Following the current guidelines helps ensure patients achieve treatment goals.
Takeaways
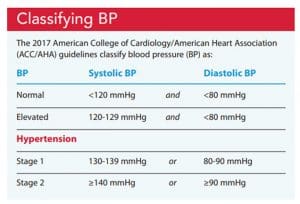
- Hypertension is defined as systolic blood pressure of ≥130 mmHg and/or diastolic blood pressure of ≥80 mmHg.
- The most common cause of error in blood pressure measurement is using the wrong cuff size, typically a cuff that’s too small.
- Home blood pressure monitoring is an essential aspect of self-care in adults with hypertension.
View and download November’s visual abstract.
According to the 2021 Heart Disease and Stroke Statistics, hypertension (HTN) affects nearly one in two (46%) adults in the United States. More men than women have HTN up until age 64, when the number of women exceeds that of men. Despite this high prevalence, only two-thirds of adults with HTN are aware of it. Of those who are aware, only 53% receive treatment. More striking is that only 25% diagnosed with HTN have their blood pressure (BP) under control (<130/80 mmHg). Control rates are lower in men than women and also in Blacks, Hispanics, and Asians (compared to Whites). These statistics are troubling because having uncontrolled HTN is a major risk factor for many cardiovascular (CV) conditions and organ damage.
To help identify those with undiagnosed HTN and to avoid complications, nurses need to understand current guidelines and treatment goals.
BP classification
The most recent American College of Cardiology/American Heart Association (ACC/AHA) clinical practice guidelines define HTN as systolic BP ≥130 mmHg or diastolic BP ≥80 mmHg. Patients are then classified as having either stage 1 or stage 2 HTN. Stage 2 usually requires medication in addition to lifestyle modifications to control BP. If the diastolic and systolic BP readings fall into different classifications, the higher classification is used. To make a clinical diagnosis of HTN, two or more BP readings obtained over two or more visits must fall into a particular classification (but not during acute illness or pain). (See Classifying BP.)
BP measurement
Accurate BP measurement is critical for diagnosing HTN and determining whether BP is controlled. Nurses can’t directly measure BP in the clinic (direct measurement requires an arterial line), so a noninvasive approach is used. Traditionally, nurses take BPs manually. However, a recent 2019 AHA scientific statement on BP measurement recommends that clinicians use an oscillometric technique with an automated (or semiautomated) BP device. The 2019 recommendations indicated that automated BPs are closer to out-of-office BP readings compared to those taken manually, making them more reflective of daily BP. Automated devices also require less time and can take multiple readings (for orthostatic BP checks or to compare measurements over time).
Error sources
Several common errors can result in inaccurate BP readings. Patient-related errors include taking a BP shortly after the patient has been eating, drinking, or smoking; when they’re moving or have a full bladder; or when they’re wearing restrictive clothing above the BP cuff. Device-related errors include using a nonvalidated BP machine (in the hospital, office, or home setting).
Procedure-related errors include placing the cuff in the wrong arm position, talking during measurement or being in a noisy location, taking repeated measurements too close together, and inaccurately documenting BP measurements. The most common source of error is using the wrong size BP cuff (miscuffing). If the cuff is too small, the BP will be falsely elevated; if it’s too large, the BP will be falsely low.
Upper arm measurements are considered the gold standard for ensuring accurate BP. The BP cuff bladder length should be 75% to 100% of the arm’s circumference and the width should be 37% to 50% of the arm’s circumference. Use a paper measuring tape to measure the arm circumference. For arms 22 to 26 cm, use a small adult size cuff. For patient’s whose arms measure 27 to 34 cm, choose an adult size cuff. Use a large adult size cuff if the arm circumference is 35 to 44 cm and an extra-large size BP cuff (adult thigh cuff) if the arm circumference is 45 to 52 cm.
If a thigh cuff is too small or doesn’t fit adequately, a wrist cuff is the best alternative. If using a wrist cuff, make sure the patient’s wrist is at heart level (mid-sternum) and the elbow is supported on a desk or table (the patient shouldn’t be holding up the arm during measurement). Finger cuffs produce falsely low BP readings and shouldn’t be used. (See How to take an accurate BP.)

