

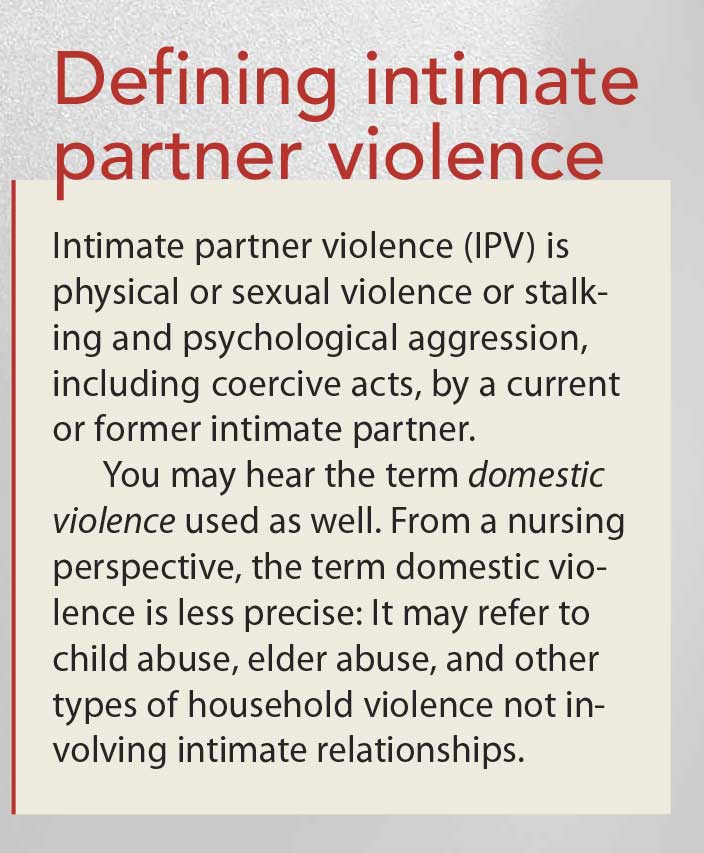
A patient who experiences violence at the hands of a spouse or partner may think of it as a personal and private matter, but intimate partner violence (IPV) has serious health consequences. Severe mental and physical harm may result from an intimate relationship that has gotten out of control, and, ultimately, life itself may be at risk. (See Defining intimate partner violence.)
The personal nature of IPV is part of what makes it such a serious health risk. Emotional ties can hinder a patient from acknowledging or protecting himself or herself against violence inflicted by the partner. Most people want a partner or spouse with whom they can share their life. When a relationship turns violent, devotion can become deadly, giving a frightening and disturbing meaning to the expression “till death do us part.”
What’s more, signs of IPV are not always visible or easily detected. Identifying a patient at risk for this type of violence and protecting him or her from potential harm, are important nursing skills.
A highly prevalent danger
High rates of IPV make it a concern for society and a challenge to the nursing profession. According to the Centers for Disease Control and Prevention (CDC), IPV affects one in three women in the United States in the course of their lifetime. In addition, many people are surprised to learn that the CDC estimates one in four men experience this type of violence in their lifetime.
Consider also that researchers may underestimate how often IPV occurs. People seeking medical care commonly won’t reveal this type of violence and may hide injuries that result from it.
Understanding this type of violence, and how to screen for it, will strengthen your ability to preserve your patients’ health and well-being. You need to know how to establish trust with patients at risk, screen for this dangerous situation, and recognize ways you can intervene.
