

Translating scarce resource management into outcomes with impact.
Takeaways:
- The more resource options available for day-to-day surge events, the more effectively hospital operations can withstand imbalances in supply and demand.
- Proactively addressing the financial impact of surge frequently isn’t considered a priority in preparedness efforts, but it’s essential for an organization’s sustainability.
- Maintaining the usual or functionally equivalent standard of patient care through the judicious and ethical allocation of scarce resources is the overarching goal of surge planning.
CNE 3.0 contact Hours
Learning Objectives
- State the importance of comprehensive surge planning.
- Describe a scarce resource management model.
- Discuss the role of nurse leaders in scarce resource management.
The author and planners of this CNE activity have disclosed no relevant financial relationships with any commercial companies pertaining to this activity. See the last page of the article to learn how to earn CNE credit.
Expiration: 11/1/23
To earn contact hour credit online, please visit the ANA website for more information on purchasing this course.
What if your hospital had to respond to a surge of 300 patients from a mass casualty incident in the next 45 minutes? What if 50 patients arrived at your critical access emergency department (ED) within 15 minutes? What if you had to staff a 150% increase in capacity to care for a surge of COVID-19 patients?
Planning for medical surge events—large or small, sudden or insidious—is complex and multi-faceted. It’s not an exact science, and more research is needed to expand our knowledge. Planners rely heavily on lessons learned from first-hand hospital experiences around the world. One of the most difficult challenges is anticipating and mitigating the potential disasters within a disaster—“surprise” circumstances inherent to both human-made and natural events. Lack of situational awareness and unintentional planning oversights can create additional chaos during the response to a crisis and hinder an organization’s ability to recover. Fortunately, many “surprises” are predictable and can be managed with preparation.
Comprehensive surge planning requires a high level of continuous readiness to achieve successful outcomes when an incident occurs. It also requires strong leadership commitment and a highly skilled team of dedicated clinical and technical subject matter experts who collaborate with community healthcare partners to plan and manage the balance between resource availability and service demand.
Hospital leaders have a moral obligation to reduce patient, staff, provider, and facility vulnerabilities. Fostering resilience to disaster situations starts with a data-driven scarce resource management model centered on the organization’s values and mission. Implementing this approach requires additional planning time and resources, but it may spare precious assets, reduce risks, and potentially save lives. Nurse leaders can serve as key influencers for ensuring successful scarce resource management.
Download a visual abstract of this continuing nursing education article to share on social media, here. Be sure to tag us on Twitter, Facebook, and Instagram!
Traditional surge planning
By 2009, mass casualty incidents were escalating around the world. In 2004, a bombing in Madrid, Spain, sent 312 injured patients to a single community hospital in less than 3 hours. The World Trade Center had been attacked in 2001. The 2009 H1N1 pandemic was on the horizon. In response to these real and emerging threats, the Office of the Assistant Secretary for Preparedness at the U.S. Department of Health and Human Services charged the Institute of Medicine (IOM; now the National Academy of Medicine) with identifying steps for the fair delivery of medical services when demand puts stress on an organization’s ability to provide the usual level of care. In 2009, the IOM issued Guidance for Establishing Crisis Standards of Care for Use in Disaster Situations: A Letter Report. A more thorough review of the theories of crisis standards of care (CSC) was published in 2012. Both documents have served as the foundation for hospital surge planning for over a decade. Although some concepts have evolved, the key principles of CSC remain the same—fairness, duty to care, duty to steward resources, transparency, consistency, proportionality, and accountability.
According to medical surge experts John Hick, MD, and Dan Hanfling, MD, CSC can be reduced to four basic elements: a planning framework based on strong ethical principles, the rule of law, provider and community engagement, and the duty to plan. When hospitals fail to adequately plan for scarce resource allocation, they can force healthcare providers to make inferior choices that lead to ethical and legal entanglements, unnecessary triage decisions, loss of public trust, and additional human suffering and death. These situations represent their own potential disasters, as we witnessed after hurricanes Katrina and Maria and other recent events.
Scarce resource management model
Converting from traditional surge planning to a scarce resource management model involves more than expanding a hospital’s capacity and capabilities. It requires a paradigm shift that prioritizes preparedness as a tenet of the organization’s mission. The COVID-19 pandemic, natural disasters, and mass casualty incidents in the United States and around the world clearly demonstrate the need for every hospital, large and small, to be disaster-ready.
