
Take a strategic approach to translating research into practice.
Takeaways
- Implementation is a major step in the evidence-based practice (EBP) process that’s often underappreciated and under-resourced, resulting in delays in using evidence in clinical practice settings.
- Implementation models for promoting uptake of EBP through strategic efforts and use of a toolbox of strategies can promote successful practice changes.
- The success of EBP initiatives depends on multiple strategies that are aligned with the stage or phase of readiness for a practice change.
 YOU’RE UNLIKELY to find a practicing nurse who hasn’t heard of evidence-based practice (EBP). Nurses are keenly aware of the expectation that they promote patient safety and quality care with the best available evidence. Aligned with these expectations, nursing education programs prepare new graduates with a foundation in EBP as a decision-making approach to patient care. Moreover, consumers and third-party payors expect evidence-based care along with value-based purchasing that reimburses for quality outcomes rather than number of procedures.
YOU’RE UNLIKELY to find a practicing nurse who hasn’t heard of evidence-based practice (EBP). Nurses are keenly aware of the expectation that they promote patient safety and quality care with the best available evidence. Aligned with these expectations, nursing education programs prepare new graduates with a foundation in EBP as a decision-making approach to patient care. Moreover, consumers and third-party payors expect evidence-based care along with value-based purchasing that reimburses for quality outcomes rather than number of procedures.
Despite these expectations, reports continue of challenges and barriers to initiating and sustaining an EBP change. Nearly 20 years ago, Balas and colleagues determined that the average time for scientific evidence to be translated into practice is 17 years. What’s even more striking is that this delay was for the 14% of evidence-based interventions that ever get translated. These observations have led to the development of translation and implementation science, which aims to reduce delays and understand what factors facilitate the successful adoption and implementation of new knowledge into practice.
Many evidence-based models have emerged to guide implementation through the stages of change. This article will review EBP implementation models, summarize key resources for selecting implementation strategies, and present a case study using an implementation model that promotes successful uptake of evidence into practice.
EBP implementation models
Nilsen published a summary of implementation models, frameworks, and theories that have been developed in implementation science to advance EBP and expedite uptake of evidence into real-world settings. He categorized the approaches as models that guide the process and steps of moving research into practice, frameworks for understanding and exploring factors that influence implementation, classic theories that explain change processes, specific implementation models, and evaluation frameworks.
Process models
Process models are action or application oriented and take a how-to approach. They’re common in nursing because nurses value practical approaches to improving practice.
Examples: The Iowa EBP Model was developed and originally implemented at the University of Iowa Hospitals and Clinics to serve as a guide to help nurses and other health care providers use research findings to improve patient care. The Advancing Research and Clinical Practice through Close Collaboration Model developed by Melnyk and colleagues begins with an organizational assessment of EBP readiness, emphasizes EBP mentors, and promotes changing beliefs and skills about EBP.
Determinants and evaluation frameworks
Determinants frameworks emphasize specific factors or characteristics that will improve the uptake of evidence into practice. They aim to improve adherence to guidelines or EBPs by leveraging enabling factors and minimizing barriers. They specify barrier and facilitator characteristics that influence implementation outcomes, with some frameworks specifying relationships between char acteristics and determinants. Eval – uation frameworks provide structure for evaluating the translation of an evidence-based practice change and addressing processes and outcomes of the change.
Examples: The Promoting Action on Research Implementation in Health Services framework emphasizes the characteristics of the evidence, the context for the adoption of the evidence (including leadership and culture), and facilitation (person and processes) that promotes the EBP initiative and implementation strategies.
The Consolidated Framework for Implementation Research addresses the gap between what research trials have shown to work and what actually occurs in real practice settings. It includes an overarching taxonomy and includes five major domains: intervention characteristics, outer setting, inner setting, individual characteristics, and processes. Addressing these domains helps facilitate the successful uptake of evidence into practice.
The Reach, Effectiveness, Adoption, Implementation, and Maintenance evaluation framework originally aimed to provide a consistent reporting mechanism for intervention studies. It has more recently been used to translate research into practice and to help plan programs and improve their chances of working in real-world settings. Questions related to this model are: What pop – ulation will be/was reached? What is/was the impact of the intervention, including positive and negative outcomes? What adoptions will be/were implemented for real-world population uptake? What implementation strategies will be/were used? How will/was the practice change maintained?