Effective screening
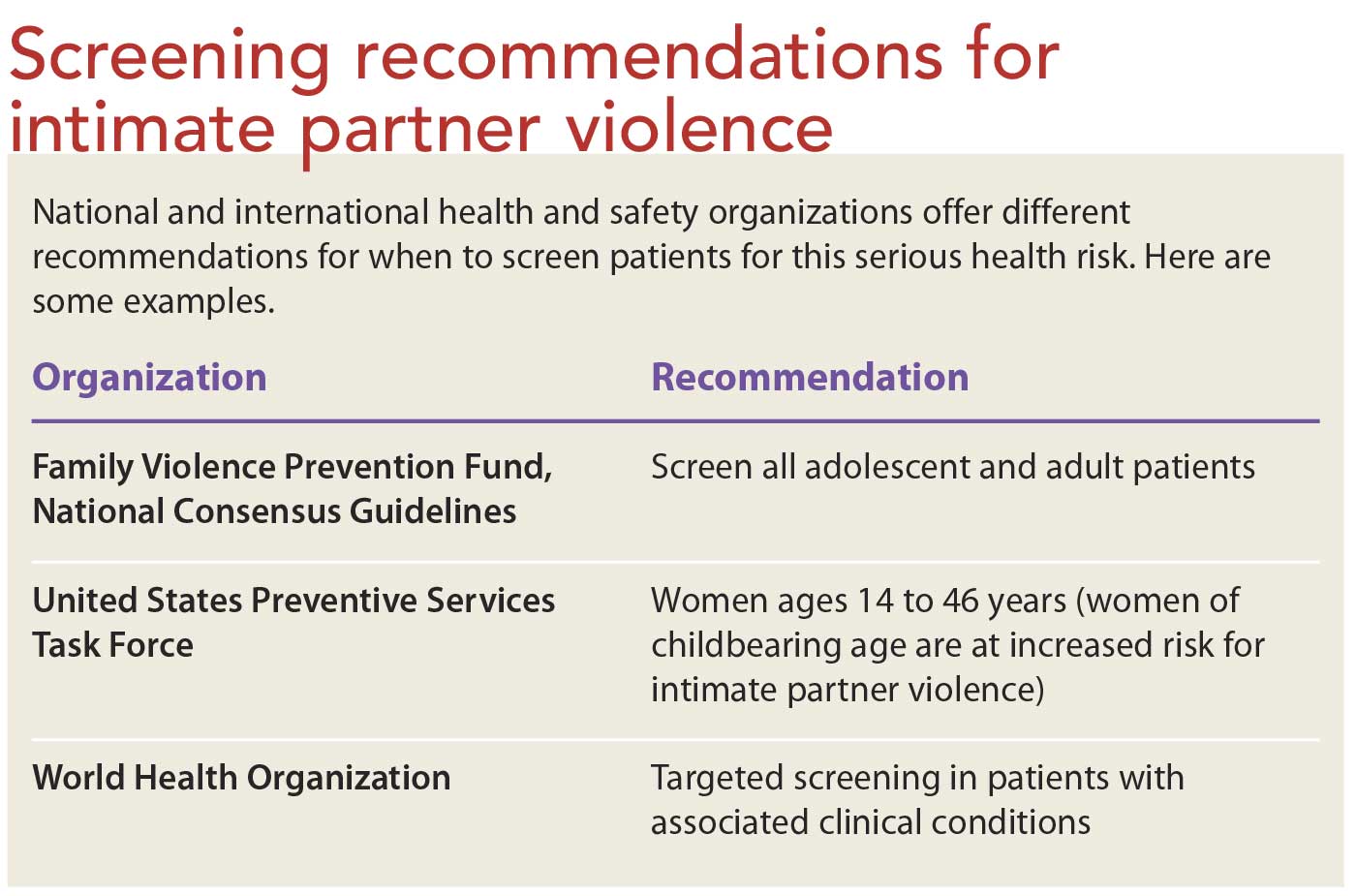
You can’t rely on any single standard test or indicator when assessing for IPV. Recommendations for when to screen issued by national and international health and safety organizations vary. (See Screening recommendations for intimate partner violence.) Be familiar with policies your employer has in place related to assessment and care of victims of violence.
One common thread links victims of IPV: the victim knows the perpetrator, knows him or her well, and vice versa. Indeed, the perpetrator may accompany the victim to a hospital, physician’s office, or urgent care center. He or she may try to prevent you from examining the victim privately. Many facilities place signs in waiting areas advocating patient privacy and stating that healthcare providers see patients alone in the exam room.