Here are seven ways nurse leaders can contribute to this effort. Each includes questions that will help leaders in their journey from a reactive to a proactive approach.
1. Advocate for a culture of readiness Nurse leaders are in a strong position to advocate for a preparedness model that goes beyond policies, procedures, and regulatory compliance. A sustainable change in mindset regarding emergency preparedness requires that every person in the organization recognize how their role fits into the bigger picture. Grassroots input for workable solutions is crucial because then everyone owns a piece of the planning and response puzzle.
Here’s an example to illustrate this point. One nurse is primarily responsible for emergency preparedness in a small, suburban hospital. He’s very knowledgeable of the components of disaster management. Over his long tenure, he’s compiled a thick manual of policies and procedures that meet regulatory requirements. But when the chief executive officer (CEO) and service-line managers gather to discuss and respond to questions about the organization’s key response capabilities, all eyes turn to this one nurse, who is charged with maintaining the operations manual. He’s viewed as the person with the answers. The managers are overconfident in the hospital’s ability to respond effectively to any disaster situation because the preparedness person will be there to direct their actions.
In what ways can you engage managers and staff to actively contribute to the planning efforts in your organization? How would you encourage those entrusted with the preparedness role to share ownership of the planning process?
2. Urge executive endorsement of a continuous preparedness business model No matter the type or scope of an emergency, the CEO has the ultimate authority, accountability, and moral imperative for providing leadership and support for all aspects of disaster management. It’s the role of C-suite administrators to maintain awareness of emerging threats to the organization and the healthcare community, prioritize attention to those events, and mobilize appropriate assets to address them. Unfortunately, the responsibility of preparedness activities too often is delegated to a single person or a committee with limited time, resources, or decision-making authority and without a direct reporting link to the top of the organization.
In annual surveys conducted between 2016 and 2019 by The American College of Healthcare Executives, hospital CEOs consistently identified financial challenges as their number one concern. Less than 1% of respondents identified emergency preparedness as a major issue. Budgetary pressures, shrinking revenue margins, lack of funding to invest in stockpiling resources, competition from myriad burning platforms, and the false hope that “it won’t happen here” contribute to the low priority given to disaster readiness. In actuality, effective scarce resource management and financial management are inextricably linked. Both are critical for successful response and recovery.
COVID-19 has changed the preparedness landscape. The sourcing and allocation of critical resources is on the mind of every hospital CEO in the country. Experts have indicated that major disasters function as focusing events and reveal gaps in planning and response, but the middle of a pandemic isn’t the time to pursue major operational changes. Nurse leaders can serve as catalysts and encourage C-suite administrators (many of whom are nurses) to participate in interdisciplinary discussions addressing the challenges of preparing for future crises.
How can you, as a nursing leader, best leverage the COVID-19 crisis to facilitate change in your organization and in your professional relationships with peers in your community? Which benefits of a culture of preparedness would you include in talking points with the administration?
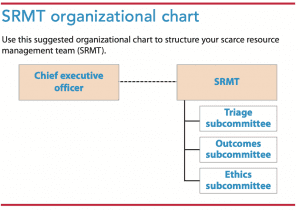 3. Promote the formation of a scarce resource management team. The concept of a scare resource management team (SRMT) is based on an operational business model for proactive resource planning and data-driven decision criteria for responding to and recovering from medical surge events. An early prototype of the concept was proposed by an Ohio Hospital Association task force as part of its CSC planning. Resource sparing strategies are based in part on a financial risk analysis directed toward high-priority outcomes vs. specific events. The team is charged by the CEO with coordinating and overseeing the entire resource management program. (See SRMT organizational chart.)
3. Promote the formation of a scarce resource management team. The concept of a scare resource management team (SRMT) is based on an operational business model for proactive resource planning and data-driven decision criteria for responding to and recovering from medical surge events. An early prototype of the concept was proposed by an Ohio Hospital Association task force as part of its CSC planning. Resource sparing strategies are based in part on a financial risk analysis directed toward high-priority outcomes vs. specific events. The team is charged by the CEO with coordinating and overseeing the entire resource management program. (See SRMT organizational chart.)
