack of insurance approval.
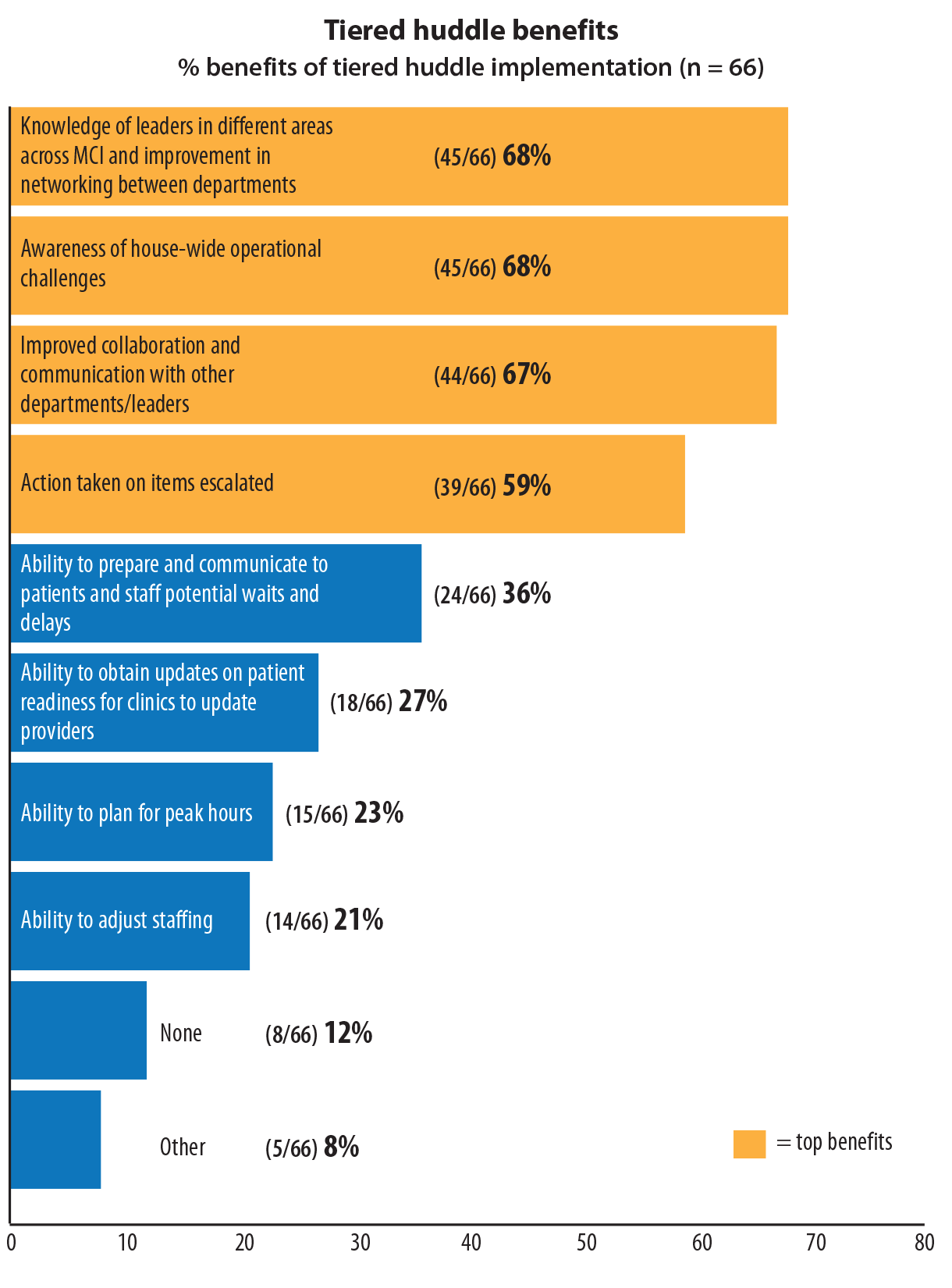
By the end of December 2022, tiered huddles had been in place at MCI for approximately 9 months and the new huddle form for 6 months. We conducted another survey of the second-tier attendees to gather stakeholder perceptions of the impact and benefits of huddles. In the last week of December 2022, 133 leaders and staff received the survey; 66 (50%) responded and gave an overall satisfaction rating of 4 out of 5. Most huddle attendees “agreed” or “strongly agreed” with timely escalation resolutions (69%), huddle efficiency (82%), and ease of obtaining staffing support (57%). (See Second survey results.)