Effective screening depends on your ability to maintain a nonjudgmental attitude. As a nurse, you set the stage for establishing a trusting and open relationship with the patient.
Foster open communication
In addition to ensuring privacy, take steps to establish trust. Victims may be embarrassed or afraid and reluctant to discuss their situation, so project a supportive attitude. Make eye contact and never rush or talk down to the victim.
Be aware of and discard any preconceptions you may hold regarding IPV. This type of violence isn’t restricted to any gender, race, age, ethnicity, or social class. It may occur in opposite-sex or same-sex relationships, and it affects people from all cultures and all walks of life.
Become comfortable with introducing the topic of IPV. Developing a standard approach to raising this sensitive subject to patients can help. For example, you might say, “Nurses look upon violence as a health issue. We now ask every patient about safety and health. Know that everything we discuss is confidential. Nothing you say will leave this room unless you clearly tell me it’s okay to share the information.”
Recognize male and female patients’ different needs
Women are more likely than men to disclose IPV to a healthcare provider. In contrast to men, women usually experience more severe physical violence and longterm effects. In addition, pregnant victims face risks for their unborn child’s health and safety.
Research indicates men may experience embarrassment or fear they will not be believed, making them less willing to disclose violence at the hands of an intimate partner. Men may think that healthcare professionals will automatically perceive them as the perpetrator rather than the victim.
Consider developing a standard approach to introducing the topic of IPV to male patients. For example, you might say, “IPV is a significant healthcare problem for many men. Research suggests that one out of four men experience IPV in their lifetime. We are here to help and provide referrals for you or anyone who may need assistance.”
Be aware that women may feel the same embarrassment about IPV that men commonly experience.
Use a screening tool
Many IPV screening tools are available; no single tool is best. One common, easy-to-use tool is HITS, which stands for Hurt, Insult, Threaten, and Scream. This tool is based on four simple questions.
How often has your partner:
• hurt you physically?
• insulted you or talked down to you?
• threatened you with harm?
• screamed or cursed at you?
Questions are individually scored from one point (never) to five points (frequently), with a total of 10 or more points indicating IPV. This screening tool is available as an app called R3—Recognize, Respond, Refer.
Assess barriers to effective screening
Be prepared to encounter victims of IPV who refuse to acknowledge abuse has taken place. Even if the patient contradicts your findings, respect his or her feelings and right to privacy. Acknowledging the patient’s response will help you gain his or her trust. You can express your concern by making an impersonal, generalized statement, communicating simply but directly that IPV is a serious and widespread problem. For example, you might say, “I am glad that you are not exposed to any violence. Unfortunately, abuse by an intimate partner is a common problem in our community. Would you like to take some informational resources in case you know someone who may need them?” Developing a standard way to address patients whom you suspect are denying abuse may help you deal with this sensitive situation.
Refrain from beginning the screening if circumstances make it unsafe. If you can’t secure a safe private area or if a foreign language interpreter is needed but not available, do not initiate screening. Any attempt to move forward with screening may cause the patient additional harm.
Identify clinical and behavioral signs and symptoms
Clinical signs and symptoms that may be associated with abuse by an intimate partner include frequent bladder infections, head or neck injury, chronic GI symptoms, eating and sleeping disorders, headaches, sexual dysfunction, sexually transmitted diseases, anxiety, depression, and lethargy.
Also be aware of behavioral signs and symptoms such as frequent healthcare visits, failure to follow up, alcohol or substance abuse, and recent divorce or separation. Note if the patient’s intimate partner exhibits signs of physical aggression, emotional abuse, or controlling behavior.
Be alert for statements that may indicate forced sexual activity. For example, a patient may say “I had multiple sexual partners during times my husband needed extra money.” This statement may indicate their spouse forced them into prostitution. Follow-up is required.
Helping the patient
If the patient admits to experiencing IPV, acknowledge his or her feelings and be supportive. The patient may need to overcome considerable shame and embarrassment to make this admission. Recognize the courage it took to come forth, and respond with sensitivity. For example, consider saying, “I am sorry you have been hurt, but I appreciate your willingness to speak openly about it. Help is available for you.”