Maintaining the usual or functionally equivalent standard of care through the judicious and ethical allocation of scarce resources is the SRMT’s overarching goal. This includes establishing benchmarks for surge responses, alternative strategies for resource consumption, and oversight of applicable operational policies and protections for staff and healthcare providers. During an event, the team’s role is to assess and analyze real-time data, adapt resource strategies, and advise hospital incident command. Data can be aggregated with regional statistics for community resource planning and mitigation efforts.
Many hospitals have a safety or emergency preparedness committee that fulfills some of the SRMT functions. However, the frequency, type, and scope of current real and emerging threats require emphasizing on-going situational surveillance, data analytics, supply chain management, and logistical collaboration with community partners. This creates demand for a broader base of subject matter expertise, a wider scope of independent decision-making capability, and a higher degree of accountability of the committee to the administration. Expanding an existing hospital or system committee is one way to establish a more comprehensive, effective resource management program. (See Who’s on the team?)
What are the advantages and challenges of converting to an SRMT in your hospital? What other subject matter experts would you add to the recommended composition of the SRMT?
4. Consider outcomes-based vulnerability analysis as a planning tool. Every hospital in the 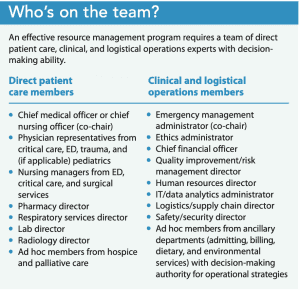 United States is required to conduct a hazard vulnerability analysis (HVA) and review it annually. The HVA is a systematic process for identifying an organization’s highest risk to certain natural and man-made events. An HVA can be conducted in a number of ways, but Kaiser Permanente has the most widely used assessment tool, which can be downloaded here.
United States is required to conduct a hazard vulnerability analysis (HVA) and review it annually. The HVA is a systematic process for identifying an organization’s highest risk to certain natural and man-made events. An HVA can be conducted in a number of ways, but Kaiser Permanente has the most widely used assessment tool, which can be downloaded here.
Unfortunately, the results of this analysis are unlikely to change from year to year (for instance, your organization’s vulnerability to a hurricane will remain the same), so completing it can become a routine exercise with minimal scrutiny.
To gain greater insight with more meaningful results, organizations should consider completing an outcomes-vulnerability analysis (OVA) as an adjunct to their HVA. The OVA correlates resource needs with categories of actionable outcomes of events (supply chain disruption, evacuation or shelter in place, security issues, staffing shortages, and financial impact to name a few). This analysis further delineates the human, business, and property impacts of high-risk events. It’s a simple method for judiciously prioritizing time and resource dollars required for planning across multiple incidents with similar vulnerabilities.
Here’s an example: A hospital on the Gulf coast identifies hurricanes and floods as high-risk hazards according to their HVA. High-impact outcomes on the OVA identify security issues, the need to evacuate or shelter-in-place, staffing concerns, supply shortages, structural damage, and financial impacts as potential vulnerabilities. The same hospital also identifies civil disruption has a high-risk hazard, and the OVA demonstrates very similar outcome vulnerabilities—even though the two events are quite different in nature. Thus, the SRMT can plan against and mitigate these outcomes in broad terms, creating a truly all-hazards approach for resource management as required by regulators and payers.
Addressing financial impact typically isn’t identified as a priority in preparedness efforts, but it’s essential for an organization’s sustainability. Every surge event has accompanying financial issues. Some of the predictable surprises of surge situations include considering shutting down outpatient services or elective surgeries, factoring in staff overtime or the need for furloughs, capturing charges in the midst of chaos for billing and Federal Emergency Management Agency reimbursement, the potential for legal liabilities, and fall-out from public relations disasters. It is imperative that a finance decision-maker is part of the SMRT.
How could you incorporate OVA data into the surge planning process for your area of responsibility?
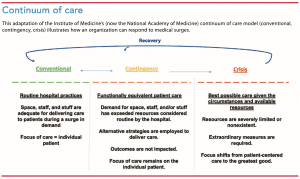
5. Embrace a conventional, contingency, and crisis continuum-of-care model. The IOM continuum-of-care model provides a visual guide for resource management during medical surge events. Historically, space, staff, and stuff have been the focus of resource planning along this continuum. Recently, “systems” has been added, representing a major shift toward community involvement and healthcare coalition participation. (See Continuum of care.)
