

An innovative program fosters appreciation for nurses.
Takeaways:
- Medical residents participating in a Nurse-for-a-Day program reported that the top lessons they learned included the difficulty and busy-ness of the nursing role.
- Medical residents felt that the program would impact their future practice by improving their communication with nurses, understanding the nurse’s role and workflow, and improving their orders.
- Both medical residents and nurses believed the program would improve their interprofessional communication.
- Nurses reported that they felt more empowered to interact with physicians.
Interprofessional collaboration is the boat that keeps patient safety afloat. Unfortunately, we’ve all seen that boat flounder in rough seas. Teamwork and mutual role understanding serves as the best guide to smoother waters.
Robust collaboration leads to the best care quality, including patient safety outcomes, patient satisfaction, cost savings, and reduced nurse burnout. According to The Joint Commission, communication failure is one of the most common root causes for sentinel events (an adverse event causing serious harm or death). Obstacles to nurse–physician collaboration include limited knowledge of the other’s role, hierarchy, differing goals, and incivility. For these reasons, the World Health Organization and The Joint Commission have recommended interprofessional training to improve patient outcomes.
Setting sail

At Cedars-Sinai Medical Center, our MD–RN Collaborative was designed to address the essential physician–nurse relationship. At a quarterly housewide collaborative meeting, the participants theorized that cultivating this relationship from the beginning of physician training might have lasting impact on interprofessional collaboration. The internal medical residency training program and medical–surgical nursing department developed a shared clinical experience in which all first-year medical residents partnered with nurse preceptors for a 12-hour shift within the first 10 weeks of residency. The goal was for nurses and physicians to collaborate on all aspects of care from patient bathing to medication administration and coordinated implementation. A detailed skills checklist facilitated and guided the clinical activities, and physicians had to demonstrate competencies per hospital policy. We named the program Nurse for a Day (NFAD).
Staff nurses known to be strong communicators were nominated for the program and could choose to precept medical residents as one of their nursing clinical ladder projects. During the program, residents arrived at 7 am and attended morning shift huddle, participated in nursing handoff report, and joined in during progression of care rounds (a daily interprofessional meeting designed to improve patient care delivery, discharge planning, and care coordination). In addition to providing nursing care and coordination under the guidance of their nurse preceptor until 7:30 pm, the residents participated in handoff report to the oncoming nightshift nursing team.
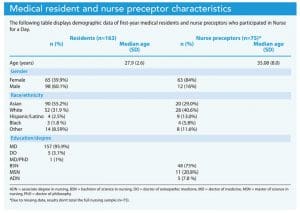
From 2016 to 2020, 163 medical residents and 75 nurse preceptors participated in the NFAD program. Of these participants, 106 (65%) of the residents and 51 (68%) of the nurse preceptors completed an anonymous survey offered at the end of their experience, providing responses to open-ended questions. The responses were then analyzed for themes.
X marks the spot
Mean age for medical residents was 28 years, with the largest percentage identifying as Asian (n=90, 55.2%) and White (n=52, 31.90%). Nurse preceptors’ mean age was 35 years, with the largest percentage identifying as White (n=28, 40.6%) and Asian (n=20, 29%). Most nurses reported having a bachelor of science in nursing (n=48, 75%) or a master’s in nursing (n=11, 20.80%).
Feedback from residents included the top lessons they learned about nurses during the experience. The top two lessons frequently overlapped and included an appreciation of the difficulty of the nursing job (42.45%) and the busyness of the role (27.36%). Residents wrote that “patients can be really mean to nurses,” that “[nurses] are on their feet all day long,” and “I learned how busy they are on a minute-to-minute basis and how demanding their job can be!” The third most common lesson was understanding the nurse’s role/workflow (25.47%). For instance, one resident stated, “I learned that the nurses do so much more than any of the doctors even know.” The residents also recognized nurses as the frontline caregivers (21.70%), saying, “they are […] the face of the care that we provide,” and “after all the deliberation behind closed doors, the nurses are the ones who finally deliver the care.”
When asked to name the best feature of the program, residents pointed to learning the nurse’s role/workflow (51.89%), experiencing nursing skills (33.96%), gaining the nurse perspective (22.69%), and learning how an order is carried out (15.09%). Comments included, “I liked just getting to know the day-to-day work-flow that [nurses] do [such as] how to trouble-shoot things like I.V. pumps and tube feeds,” “I enjoyed seeing the workflow from a nurse perspective,” and “The most interesting part for me was seeing how an order placed by a physician is verified, actuated, and administered by the different members of the healthcare team.”
Resident feedback related to themes that will impact their future practice included understanding the nurses’ role/workflow (35.85%), improving nurse–physician communication (MD 58.9%, RN 29.25%), and improving orders (28.30%). Comments included, “It will give me insight into how a nurse receives the care plan and the important role they play in providing care” and “I think it will help me talk with nurses as well.” A number of residents specifically referenced bundling lab orders, making statements such as, “I will try to order all of my lab tests at the same time so that they do not need to do multiple sticks and irritate/hurt the patient.”