Next, assess current safety risk; victims of IPV face greater than average risk of death by homicide. Ask the patient if a weapon is kept at home. If yes, ask if he or she has been threatened with it. Also, question if abuse has increased in the last 6 months, whether the partner is obsessive or jealous, and if children live at home. Assess for suicidal risk. If the patient is female, ask if she is pregnant.
Develop a safety plan
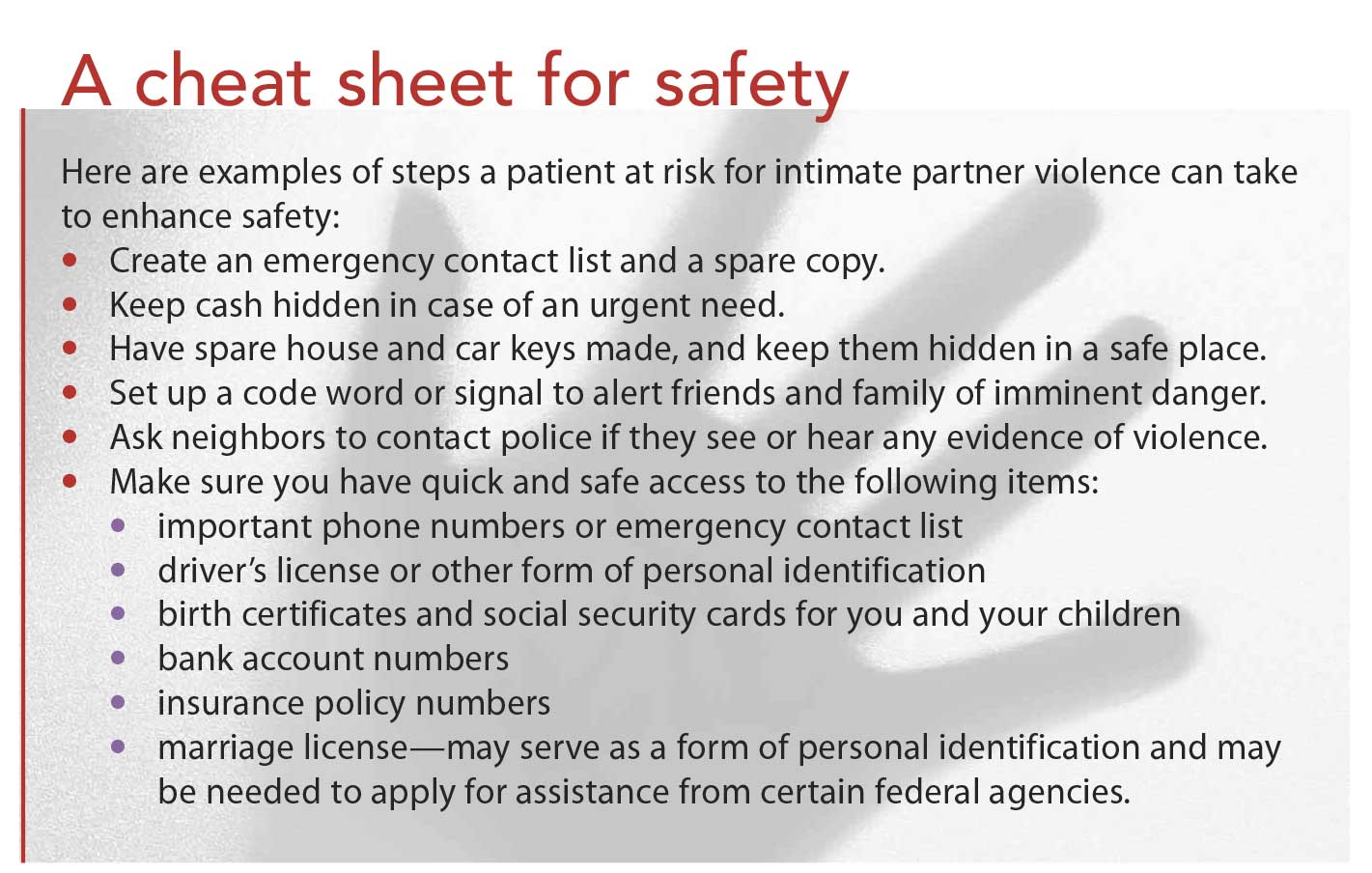
Help the patient find the best way to cope with an unsafe situation. Work with him or her to develop a safety plan. (See A cheat sheet for safety.) This plan must be realistically tailored to a patient’s individual circumstances. Identify steps patients can take to ensure their safety. Encourage them to plan ahead should tension escalate, and tell them to:
• have a plan and provisions in place for a safe escape
• plan ahead for a safe place to go
• have essentials packed and kept as close as possible to an exit from their home.