Although “crisis standards of care planning” is the traditional terminology, the end goal is to never get to crisis mode. Most hospitals face fluctuating surges in demand every day, and EDs routinely function beyond capacity. Temporary adaptations usually allow standard protocols to remain intact. Consequently, preparedness activities bolster what’s considered customary and integrate the new normal into the fabric of daily operations. This makes for a more resilient organization when an event does occur. No bright line exists between each level of care; some resources may remain consistent with daily practice while scarcity of others may require contingency or crisis strategies.
If a hospital shifts to contingency plans, some practice standards change, but patient care remains functionally equivalent. I use the “salt and soda” analogy. If we ran out of toothpaste when I was young, my mother would make a baking soda and salt mixture for us to use until our “stock” was replenished. We hated it. It tasted awful and left grit in our mouths, but the outcome was the same whether we used salt and soda or toothpaste. Our teeth were clean. This is contingency planning in a nutshell—having alternatives to substitute for scarce resources until returning to a conventional standard of care.
In crisis mode, substantial changes occur in the way care is provided with potential implications for patient outcomes. Crisis mode also may lead to devastating effects on staff members’ physical and emotional health. We’ve seen this with COVID-19 and scarce personal protective equipment (PPE). Resources may eventually become so scarce that life-saving treatment must be withheld or withdrawn from selected patients and allocated to others who are deemed more likely to survive. This is the definitive meaning of crisis standards of care.
Remember that “catastrophe” and “crisis” aren’t synonymous. A hospital may experience a catastrophic event but remain in conventional mode if its resource capacity and capability can accommodate a large patient surge. Conversely, if resource planning efforts are inadequate at a local, regional, or national level, even a small event can turn into a crisis.
Alternative resource strategies. The more resource options available for day-to-day surge events, the more effectively hospital operations can withstand sudden or prolonged imbalances in supply and demand. The Minnesota Department of Health has developed a set of informational cards that serve as a planning guide for hospitals to assess alternative resource strategies for substitution, adaptation, conservation, reuse, and reallocation across the continuum. This guidance is particularly helpful for nurse managers when considering staffing plans for each level of care.
What is the conventional surge capacity in your department or unit? What alternative resource strategies have been identified specific for your area of responsibility to provide functionally equivalent patient care if usual resources are exhausted?
6. Contribute to planning metrics. Comprehensive resource management along the continuum isn’t possible without first recognizing the components of daily care delivery. These components are the hospital’s key response capabilities. Nurse leaders are essential to collecting accurate data from their areas of responsibility and assisting the SRMT in interpreting the metrics to establish baseline measures for conventional surge levels. Knowing these metrics enables organizations to more effectively scale up when a surge occurs. Nurses also play a vital role in collaborative planning with leaders from other departments to facilitate efficient patient movement to the most definitive level of care during a surge.
What are the metrics for daily through-put for ED admissions to the units or to OR for emergent surgery? How long does it take to get patients through radiology or get routine lab results on a busy day? How does timing vary during off-shifts, weekends, and holidays? What are the benchmarks for secondary and tertiary triage, ED trauma care, and a discharge surge from the units or ICU? Have expedited processes in nonclinical departments (such as registration, billing, and environmental services) been assessed and measured? Could daily bottlenecks become a secondary disaster in a crisis?
Indicators and triggers. Predefined indicators and triggers must be established for each level on the continuum of care to determine data-driven resource thresholds. In other words, how does an organization know when it’s time to make a change in operations? Triggers should stretch the perception of a hospital’s capacity and ability to manage conventional and contingency surge levels.
Nursing leaders and administrators must be aware, in absolute terms, when the situation necessitates a move along the continuum. This could mean expanding care into nontraditional spaces, adapting staffing plans, or opening an alternate care site. The SRMT and hospital incident command will rely on this information to make prudent decisions.
As we’ve seen during the COVID-19 pandemic, being able to analyze the burn rate for scarce resources, such as PPE, also is critical. The Centers for Disease Control and Prevention has developed a predictive model to help health systems estimate demand for medical and ICU beds, ventilators, PPE, medications, and available staff 1 to 30 days in advance on a rolling basis (that is, calculated daily).