Home BP monitoring
Home BP readings can better predict CV risk and organ damage compared to one-time office readings. Providers can use home BP readings for risk stratification when determining treatment goals and whether treatment should be intensified. In addition, home monitoring can help rule out white coat HTN (when clinic BP readings are higher than home readings) and masked HTN (when clinic readings are lower than home readings). Both situations are important to recognize when determining whether the patient actually has HTN and whether medications should be started or intensified.
Treatment goals
The ACC/AHA HTN clinical practice guidelines simplified how treatment goals are determined: The goal for all adults with HTN is <130/80 mm Hg. Although the goals are the same, the decision for when to start medications (added to lifestyle changes) is based on the patient’s atherosclerotic cardiovascular disease (ASCVD) risk, which can be calculated using the ACC/AHA ASCVD risk estimator plus. Patients considered at high risk for negative outcomes (myocardial infarction, stroke, death) include those with a confirmed history of CV disease (myocardial infarction, stroke, peripheral arterial disease) or with a ≥10% ten-year ASCVD risk.
When to start medications
The HTN guidelines recommend that high-risk patients should begin medications if their average BP is ≥130/80 mmHg. For lower risk patients (no history of CV disease or an ASCVD risk <10%) medications are recommended for primary prevention when their average BP is ≥140/90 mmHg.
Age-related considerations
The ACC/AHA HTN guidelines also provide age-related guidance for treatment goals. For adults age 65 years or older who live in their community and are ambulatory, treatment goals also are <130/80 mmHg. However, this goal may be too strict for adults in this age range who have multiple comorbidities or a limited life expectancy, especially if the patient, family, and provider concur that the risks of starting or intensifying medication treatment outweigh the benefits. Shared decision-making can help determine the best treatment strategy.
Lifestyle modifications
Lifestyle modifications for all patients include maintaining a healthy weight, following a heart healthy diet, reducing sodium intake, increasing potassium intake (unless contraindicated), being physically active, limiting alcohol intake, and eliminating tobacco use. Patient teaching should emphasize adopting a long-term healthy lifestyle as opposed to short-term fixes to reduce BP quickly.
Diet
The relationship between obesity and HTN is well known; as the body mass index increases so does BP. Weight loss via dietary modification and physical activity or participating in an anti-obesity treatment program can help reduce BP. A good rule of thumb for patients who are overweight or have obesity is that for every 1 kg of weight loss they can achieve a corresponding 1 mmHg reduction in systolic BP.
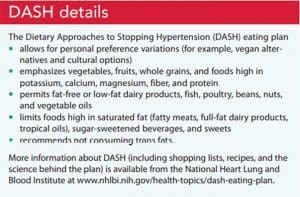
The Dietary Approaches to Stopping Hypertension (DASH) eating plan can help patients adopt a heart-healthy eating style for life. Rather than requiring special foods, it focuses on daily and weekly nutritional goals. The DASH eating plan has been shown to reduce systolic BP in those with HTN by as much as 8 to 14 mmHg (equivalent to a low or moderate dose of an antihypertensive agent). (See DASH details.)
Because reducing sodium intake has been shown to reduce systolic BP by 2 to 8 mmHg, the AHA recommends that adults should ingest no more than 2,300 mg of sodium each day. For patients with elevated BP or HTN, the recommendation is 1,500 mg per day. These recommendations can be challenging for Americans, many of whom ingest about 3,500 mg of sodium every day.
Many patients think that sodium reduction means removing salt from the dinner table or not using it in meal preparation. These strategies are helpful, but most of the sodium in the American diet comes from processed (canned and packaged) foods. Teach patients how to read labels and to choose foods with <300 mg of sodium per serving. Even if a patient can’t reach a goal of <1,500 mg of sodium per day, cutting back by 1,000 mg per day from their current level can improve BP and heart health.