Implementation and classic theories
Implementation theories were developed to advance knowledge about best strategies and processes for promoting evidence uptake. They build on classic (social cognitive theory, theory of diffusion of innovation) and change theories from other fields. Everett Rogers developed the theory of diffusion of innovation, which is widely used to promote the spread and adoption of new ideas. It recognizes that relative advantage, compatibility, complexity, trialability, and observability are key characteristics to expedite change adoption and that ideas undergo stages of adoption: build knowledge about the innovation, build persuasion and interest in the innovation, make a decision about adopting the innovation or practice change, implement the innovation/practice change, and confirm whether to continue. Rogers also emphasized that types of adopt – ers (innovators, early adopters, early majority, late majority, and laggards) influence rate and success of new idea adoption.
Examples: The Transtheoretical Model (TTM), also known as Stages of Change Model, proposes that people move through a series of stages when modifying behavior. Different principles and processes of change work best at each stage to reduce resistance, facilitate progress, and prevent drift back to old behavior. (See Transtheoretical Model.)
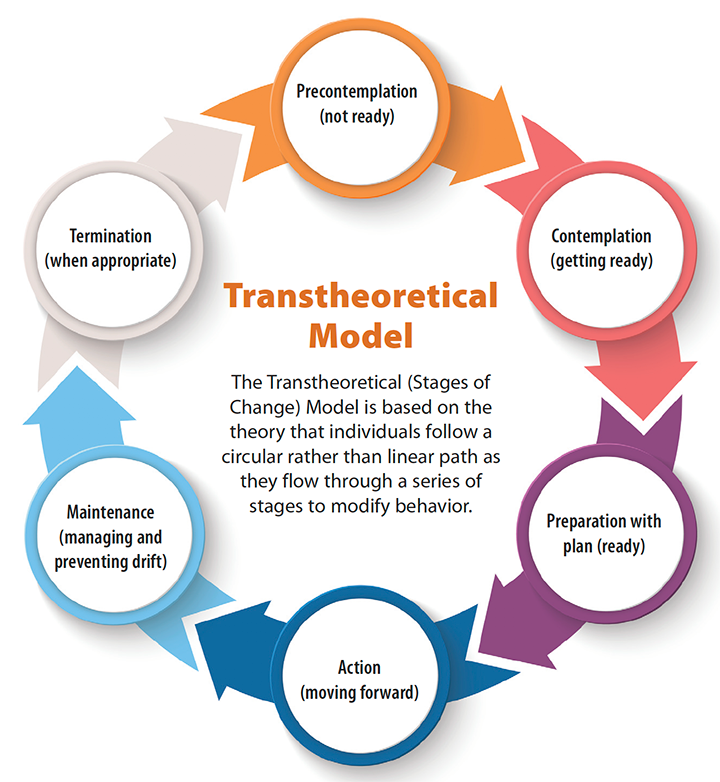
Case studyThis case study uses TTM (stages of change) to illustrate the value of EBP implementation models to guide strategy selection. Like individuals making behavior change, groups and organizations also experience different levels of readiness to change. The TTM stages can guide the selection of implementation strategies. Case description An organization with an opioid use reduction program decides to integrate evidence-based nonpharmacologic interventions for pain control in patients with chronic pain (such as back pain) admitted to a hospital unit for acute pain (such as fractured wrist needing surgery). Precontemplation stage (not ready) At this stage, many staff members and leaders may feel that the current practice is working fine, and they aren’t open to exploring change. Maybe the timing isn’t right, the initiative isn’t aligned with organizational strategic priorities, resources aren’t available, or leadership isn’t on board. Nursing staff and leaders operating in this stage may view offering nonpharmacologic interventions for shortterm patients admitted to the hospital as unnecessary given other patient care demands, or maybe they think the intervention is more appropriate for the outpatient practice. Implementation strategies: Engage leadership in discussions about pain management and opioid concerns and aligning the change with strategic priorities. Staff should explore attitudes and goals about nonpharma – cologic pain management to understand resistance they encounter and offer evidence about opioids and nonpharmacologic interventions. Facts can be reviewed in a workshop, newsletter, or a journal club facilitated by opinion leaders or champions. Contemplation stage (getting ready) Staff are aware that integrating nonpharmacologic pain management strategies is aligned with the organization’s opioid use reduction program. Organizational leaders are responding to regulations and national mandates, and they’re aware of opioid-related mortality rates within their practices and geographic region. They may appoint a task force to examine the issue and current practices, or an interprofessional team may convene on its own to discuss their opioid use practices and the integration of nonpharmacologic strategies to augment pain management. Implementation strategies: Begin by exploring expectations about using nonpharmacologic interventions with staff and then summarizing their pros and cons. Engage leaders and staff in discussions about national opioid use concerns, their own current opioid practices, and desired outcomes. Provide education and share best evidence to build staff confidence in delivering nonpharmacologic interventions. Continue to engage local champions. Preparation stage (ready) Staff and leaders are ready to take action within a specified time period, a literature review is conducted, and an action plan is developed. In the case example, leaders would request an EBP initiative, and an interprofessional team would form and create an EBP question. (See Framing the question.) |
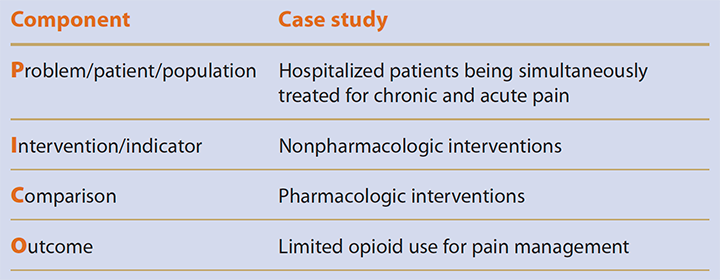
Framing the QuestionA common tool to help frame an evidence-based practice (EBP) question is problem/patient/population, intervention/indicator, comparison, and outcome (PICO). Here’s how the tool was applied in the case study
The team combined the elements into this EBP question: In hospitalized patients being simultaneously treated for chronic and acute pain, what nonpharmacologic interventions can augment pharmacologic interventions and limit opioid use as compared to opioid use only for pain management? |