If returning home isn’t safe, direct patients to available resources, such as police, legal assistance, and alternative housing.
Offer information and support
Help the patient obtain the information and support he or she needs. When offering information, make sure the patient can take printed materials home safely.
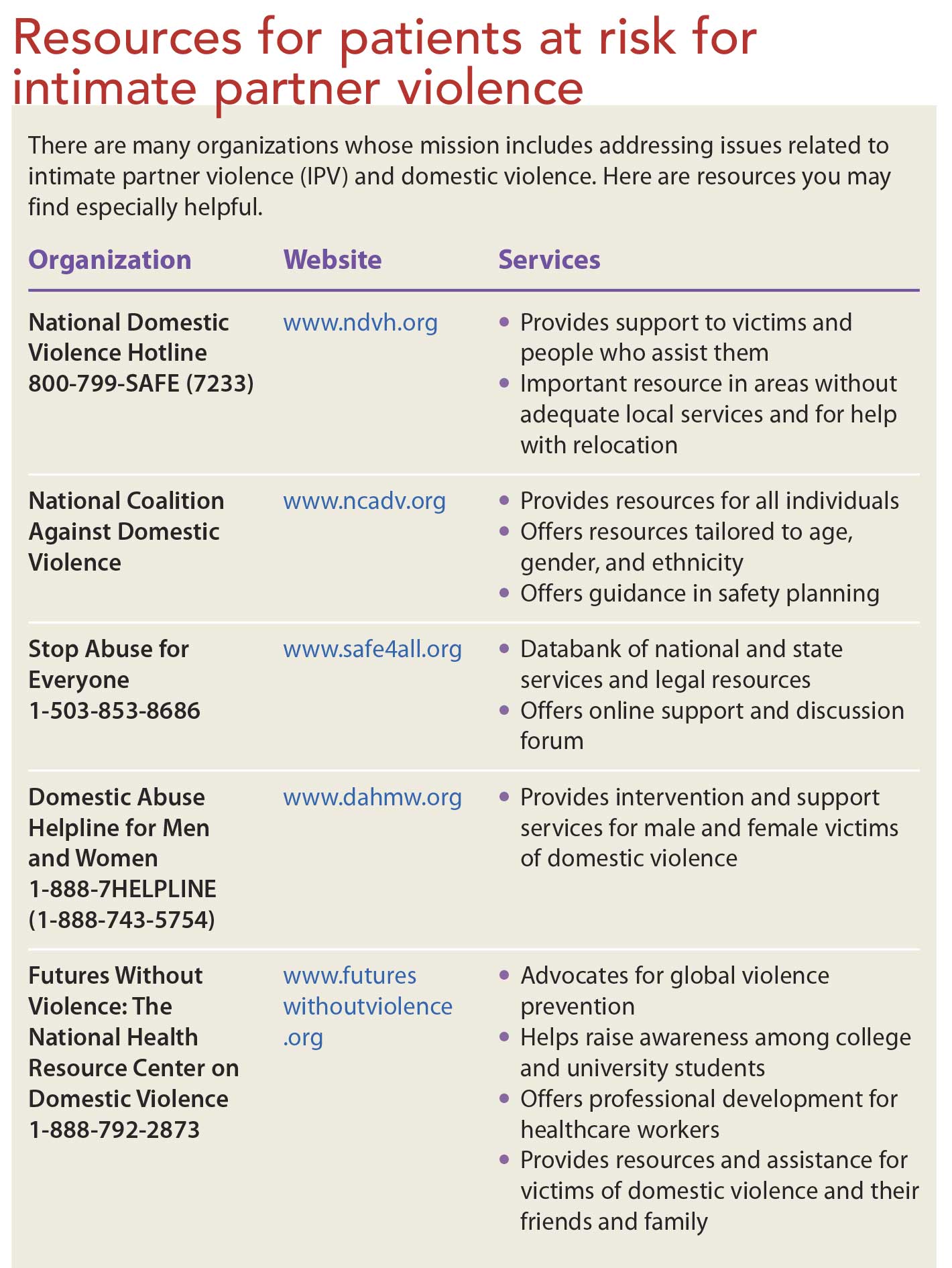
Inform him or her about national and locally based support services. (See Resources for patients at risk for intimate partner violence.) For example, the National Domestic Violence Hotline (1-800-799-SAFE [7233]) offers crisis intervention, safety planning, and referral services. It is available 24 hours a day and has interpreters for more than 100 languages.