Combining the DASH eating plan with decreased sodium intake results in the greatest BP reduction. For example, following DASH and ingesting 1,150 mg of sodium per day has been shown to reduce systolic BP up to 20 mmHg. According to research by Jurascheck and colleagues, patients who follow DASH and ingest 2,300 mg of sodium each day can reduce their systolic BP by 10 mmHg.
Physical activity
Increasing physical activity has been shown to reduce systolic BP as much as 4 to 9 mmHg. World Health Organization (WHO) physical activity recommendations include engaging in 150 to 300 minutes of moderate-intensity aerobic physical activity per week. This equates to walking at a brisk pace (4 miles/hour) an average of 30 minutes per day for five days each week. Alternatively, adults (as able) can engage in 75 to 100 minutes of vigorous intensity aerobic activity (for example, jogging 6 miles/hour) each week. The WHO recommendations also call for muscle-strengthening activities that involve all major muscle groups for 2 or more days each week. Patients who don’t currently meet the WHO recommendations should start with small amounts of activity (in duration, frequency, and intensity). As with other life style modifications, engaging in some physical activity is better than none.
Alcohol
Drinking alcohol can increase BP. Current recommendations for patients with elevated BP or HTN include limiting alcohol intake to no more than one serving per day for women and no more than two for men. A standard serving may include 5 ounces of wine, 12 ounces of beer, 8 ounces of malt liquor/IPA beer, or 1.5 ounces of whiskey (or equivalent). Remind patients that this doesn’t mean they can ingest 7 days’ worth of servings in one 24-hour period. Following these recommendations can reduce systolic BP by as much as 3 to 4 mmHg.
Tobacco
Smoking tobacco acutely increases BP for about 30 minutes after each cigarette. Over time, chronic cigarette use increases arterial stiffness, which increases HTN, myocardial infarction, stroke, and peripheral arterial disease risk. Complete cessation of cigarette smoking is recommended. If cessation isn’t possible, any reduction is better than none.
Pharmacologic management
According to the ACC/AHA HTN treatment recommendations, four main medication classes may be used as first-line pharmacologic therapy: angiotensin converting enzyme (ACE) inhibitors, angiotensin receptor blockers (ARBs), calcium channel blockers (CCBs), and diuretics. The prescribed medication class will depend on the patient’s comorbidities, allergies and intolerances, and patient preferences.
Beta-blockers are not considered first-line HTN medications. However, if a patient has other conditions (such as chronic heart failure, coronary artery disease, or atrial fibrillation), they may benefit from a beta-blocker for HTN and the comorbid condition. For example, carvedilol or metoprolol tartrate might be prescribed if the patient has chronic heart failure with reduced ejection fraction. Not all beta-blockers have the same mechanism of action. For example, carvedilol has alpha-1, beta-1, and beta-2 blocking activities, but metoprolol, a cardio-selective beta-blocker, can be used if the patient has reactive airway disease (as long as they don’t use daily beta-agonist inhalers).
ACE inhibitors and ARBs
Renin angiotensin aldosterone system (RAAS) blockers, such as ACE inhibitors and ARBs, commonly are used for patients with comorbid diabetes and kidney dysfunction. Some patients may experience a transient increase in their potassium, blood urea nitrogen, and creatinine levels after starting or increasing RAAS blockers; however, these medications protect the kidneys in the long-term. If potassium levels remain within normal limits and creatinine doesn’t increase more than 30%, most patients can tolerate the transient increase.
ACE inhibitors and ARBs should not be used together. Dual RAAS blockade can result in markedly worse kidney function or hyperkalemia, especially in patients with chronic kidney disease or in those taking supplemental potassium or potassium-sparing diuretics.
CCBs
CCBs, in addition to effectively reducing BP, also are effective anti-anginal agents in patients with coronary artery disease. Within this class of medications are two sub-classes: dihydropyridines (such as amlodipine) and non-dihydropyridines (such as diltiazem and verapamil). Most dihydropyridines are prescribed once daily and are well tolerated, but they may be associated with pedal edema. Decreasing the dose may reduce this side effect without reducing the medication’s BP lowering action.