| Implementation strategies: Multiple implementation strategies can be used in this stage to ensure successful adoption of the practice by all staff. Create an interprofessional team with a committed leader who attends planning discussions and supports needed resources and time. Before launching, identify and manage barriers to practice change, such as resources, lack of knowledge, negative attitudes among select and influential staff, and lack of leader modeling and engagement. The leader will work with the team to create an action plan with a timeline and key accountable people. Collect baseline data for evaluating the practice change and communicate (through formal announcements and informal discussions) with all stakeholders, including patients, families, and staff. Implement a toolkit with several nonpharmacologic options and create quick references cards about opioid assessment and nonpharmacologic pain management approaches. Plan training and education sessions and create a patient and family education pamphlet. Rally early adopters. Action stage (moving forward) At this point, the practice change should be in process with multiple implementation strategies to increase evidence uptake. Leaders designate resources, such as information technology, to conduct and evaluate the change. The goal is to keep the change moving forward. In the case study, administrative support is observed with resource allocation. One nursing unit may pilot the practice change to routinely offer nonpharmacologic interventions to patients experiencing pain to augment pharmacologic strategies. Implementation strategies: Multiple implementation strategies are purposefully selected to maintain the practice change momentum. Frequently measure outcomes such as pain ratings, opioid use, and nonpharmacologic interventions. Flexible selflearning modules and pocket reference cards can help staff gain confidence with the new practice. Electronic health record prompts, other types of remind – ers, and reports to leadership reinforce the new practice. In addition, patient education and support help ensure success. Maintenance stage (managing and preventing drift) This stage demands ongoing effort and resources to ensure the practice becomes hardwired and replaces the old practice. This may take weeks, months, and even years. In the case study, staff work to maintain their commitment to offering patients nonpharmacologic pain strategies. Leaders must offer ongoing support and encouragement, continue auditing/monitoring, and provide feedback. Booster training may be needed for existing staff and a structured process created for onboarding new staff. Implementation strategies: Several implementation strategies can help maintain the practice change. Monitor data trends, report data to senior leaders, and encourage leadership rounds to ask about nonpharmacologic interventions. Project team members and unit leaders should continue to celebrate and recognize success and support champions with incentives and rewards. Address resistance as soon as it’s identified. Other strategies include rolling out the practice to other units, recognizing that drift back to the old practice can occur at any time, changing the reminder mechanisms, continuing to review literature and new evidence at regular intervals, setting new goals and objectives as needed, updating action plans, reporting to quality improvement teams, presenting project details and data through informal and formal presentations, and including project reports in annual reports. Termination stage (when appropriate) If the practice is truly hardwired, no additional efforts are needed to sustain the change, and the implementation process can be terminated. This stage may not be reached for a long time and may not be appropriate for many practice changes. Or maybe the practice isn’t feasible or effective and it should be abandoned. Implementation strategies: Specific implementation strategies at this stage begin with determining if terminating the team efforts is appropriate. In the case study, if termination can occur, team members will want to identify what indicators suggest that the nonpharmacologic interventions are consistently used and which focused implementation strategies are no longer needed. Leadership will be responsible for ongoing monitoring of data trends and adherence to the practice change. If evidence of practice drift back is identified, the implementation project may need to be resumed or a new project created. Thank and celebrate all staff members, as a group and individually, and consider thank-you gifts for project team members. Termination interviews or focus groups can help the organization learn which implementation strategies were most effective. Implementation strategies: Multiple implementation strategies can be used in this stage to ensure successful