Metrics also provide a transparent way to share information with community partners for leveraging resources and sharing patient load. The availability of improved communication technology and data analytics for real-time decision-making is revolutionizing response capabilities and situational awareness within healthcare communities.
Are you aware of the metrics that signal an operational change from conventional to contingency care or contingency to crisis care is imminent? Which metrics would be most important for you to measure for your area of responsibility?
7. Oversee development of realistic, values-based reciprocal obligations. Staff is the most critical resource in any surge event. Listening, hearing, caring, and supporting staff are as vital to positive patient outcomes as any other step in the scarce resource management process.
Reciprocal obligations fall into two categories: duty of care and institutional obligations.
Duty of care. Thoughtful conversations must take place among leaders, clinical personnel, and physicians to discuss what they perceive as limits to their duty to provide care and do no harm under fluctuating and adverse conditions. This is particularly important when catastrophic situations have the potential for greater personal and professional risk, moral distress, and dual obligations to work and family. Openly addressing these conflicts lays the foundation for assumption-based staffing plans, provides a respectful way to give voice to staff and provider concerns, and serves as the basis for operational and educational policies that balance organizational and staff needs.
In what ways can nurse leaders create a safe and trusting environment for crucial conversations with clinical staff and medical providers? What questions would you pose to elicit honest, open responses? How would you incorporate staff fears and concerns into actions and policy?
Institutional obligations. Every hospital must address its obligations to staff and providers through pre-planned strategies that recognize threats to their physical and psychological health and occupational safety. The ability of nurses and clinicians to make reasoned decisions in austere conditions is crucial. The adverse impact of emotional and physical stress on decision-making capabilities is well documented in the literature.
Not only front-line caregivers become deeply affected by their roles in a crisis. The staff members who clean the bloody floors in the ED during a mass casualty incident can be just as traumatized as the trauma team. The same can be said for anyone working in an overburdened ICU or COVID-19 unit. Policies and procedures must be developed to protect staff. But more important, the leaders’ actions must reflect that they care, support, and appreciate workers.
Communicate. In June 2020, The American Organization of Nurse Leadership presented a webinar on the challenges of leading during the COVID-19 pandemic. Presenters David Bailey, PhD, RN, chief nursing officer at UCLA Health, and Sylvain Trepanier, DNP, RN, chief clinical executive officer at St. Joseph Health, emphasized the importance of consistent, timely, and transparent communication. Bailey noted, “Staff and physicians are panicked over the unknowns of the virus and expectations to provide care with limited PPE.” Bailey also stressed how important it is that the organization’s mission serves as the north star for ethical decision-making and development of processes that are fair and respectful to patients, staff, providers, and community partners.
Share patient volume data, supply availability, and alternative resource strategies daily with all staff, either verbally, by email, or via an alert system. Establish a method for staff to communicate their concerns. Keeping people in the dark or ignoring their fears adds to stress and disillusionment—even anger. An exhausted, frightened staff that feels angry and unappreciated is an unnecessary disaster waiting to happen.
Train and exercise. An organization is morally obligated to ensure that its workforce is trained and knowledgeable. Maintaining competency levels that promote safe practices is time-consuming and expensive, but it’s part of a CEO’s commitment to a culture of readiness. Just-in-time training is necessary under certain circumstances, but disaster situations aren’t the best time for people to do something for the first time. This includes administrators who might serve in hospital incident command roles during an event. Disaster preparedness must go beyond a quick mention in an already packed orientation schedule or an annual review to meet regulations.
Most hospitals haven’t had their surge plans tested by real-life circumstances. Opportunities to participate in crisis-level exercises that stress the entire organization in worst-case scenarios must be part of continuous readiness. Nursing leaders should advocate for exercises that stress the limits of the organization to the point of failure. This provides the most fertile ground for reassessing planning metrics, processes, and competencies. Trepanier and Bailey note that organizations can’t push the envelope far enough and should consider what plans would look like at 50%, 130%, or 150% of capacity. The lesson learned in their California hot spot hospitals is to go extreme and always ask “What if?”