Second survey results
After tiered huddle use for 9 months, 133 leaders and staff who attended second tier huddles received a survey requesting feedback (66 responded). Respondents selected all options perceived applicable to the benefits of tiered huddles.
Positive outcomes
Providing patient-centered care to oncology patients requires an interdisciplinary approach with streamlined communication, collaboration, and teamwork. Tiered huddles have improved organizational communication and positively impacted patient and staff safety and satisfaction. Including operational leaders and staff and receiving the support of executive leadership contributed to tiered huddle success at MCI. Including departments (such as information technology, facilities, and security), which don’t generally attend operational meetings, provided an accurate high-level snapshot of the organization.
Blocking calendars for huddles to prevent simultaneous scheduling of all other meetings, unless crucial to patient care or the organization, allowed leaders and executives to huddle and round with their teams consistently and actively engage in the process. Huddles expose executives to leaders and staff they wouldn’t normally interact with on a daily basis.
Limitations
Challenges to the MCI tiered huddle launch include documentation in the daily huddle report and a gradual decline in issue escalation. Lack of leader and staff adherence to completing the daily report limited the amount of content for analysis; report completion is associated with the value and the priority placed on documenting the information. Especially during the transition from the old to the new report, leaders and staff received routine reminders until most departments were completing the report regularly. However, the process still isn’t perfect. Departments may have a few days missing in a given month. Toward the end of each month, leaders receive reminders to review their reports and fill in any missing dates.
The literature notes awareness and escalation of clinical and operational issues as an important outcome of tiered huddles. MCI’s implementation of tiered huddles saw similar issues arise related to safety, staffing, equipment failure, delays in patient care, information technology, telecommunications interruptions, and patient satisfaction. However, as implementation progressed, frequency of escalation reporting steadily declined; escalations and safety concerns occurred more frequently in the first 4 to 5 months of tiered huddles. We made this discussion a permanent part of the tiered huddle agenda template to remind leaders that they’re encouraged to escalate concerns and seek support.
Reduction of escalations may be attributable to leaders networking and feeling empowered to work cross-functionally to address concerns. For example, silos between departments reduced over time and leaders proactively and independently addressed operational issues directly with each other rather than waiting for huddles to present a problem. Another reason for the decline in the frequency of escalations may be due to organization size and setting. Two of MCI’s smaller off-site locations participate in tiered huddles, but the research articles used for implementation focused on hospital settings within large healthcare systems with more than two tiers.
Nursing implications
Nurses serve as patient advocates, and tiered huddles provide a standard place and time to discuss safety, quality, and efficiency issues that impact patient care. Nurses’ close connection to patients, staff, and physicians at MCI makes their voices essential. They’ve alerted their teams to issues related to delays in initiating chemotherapy infusion because of peripherally inserted central catheter line placement, critical clinical staff shortages, the need to increase the rate of early chemotherapy compounding to decrease infusion delays, and trends in increased appointment cancellations due to lack of authorization. In each instance, the leadership team acknowledged the issue, followed up, and addressed it to closure.
In healthcare, a lack of communication and teamwork can lead to patient safety issues and errors, which can decrease team morale and patient satisfaction. As seen in both surveys, awareness of operational challenges, improved networking, collaboration, and communication were top-scoring benefits. Huddles empower nursing (and non-nursing) leaders and staff to proactively address clinical and operational issues and to collaborate with teams from across MCI.
