Astute triage and evaluation prompt fast action.
- Herpes zoster ophthalmicus occurs as a result of reactivation of the varicella-zoster virus. Without prompt identification and ophthalmology evaluation, permanent vision loss may occur.
Caroline Carey*, a 62-year-old woman recently diagnosed with non-small cell lung cancer, arrives at the emergency department (ED) with fatigue, facial pain, and a rash on the left side of her face. Since her cancer diagnosis, she’s received 10 cycles of chemotherapy. Her last dose was 4 days ago. Ms. Carey knows that as a result of her diagnosis and treatment she’s immunocompromised and susceptible to infection. The ED has a 5-hour wait.
History and assessment
During triage, Ms. Carey tells Mary, the ED nurse, that she’s had increasing fatigue for the past 2 weeks. Five days ago, she developed a sharp, stabbing pain along the left side of her face. The pain has been consistent (10/10) and unresponsive to over-the-counter acetaminophen and ibuprofen. She also reports a “red rash” on the left side of her face that has worsened.
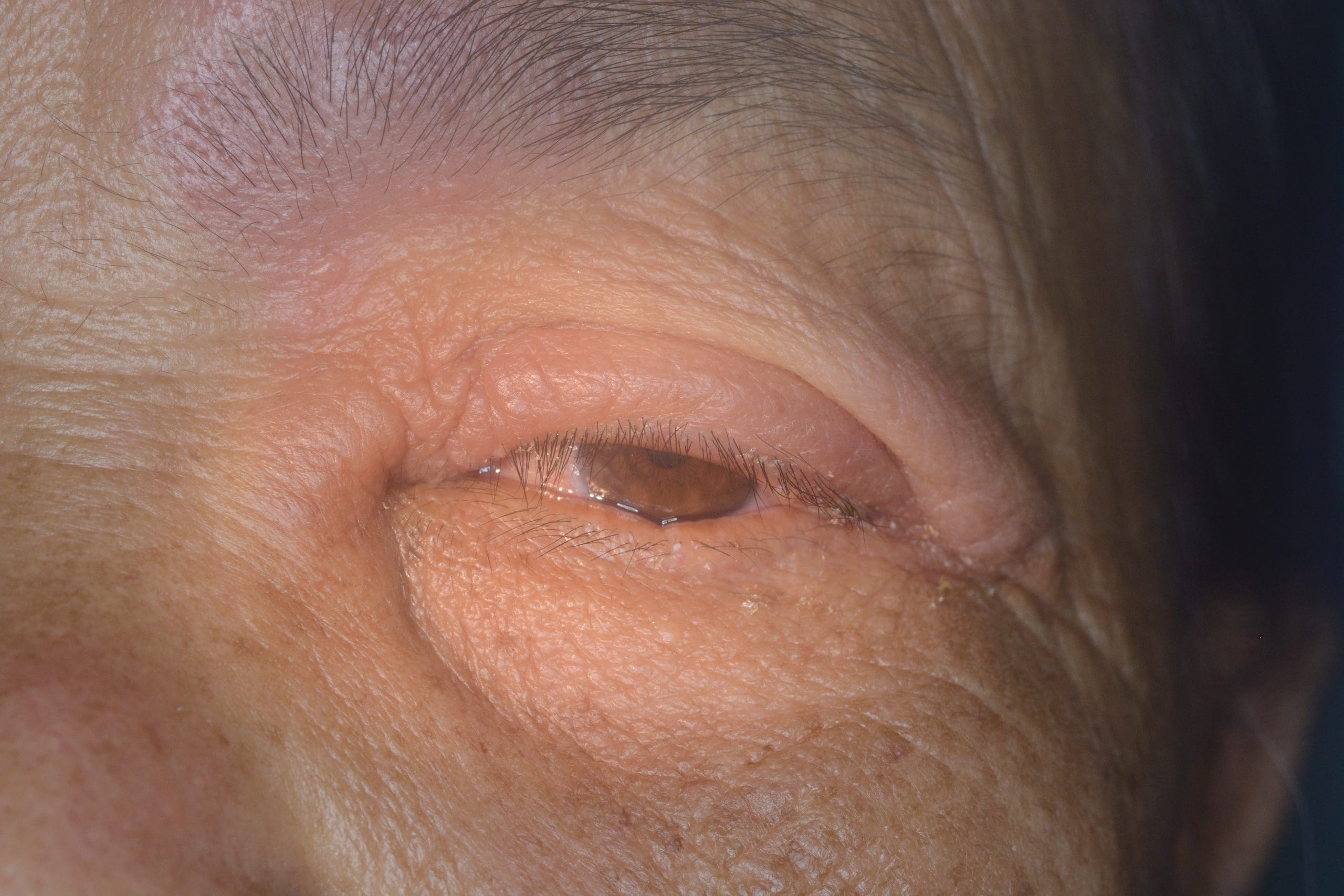
Ms. Carey’s vital signs are stable: temperature 98° F (36.6° C), HR 66 bpm, RR 20 breaths per minute, BP 112/64 mmHg, and O2 saturation 95% on room air. Mary notes that the facial rash doesn’t cross the midline and identifies several grouped vesicles on the nose and around the left eye. She bypasses the waiting room, and takes Ms. Carey directly to the treatment area.