Turn disaster into manageable chaos
Let’s go back to the beginning and our “what if” questions. How would you handle a sudden surge?
- Three hundred patients from a mass casualty incident in the next 45 minutes? Citizen-transporters take as many as 80% of victims to the ED in their truck beds and cars. They don’t know if your hospital has a trauma designation; they only know it’s the closest one to the scene.
- Fifteen minutes till 50 patients? A critical access hospital may be the only option in the county, and good Samaritans will be carrying victims to you as well.
- A 150% increase in capacity? Hospitals have become adept at increasing their space, but a corresponding increase in staff is so difficult that it’s frequently set aside until a real event occurs.
Usually, scenarios such as these are so beyond what’s normal that we automatically say, “No way.” But U.S. hospitals have experienced (or are experiencing) these very situations. The answer has to be “Yes, we can.” We really have no choice. Strategic scarce resource management combined with administration commitment, a strong team of experts, well-informed staff who are passionate about their work, and nurse leaders who are dedicated to the highest-quality patient care under any circumstances make all the difference. Anticipating predictable surprises under the umbrella of a culture of readiness can turn a disaster into manageable chaos with positive patient outcomes.
For an example of use of the OVA tool, click here.
Jacklyn Shaffer is president of CommonGround Partners in Dublin, Ohio. She’s consulted with many healthcare and public health organizations on medical surge and scarce resource management.
References
California Department of Public Health. 15 ‘til 50—Mass casualty incident toolkit. cdphready.org/15-til-50-mass-casualty-incident-toolkit-multimedia.
Centers for Disease Control and Prevention. Optimizing supply of PPE and equipment during shortages. July 16, 2020. cdc.gov/coronavirus/2019-ncov/hcp/ppe-strategy/index.html
Centers for Disease Control and Prevention. Personal protective equipment (PPE) burn rate calculator. April 7, 2020. cdc.gov/coronavirus/2019-ncov/hcp/ppe-strategy/burn-calculator.html
Einav S, Hick JL, Hanfling D, et al. Surge capacity logistics: Care of the critically ill and injured during pandemics and disasters: CHEST consensus statement. Chest. 2014;146(4 suppl):e17S-43S.
Healthcare Emergency Preparedness Gateway. Topic collection, crisis standards of care. asprtracie.hhs.gov/technical-resources/63/crisis-standards-of-care/0
Healthcare Financial Management Association. Disaster Planning Checklist for Chief Financial Officers of Healthcare Organizations. hfma.org/content/dam/hfma/Documents/industry-initiatives/disaster-checklist-healthcare-organizations.pdf
Hick JL, Hanfling D, Wynia MK, Pavia AT. Duty to plan: Health care, crisis standards of care, and novel coronavirus SARS-CoV-2. National Academy of Medicine. March 5, 2020. nam.edu/duty-to-plan-health-care-crisis-standards-of-care-and-novel-coronavirus-sars-cov-2
Institute of Medicine. Guidance for establishing crisis standards of care for use in disaster situations: A letter report. Washington, DC: The National Academies Press; 2009. ncbi.nlm.nih.gov/books/NBK219958
Institute of Medicine. Crisis standards of care: A systems framework for catastrophic disaster response: Volume 1: Introduction and CSC framework. Washington, DC: The National Academy. 2012. nap.edu/catalog/13351/crisis-standards-of-care-a-systems-framework-for-catastrophic-disaster
Minnesota Health Care Preparedness Program. Patient care strategies for scarce resource situations. Minnesota Department of Health. May 2020. www.health.state.mn.us/communities/ep/surge/crisis/standards.pdf
Smith JE, Gebhart ME. Patient surge. In: Ciottone G, Biddinger PD, Darling RG, et al, eds. Ciottone’s Disaster Medicine. 2nd ed. Philadelphia, PA: Elsevier; 2015;233-40.
U.S. Department of Health and Human Services Hospital Preparedness Program. 2017–2022 Health Care Preparedness and Response Capabilities. November 2016. phe.gov/Preparedness/planning/hpp/reports/Documents/2017-2022-healthcare-pr-capablities.pdf
















1 Comment.
This was a great article. I think that when you can get the entire hospital to understand how they can be so impactful with many doing a little, they can do a lot with a little.