Consistent connection
After conducting 259 tiered huddles, staff and leaders experienced improved communication and networking across the cancer center. Awareness of operational challenges increased and teams worked together to address operational and safety concerns. Leaders perceived that appropriate departments promptly addressed concerns raised at huddles, and more leaders obtained and shared staffing resources. Tiered huddles also provided nursing and provider teams with insight into the clinical and operational challenges of the day so they could adjust the patient plan of care, clinic operations, and patient communication accordingly.
The next phase of tiered huddles at MCI will focus on the organization’s view of the huddle report to analyze staffing resources, ongoing operational efficiency opportunities, and improve access to care in partnership with external community practices and hospitals.
Smooth operations and efficient patient care at MCI depend on staffing and daily census awareness, chart readiness, early compounding of chemotherapies, and timely authorizations. Monday through Friday, the executive team, nursing, and operational leaders have a consistent time and place to obtain insight into daily clinical and nonclinical operations, quickly resolve problems and gaps in care or services, and connect to MCI’s mission and vision.
Marguerite Rowell is the assistant vice president of nursing at the Miami Cancer Institute of Baptist Health South Florida in Miami.
American Nurse Journal. 2024; 19(2). Doi: 10.51256/ANJ022444
References
Adapa K, Ivester T, Shea C, et al. The effect of a system-level tiered huddle system on reporting patient safety events: An interrupted time series analysis. Jt Comm J Qual Patient Saf. 2022;48(12):642-52. doi:10.1016/j.jcjq.2022.08.005
Advisory Board. 3 key lessons of Intermountain’s 15-minute daily huddles, according to CEO Marc Harrison. March 24, 2023. advisory.com/daily-briefing/2018/12/03/intermountain
Baloh J, Zhu X, Ward MM. Implementing team huddles in small rural hospitals: How does the Kotter model of change apply? J Nurs Manag. 2018;26(5):571-8. doi:10.1111/jonm.12584
Bermo K, Oldham L, Sewell N, Laggner M. Improving bi-directional communication within nursing service by implementing a tiered huddle structure. Sigma Repository. https://sigma.nursingrepository.org/handle/10755/21486
Harrison M. How a U.S. health care system uses 15-minute huddles to
keep 23 hospitals aligned. Harvard Business Review. November 29, 2018. hbr.org/2018/11/how-a-u-s-health-care-system-uses-15-minute-huddles-to-keep-23-hospitals-aligned
Harrison M. Tiered escalation huddles yield rapid results. NEJM Catalyst Carryover. March 7, 2018.
Hung DY, Rundall TG, Lee J, Khandel N, Shortell SM. Managing through a pandemic: A daily management system for COVID-19 response and recovery. J Healthc Manag. 2022;67(6):446-57. doi:10.1097/jhm-d-21-00319
Merchant NB, O’Neal J, Montoya A, Cox GR, Murray JS. Creating a process for the implementation of tiered huddles in a Veterans Affairs medical center. Mil Med. 2023;188(5-6):901-6. doi:10.1093/milmed/usac073
Mihaljevic T. Tiered daily huddles: The power of teamwork in managing large healthcare organisations. BMJ Qual Saf. 2020;29(12):1050-2. doi:10.1136/bmjqs-2019-010575
Parker AL, Forsythe LL, Kohlmorgen IK. TeamSTEPPS®: An evidence-based approach to reduce clinical errors threatening safety in outpatient settings: An integrative review. J Healthc Risk Manag. 2019;38(4):19-31. doi:10.1002/jhrm.21352
Ryan PT, Merlino J. Intermountain Healthcare embraces transformation. AHA Trustee Services. trustees.aha.org/performanceimprovement/articles/intermountain-healthcare-embraces-transformation
Shahid S, Thomas S. Situation, background, assessment, recommendation (SBAR) communication tool for handoff in health care – A narrative review. Saf Health. 2018;4(1):7. doi:10.1186/s40886-018-0073-1
Key words: tiered huddles, patient safety, quality improvement, communication, teamwork