Taking action
Mary assesses Ms. Carey’s visual acuity (left eye 20/40, right eye 20/30, and both eyes 20/30) and immediately notifies the ED physician about her concern for herpes zoster ophthalmicus (shingles). The physician assesses Ms. Carey and notes a positive Hutchinson’s sign with vesicular lesions on the tip and side of the nose, which indicates trigeminal nerve involvement. Ophthalmology is consulted and antiviral therapy initiated with I.V. acyclovir 10 mg/kg every 8 hours.
Outcome
Ms. Carey is admitted to the medical–surgical unit and placed on airborne, contact isolation. The ophthalmology team performs a slit-lamp examination of the anterior segment and fluorescein staining. They don’t identify corneal or anterior chamber abnormalities. Ms. Carey’s treatment with I.V. acyclovir continues for 7 days, after which she’s discharged home with close primary care, oncology, and ophthalmology follow up.
Education and follow-up
Herpes zoster ophthalmicus occurs as a result of reactivation of the varicella-zoster virus. Patients at highest risk include adults over the age of 60, women, and those with immunosuppression. Ophthalmic manifestations of herpes zoster infection may present with headache, fatigue, unilateral facial pain, and fever. A 2- to 3-day prodromal phase precedes vesicular eruptions. Diagnosis is primarily clinical.
Approximately 85% of herpes zoster infection ophthalmic cases have ocular involvement and 10% have permanent vision loss due to corneal scarring, which makes prompt identification and ophthalmology evaluation critical. Treatment with I.V. acyclovir remains the mainstay for patients who are immunocompromised; others can receive oral and topical antivirals. Common side effects of acyclovir include nausea, vomiting, diarrhea, headaches, and dizziness. The CDC recommends two doses of herpes zoster vaccination 2 to 6 months apart for healthy adults over age 50 and for immunocompromised adults over age 19.
In Ms. Carey’s case, Mary’s astute triage assessment facilitated timely implementation of an evidence-based treatment plan.
*Name is fictitious.
Aaron M. Sebach is dean of the College of Health Professions and Natural Sciences, Wilmington University, in New Castle, Delaware, and a mobile integrated health nurse practitioner at TidalHealth Peninsula Regional in Salisbury, Maryland.
American Nurse Journal. 2023; 18(7). Doi: 10.51256/ANJ072318
References
Anderson TC, Masters NB, Guo A, et al. Use of recombinant zoster vaccine in immunocompromised adults aged 19 years: Recommendations of the Advisory Committee on Immunization Practices – United States, 2022. MMWR Morb Mortal Wkly Rep. 2022;71(3):80-4. doi:10.15585/mmwr.mm7103a2
Cason JB. Herpes zoster opthalmicus. EyeWiki. 2022. eyewiki.aao.org/Herpes_Zoster_Ophthalmicus
Centers for Disease Control and Prevention. Shingrix recommendations. January 24, 2022. cdc.gov/vaccines/vpd/shingles/hcp/shingrix/recommendations.html
Key words: herpes zoster ophthalmicus, shingles, trigeminal nerve, varicella-zoster virus



















1 Comment. Leave new
thanks for info.