Residents and nurses thought the program would improve interprofessional communication (MDs 29.25%, RNs 35.90%). One resident stated, “Now I think that I will have a more open communication with nurses and be more proactive in keeping the nurses on the same page.” Of those who said their personal communication would be improved, 19% (n=6) specifically stated they would increase communication frequency. One resident said, “[The program] increases my propensity to communicate more often with nurses.” Similarly, a nurse stated, “[The program] helps nurses to know how to have better interdisciplinary conversations with physicians.”
Nurses also reported feeling more empowered to interact with physicians (17.95%). One wrote that the program would impact their practice as a nurse by “being able to proactively […] make suggestions with patients’ overall care and needs with [physicians].”
Lessons from the voyage
Participant survey responses demonstrate how programs such as this have the potential to shape future care delivery. A common theme across all responses was how valuable the program was in cultivating mutual role understanding, particularly in clarifying the nurse’s role and workflow.
We initially thought the NFAD program would be a hard sell to medical residents, but we were pleasantly surprised to learn that residents wanted interprofessional training experiences. We assumed that the opportunity to practice skills would be the biggest draw. The residents did appreciate being able to practice skills (33.96%), but that was secondary to learning about the nurse’s role and workflow (55.89%). When asked how the program could be improved, 25.47% said no improvement was necessary. Of those who did offer suggestions, 36.23% requested a shorter shift and 20.29% asked for more NFAD opportunities. Many participants recommended a 4- to 8-hour shift. Other organizations initiating a similar program will want to determine whether the full 12-hour shift is necessary or perhaps consider a reciprocal interprofessional experience where nurses shadow residents.
To ensure good communication and that the program ran smoothly, we took several steps. For example, to accommodate unforeseen staffing challenges, nursing leadership identified a primary preceptor and a back-up. In addition, reminder emails were sent weekly to preceptors, nursing leadership, and the relevant charge nurses to prepare for resident presence on the unit. To ensure residents had a diverse experience, charge nurses were asked to inform the MD–RN pair of less-common patient care events they could participate in, such as placing indwelling devices or wound care.
Mapping out future journeys
This relatively inexpensive program provided potentially long-lasting benefits. Pairing residents with nurses is primarily an issue of gaining buy-in and coordinating schedules. NFAD highlights the benefits of physicians and nurses serving as co-captains steering patient care. Findings from our project highlight the importance of interprofessional training for residents early in their careers to facilitate interprofessional communication and collaboration by cultivating understanding essential for both physicians and nurses. As one physician participant shared, “I could never have known the physical marathon, complexity, and emotional fulfillment of my colleague’s job without spending a day in the life.” Overall, the program was so well received that we run it annually.
The authors work at Cedars-Sinai Medical Center in Los Angeles, California. Sarah Low is an oncology nurse navigator in the patient family support program at the Samuel Oschin Comprehensive Cancer Institute. Emily Gray is an assistant nurse manager in medical nursing services. Amanda Ewing is director of the internal medicine residency training program. Patricia Hain executive director of surgical nursing services. Linda Kim is a research scientist in the nursing research department.
References
Ansryan LZ, Aronow HU, Borenstein JE, et al. Systems addressing frail elder care: Description of a successful model. J Nurs Adm. 2018;48(1):11-7. doi:10.1097/NNA.0000000000000564
Evans JR, Benore E, Banez GA. The cost-effectiveness of intensive interdisciplinary pediatric chronic pain rehabilitation. J Pediatr Psychol. 2016;41(8):849-56. doi:10.1093/jpepsy/jsv100
Gilbert JHV, Yan J, Hoffman SJ. A WHO report: Framework for action on interprofessional education and collaborative practice. J Allied Health. 2010;39(Suppl 1):196-7.
House S, Havens D. Nurses’ and physicians’ perceptions of nurse–physician collaboration: A systematic review. J Nurs Adm. 2017;47(3):165-71. doi:10.1097/NNA.0000000000000460
Kim LY, Rose DE, Ganz DA, et al. Elements of the healthy work environment associated with lower primary care nurse burnout. Nurs Outlook. 2020;68(1):14-25. doi:10.1016/j.outlook.2019.06.018
Sentinel Event Statistics Released for 2015. Jt Comm Perspect. 2016;36(4):10.
Welp A, Manser T. Integrating teamwork, clinician occupational well-being and patient safety—Development of a conceptual framework based on a systematic review. BMC Health Serv Res. 2016;16:281. doi:10.1186/s12913-016-1535-y
Keywords: Interprofessional collaboration, Physician-nurse collaboration, Communication