Non-dihydropyridines lower heart rate, which is helpful in patients with atrial fibrillation or other arrhythmias that cause tachycardia or palpitations. However, these medications are not recommended for patients with bradycardia or advanced heart block. Both CCB subclasses are negative inotropes (especially non-dihydropyridines), so they shouldn’t be prescribed to patients with heart failure.
Diuretics
Providers usually start with thiazide (or thiazide-like) diuretics to treat HTN. If the patient has moderate to severe chronic kidney disease with an estimated glomerular filtration rate <30, a loop diuretic will be prescribed because these agents work higher up on the nephron. Even if a patient isn’t experiencing edema, a diuretic may be required to reduce circulatory blood volume and lower BP.
A common side effect of diuretics is electrolyte imbalance (such as hypokalemia and hyponatremia). However, because many patients with HTN ultimately need three to four medications, some side effects may offset others. For example, patients on a RAAS blocker and a thiazide or loop diuretic may have normal potassium levels.
Encouraging self-care
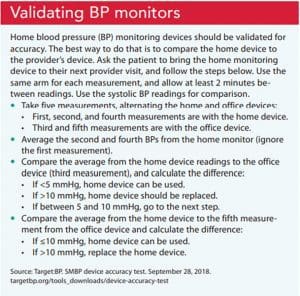
Home BP monitoring allows patients to be more engaged in their healthcare, which frequently increases treatment adherence. To implement home BP monitoring, ensure the patient has a validated monitor and uses the correct size BP cuff. (See Validating BP monitors.)
Based on the AHA/American Medical Association 2020 self-measured BP monitoring at home joint policy statement, patients should take their BP at least twice in the morning and twice in the evening (each reading separated by 1 to 2 minutes) for a week, to obtain 28 or more readings, ideally over 7 days (minimally, 12 total readings over 3 days). Patients can submit their findings to their provider via their patient portal or bring a copy of the recordings to each clinic visit. Providers typically discard the first day’s readings for patients newly implementing home monitoring because the readings tend to be falsely elevated until the patient becomes comfortable with home monitoring. On average, home BP readings will be 5 mmHg lower than clinic readings. If most of the remaining readings are above the desired target, the provider may consider intensifying medications and lifestyle modifications. After the BP is controlled, patients should continue home monitoring a few times a week to note whether BPs remain at or below goal. In the week before the next clinic visit, they should obtain daily readings for a week as they did initially.
Share the information
Nurses should take the opportunity to educate their colleagues about the BP classifications. Nurses also can partner with patients and their families to provide information about maintaining a heart-healthy lifestyle, adhering to their pharmacologic treatment, implementing home BP monitoring, and validating the accuracy of their BP monitors.
Leslie L. Davis is an associate professor in the school of nursing, PhD division, at the University of North Carolina at Chapel Hill.
References
Bull FC, Al-Ansari SS, Biddle S, et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br J Sports Med. 2020;54(24):1451-62. doi:10.1136/bjsports-2020-102955
Juraschek SP, Miller ER 3rd, Weaver CM, Appel LJ. Effects of sodium reduction and the DASH diet in relation to baseline blood pressure. J Am Coll Cardiol. 2017;70(23):2841-8. doi: 10.1016/j.jacc.2017.10.011
Muntner P, Shimbo D, Carey RM, et al. Measurement of blood pressure in humans: A scientific statement from the American Heart Association. Hypertension. 2019;73(5):e35-66. doi: 10.1161/HYP.0000000000000087
Shimbo D, Artinian NT, Basile JN, et al. Self-measured blood pressure monitoring at home: A joint policy statement from the American Heart Association and American Medical Association. Circulation. 2020;142(4):e42-63. doi: 10.1161/CIR.0000000000000803.
Virani SS, Alonso A, Aparicio HJ, et al. Heart disease and stroke statistics—2021 Update: A report from the American Heart Association. Circulation. 2021;143(8):e254-743. doi: 10.1161/CIR.0000000000000950
Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: A report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines. Hypertension. 2018;71(6):e13-115. doi: 10.1161/HYP.0000000000000065