adoption of the practice by all staff. Create an interprofessional team with a committed leader who attends planning discussions and supports needed resources and time. Before launching, identify and manage barriers to practice change, such as resources, lack of knowledge, negative attitudes among select and influential staff, and lack of leader modeling and engagement. The leader will work with the team to create an action plan with a timeline and key accountable people. Collect baseline data for evaluating the practice change and communicate (through formal announcements and informal discussions) with all stakeholders, including patients, families, and staff. Implement a toolkit with several nonpharmacologic options and create quick references cards about opioid assessment and nonpharmacologic pain management approaches. Plan training and education sessions and create a patient and family education pamphlet. Rally early adopters. Action stage (moving forward) At this point, the practice change should be in process with multiple implementation strategies to increase evidence uptake. Leaders designate resources, such as information technology, to conduct and evaluate the change. The goal is to keep the change moving forward. In the case study, administrative support is observed with resource allocation. One nursing unit may pilot the practice change to routinely offer nonpharmacologic interventions to patients experiencing pain to augment pharmacologic strategies. Implementation strategies: Multiple implementation strategies are purposefully selected to maintain the practice change momentum. Frequently measure outcomes such as pain ratings, opioid use, and nonpharmacologic interventions. Flexible selflearning modules and pocket reference cards can help staff gain confidence with the new practice. Electronic health record prompts, other types of remind – ers, and reports to leadership reinforce the new practice. In addition, patient education and support help ensure success. Maintenance stage (managing and preventing drift) This stage demands ongoing effort and resources to ensure the practice becomes hardwired and replaces the old practice. This may take weeks, months, and even years. In the case study, staff work to maintain their commitment to offering patients nonpharmacologic pain strategies. Leaders must offer ongoing support and encouragement, continue auditing/monitoring, and provide feedback. Booster training may be needed for existing staff and a structured process created for onboarding new staff. Implementation strategies: Several implementation strategies can help maintain the practice change. Monitor data trends, report data to senior leaders, and encourage leadership rounds to ask about nonpharmacologic interventions. Project team members and unit leaders should continue to celebrate and recognize success and support champions with incentives and rewards. Address resistance as soon as it’s identified. Other strategies include rolling out the practice to other units, recognizing that drift back to the old practice can occur at any time, changing the reminder mech a ni – sms, continuing to review literature and new evidence at regular intervals, setting new goals and objectives as needed, updating action plans, reporting to quality improvement teams, presenting project details and data through informal and formal presentations, and including project reports in annual reports. Termination stage (when appropriate) If the practice is truly hardwired, no additional efforts are needed to sustain the change, and the implementation process can be terminated. This stage may not be reached for a long time and may not be appropriate for many practice changes. Or maybe the practice isn’t feasible or effective and it should be abandoned. Implementation strategies: Specific implementation strategies at this stage begin with determining if terminating the team efforts is appropriate. In the case study, if termination can occur, team members will want to identify what indicators suggest that the nonpharmacologic interventions are consistently used and which focused implementation strategies are no longer needed. Leadership will be responsible for ongoing monitoring of data trends and adherence to the practice change. If evidence of practice drift back is identified, the implementation project may need to be resumed or a new project created. Thank and celebrate all staff members, as a group and individually, and consider thank-you gifts for project team members. Termination interviews or focus groups can help the organization learn which implementation strategies were most effective. |
EBP uptake strategies
A by-product of developing implementation models is identifying strategies for a successful EBP initiative. These strategies generally fall into seven categories: leadership, coaching, communication, reinforcement, recognition, measurement, and reporting.