Another example of a resource available to patients is the Aspire News App, which is available free from an organization called When Georgia Smiled. The home page of this app appears like a regular news app, but the Help section is designed for people in domestic violence situations. It includes options for quickly accessing a list of local sources of support and alerting chosencontacts and local authorities, if the need arises. The creators of this app note that it is not meant as a substitute for emergency 911 services.
Advise patients to turn on the location setting on their cellphone to assist law enforcement in locating them if it becomes necessary; for example, if they are taken to a remote location against their will.
Many communities lack shelters for men who experience domestic violence. Help the patient explore alternative living arrangements, if necessary.
Document your findings
Document screening and assessment findings, patient responses, implementation plan, referrals, and your plan follow-up. Quote the patient’s responses to your questions, rather than your interpretation of what he or she says. For example, instead of writing “patient reports being beaten by her husband,” document what the patient said—“My husband was mad at me for not having dinner cooked on time. He punched me in my eye in front of our children, and I fell onto the ground. It made me dizzy. My eye hurts and is swollen now.”
Precise documentation establishes clear communication to the healthcare team members. Accuracy is also important because the documentation may be used in future court proceedings involving the patient.
Balance nursing goals
Your initial screening and discussion with patients who experience IPV may be their most important avenue for future assistance. At the same time, you must also accept the reality that patients may not be ready to seek help, nor may they be able to leave the relationship, no matter how abusive it appears in your eyes.