The following references were selected to highlight key implementation strategies that nurses can use in their EBP initiatives. Keep in mind that a toolbox of strategies will improve success. A different strategy may be needed at each phase of the initiative, for use with barriers and facilitators, and in specific settings. These strategies can be used with each of the models described above.
Grol and Grimshaw: Over 15 years ago, Grol and Grimshaw summarized 54 reviews about how to successfully change practice. They focused on three areas: attributes of the practice, including its complexity and difference from usual practice; barriers and facilitators within the practice change setting and people involved; and the effectiveness of the most frequently used strategies for promoting change.
Grol and Grimshaw found that education strategies, audit and feedback, and reminders and computers are important for successful change. They also recommended interactive small group meetings, mass media campaigns, and combined strategies. The authors concluded that change generally requires comprehensive approaches at different levels and for different interventions, and that a one-size-fits-all approach is unlikely to be successful.
Grimshaw and colleagues: Grimshaw and colleagues suggested that successfully translating research into practice requires asking five key questions:
- What research evidence should be translated?
- Who should the evidence be transferred to?
- Who should translate or deliver the evidence?
- How should the evidence be translated?
- What effects can be expected from the translation?
The authors stressed that a critical first step is assessing organizational barriers and facilitators specific to the proposed practice change. This assessment can guide implementation strategy selection. They also reviewed the latest evidence on various implementation strategies and highlighted the most effective: Holding educational meetings and providing learning materials, leveraging the influence of local opinion leaders, auditing clinician documentation and providing specific feedback, and building computerized reminders. In addition, they noted patient strategies— such as patient decision aids, interactive health communication apps, and communication before consultations to introduce recommended health behavior— that can help facilitate health behavior change.
University of Iowa Hospitals and Clinics (UIHC) Resources: For decades, UIHC nurses have been EBP leaders. The Iowa EBP Model is a key product of this group’s work. Using this model, UIHC teams identified the complexity of EBP implementation. From their observations, UIHC colleagues Cullen and Adams built on Rogers’ theory of innovation and developed a four-phase (create awareness and interest, build knowledge and commitment, promote action and adoption, and pursue integration and sustained use) implementation guide for selecting the best strategies for a specific practice.
Cullen and colleagues used this tool along with the Iowa EBP Model as the foundation for an application- oriented book, Evidence-based Practice in Action: Comprehensive Strategies, Tools, and Tips from the University of Iowa Hospitals and Clinics. For each of 63 implementation strategies, the authors provide a definition, benefits, procedure, case example, and support references.
Powell and colleagues: Similar to the work led by the UIHC nursing team, Powell and colleagues used an expert panel to compile a list of 73 implementation strategies (for example, accessing funding, audit and feedback, centralizing technical assistance, developing an implementation glossary, distributing education materials, facilitating, and using advisory boards and data experts) for the mental health sector. The panel was selected based on expertise in implementation science and clinical practice, and members participated in three rounds of a survey using a Delphi process research design. The first two rounds involved a web-based survey; the third round used a web-based live polling and consensus process. Although these strategies are specific to mental health, they cross disciplines, specialties, and settings.
Li and colleagues: A systematic review by Li and colleagues focused on organizational contextual features that influence EBP implementation across healthcare settings. They reviewed and rated the quality of 36 studies published between January 2005 and June 2017. Using a standardized rating tool, they scored five studies as high quality, 22 as moderately high quality, and eight as moderate quality. Factors identified as important to implementation included organizational culture, networks and communication, leadership, resources (financial, staffing and workload, time, and education and training), evaluation, monitoring and feedback, and champions. The authors noted that leadership influences all other factors and should be a priority in implementation initiatives and that combined factors are more influential than a single factor, pointing to the importance of a multistrategy toolkit.
Take a collective approach
These combined resources provide nurses with multiple strategies to consider when embarking on EBP changes. Tucker and colleagues from the Ohio State University developed a scale that includes a list of implementation strategies clinicians can rate their confidence in using. (See EBP Implementation Strategies Self-Efficacy Scale.)
A sure path to success
Implementation is a major step in the EBP process, but it’s often underappreciated and lacks resources. Consequently, the translation of evidence into practice is slow, can’t be sustained, or doesn’t even occur. Many implementation models promote EBP, and a toolbox of strategies is your surest path to success.
Sharon Tucker is the Grayce Sills endowed professor in psychiatric–mental health nursing in the college of nursing, the translational/implementation research core director, and the Helene Fuld Health Trust National Institute for Evidence-based Practice in Nursing and Healthcare nurse scientist at the Wexner Medical Center at The Ohio State University in Columbus.
Selected References
Buckwalter KC, Cullen L, Hanrahan K, et al. Iowa model of evidence-based practice: Revisions and validation. Worldviews Evid Based Nurs. 2017;14(3):175-82.
Cullen L, Adams SL. Planning for implementation of evidence-based practice. J Nurs Adm. 2012;42(4):222-30.
Cullen L, Hanrahan K, Farrington M, DeBerg J, Kleiber C, Tucker S. Evidence-Based Practice in Action: Comprehensive Strategies, Tools, and Tips from the University of Iowa Hospitals and Clinics.Indianapolis, IN: Sigma Theta Tau International; 2018.
Damschroder LJ, Hagedorn HJ. A guiding framework and approach for implementation research in substance use disorders treatment. Psychol Addict Behav. 2011;25(2):194-205.
Glasgow RE, Vogt TM, Boles SM. Evaluating the public health impact of health promotion interventions: The RE-AIM framework. Am J Public Health. 1999;89(9):1322-7.
Grimshaw JM, Eccles MP, Lavis JN, Hill SJ, Squires JE. Knowledge translation of research findings. Implement Sci. 2012;7(1):50.
Grol R, Grimshaw J. From best evidence to best practice: Effective implementation of change in patients’ care. Lancet. 2003;362(9391):1225-30.
Li SA, Jeffs L, Barwick M, Stevens B. Organizational contextual features that influence the implementation of evidence-based practices across healthcare settings: A systematic integrative review. Syst Rev. 2018;7(1):72.
Melnyk BM, Fineout-Overholt E, Giggleman M, Choy K. A test of the ARCC©model improves implementation of evidence-based practice, healthcare culture, and patient outcomes. Worldviews Evid Based Nurs. 2017;14(1):5-9.
Melnyk BM, Gallagher-Ford L, Zellefrow C, et al. The first U.S. study on nurses’ evidence-based practice competencies indicates major deficits that threaten healthcare quality, safety, and patient outcomes. Worldviews Evid Based Nurs. 2018;15(1):16-25.
Nilsen P. Making sense of implementation theories, models and frameworks. Implement Sci. 2015;10:53.
Powell BJ, Waltz TJ, Chinman MJ, et al. A refined compilation of implementation strategies: Results from the Expert Recommendations for Implementing Change (ERIC) project. Implement Sci.2015;10:21.
Prochaska JO, DiClemente CC. The Transtheoretical Approach: Crossing Traditional Boundaries of Therapy. Krieger Publishing: Malabar, FL; 1994.
Rogers EM. Diffusion of Innovations.5th ed. New York, NJ: Simon & Schuster; 2003.
Rycroft-Malone J. The PARIHS framework—A framework for guiding the implementation of evidence-based practice. J Nurs Care Qual. 2004;19(4):297-304.
Schaffer MA, Sandau KE, Diedrick L. Evidence-based practice models for organizational change: Overview and practical applications. J Adv Nurs. 2013;69(5):1197-209.
VanLare JM, Conway PH. Value-based purchasing—National programs to move from volume to value. N Engl J Med. 2012;367(4):292-5.
ant3-CE Evidence based practice-206a


















2 Comments.
So glad to locate this article for my class I’m teaching on EBP this summer!
Excellent article on EBP implementation. Karen Breda, University of Hartford, West Hartford, CT.