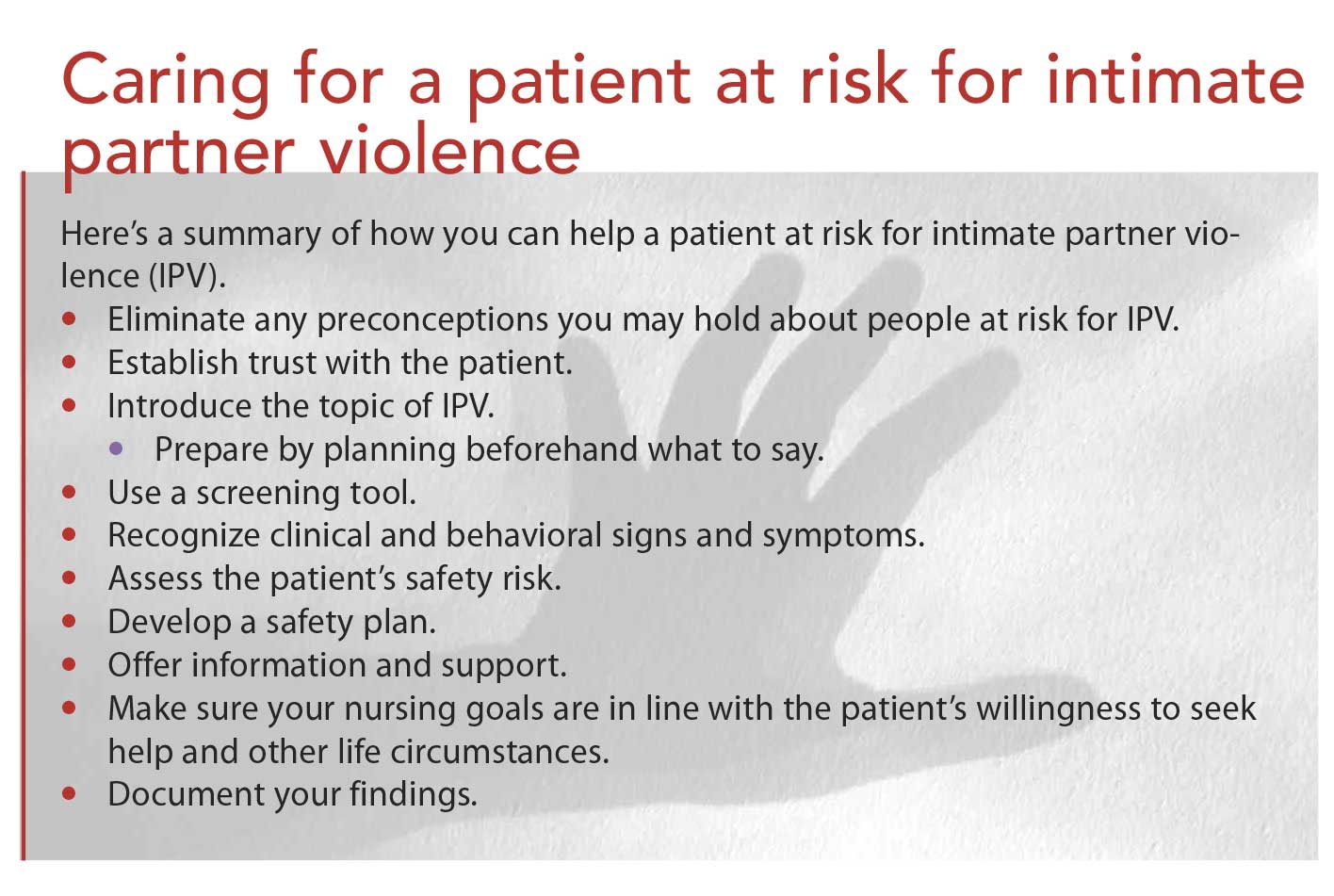
None of this changes your responsibility as a nurse and patient advocate. Your goal is the same: bring up the topic, establish a trusting relationship, and educate the patient on the available resources. For quick summary of your role, see Caring for a patient at risk for intimate partner violence.
Jessica McCarthy is an instructor at the University of Louisiana at Lafayette and a family nurse practitioner at the Minute Med Walk-In Clinic in that city. She is also a student in the Doctor of Nursing Practice (DNP) program at the University of Alabama at Huntsville. Janell Williams is an advanced practice registered nurse at Tennessee Valley Healthcare in Murfreesboro and a student in the DNP program at University of Alabama at Huntsville. Azita Amiri is an assistant professor at the University of Alabama in Huntsville.
Selected references
Breiding MJ, Smith SG, Basile KC, Walters ML, Jieru C, Merrick MT. Prevalence and characteristics of sexual violence, stalking, and intimate partner violence victimization—national Intimate partner and sexual violence survey, United States, 2011. MMWR Surveill Summ. 2014;63(8):1-18.
Brown MJ, Weitzen S, Lapane KL. Association between intimate partner violence and preventive screening among women. J Womens Health (Larchmt). 2013;22(11):947-52.
Dudgeon A, Evanson TA. Intimate partner violence in rural U.S. areas: what every nurse should know. Am J Nurs. 2014;114(5):26-35; 36, 48.
Singh V, Petersen K, Singh SR. Intimate partner violence victimization: identification and response in primary care. Prim Care. 2014;41(2):261-281.
Valpied J, Hegarty K. Intimate partner abuse: identifying, caring for and helping women in healthcare settings. Womens Health (Lond). 2015;11(1):51-63.















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}