A hospital or healthcare organization may have to review their current fever protocol when purchasing a new type or brand of thermometer. In this white paper, we describe what fever protocols are, and what changes might be involved if fever protocols are changed. In addition, we describe what stakeholders you should keep in mind when pitching Temporal Artery Thermometers to new customers and how to approach systematically a key account for a successful sale.
Background
Fever is a clinical sign of key relevance that characterizes a wide number of conditions, most of them infectious. It has a high clinical value for early diagnosis and treatment of the patient, but also for the protection of close contacts when the condition is transmissible. Thermometry has been essential during the pandemic of SARS COVID-19 to identify patients and act accordingly.
Thermometry methods are diverse, and electronic thermometers have largely replaced mercury thermometers that were banned. There are also differences in the methodology and degree of dependence of the results on the user and the patient between the technologies. Standard-of-care (SOC) methods are currently used in professional and domestic settings, namely electronic devices for measuring oral and cutaneous temperatures, tympanic and temporal arteries. Infrared guns have been widely used in public and domestic spaces during the pandemic, but there is solid evidence that they lack diagnostic accuracy and reliability for clinical use.
A fever is one of the oldest clinical signs. While infection is of great clinical and epidemiological importance today, it was along with trauma the primary cause of death in the past.
The history of thermometry is as long as fever’s, starting with the assessment methods, such as observation and palpation, and progressing through a long list of techniques, including mercury, which has remained the standard of care for centuries. The use of electronic methods has successfully replaced mercury as a global standard of care for good.
As with other essential vital signs, the observer is crucial to the accuracy and precision of the measurement(1). The quality and diagnostic power of vital signs, including thermometry, may be compromised by routine and workflow pressure. Since fever is so important, medical care institutions strive to have a common understanding of the diagnosis and management of fever.
This white paper describes fever management protocols focused on diagnosis.
The fever protocol
An institution’s fever protocol governs clinical decision making in the event of a fever diagnosis. Included in the protocol are subjects such as:
- Definitions (glossary)
- Technical methods
- Cut-off values (diagnostic criteria)
- Decision trees for management
- Cases with a special focus
- Study, reading, and scientific references
A fever protocol assists healthcare professionals in assessing and potentially managing patients’ body temperatures appropriately.
Health care layers must provide solid guidance on fever management. Clinically, the hospital plays a particularly important role, since nosocomial infections are particularly severe. The public health and epidemiological aspects are particularly important at the lower acuity layers, but chronic patients with a lower immunity represent a critical clinical case (oncology and transplant patients, for instance).
Challenges and needs of current practice
Despite its high relevance, there is little consensus on two key aspects of fever management:
- the cut-off values for each standard-of-care (SOC) technique
- the therapeutic attitude
A hospital’s fever protocol is built with less-than- optimal guidance from scientific societies, resulting in significant differences. Changing methods and, accordingly, criteria is a painful process that care givers tend to resist.
The measurement of vital signs during a physical examination is largely suboptimal, and technological advancement has greatly improved the quality of data and the hygienic aspects of the vital sign measurement. A sphygmomanometer or SpO2 gauge that automatically measures the pulse or blood oxygen level has made the measurement more accurate and precise compared to a manual instrument or auscultation of the Korotkoff sounds or palpating the fingernails by sight. With the transition from mercury to electronic thermometers, workflow has improved and newer thermometry techniques, such as the tympanic and temporal artery thermometers, have been available that evolve from the elusive skin temperature to more central estimations. Mercury thermometers were already commonly used for oral and rectal thermometry, and both uses sparked the urge to ban the technique because of the potential toxicity associated with a fractured probe. Electronic skin (axillary and inguinal), oral, and rectal probes are safe and are protected by a disposable sleeve.
Currently, there are four non-invasive thermometry SOCs:
- the axillary (or inguinal)
- oral
- tympanic
- and temporal arteries
There is also a semi-invasive one, the rectal probe. This last method is often considered the gold standard for central temperature. Although SwanGanz catheters are not generally used for measuring temperatures alone, they are obviously the real gold standard for pulmonary artery thermometry.
These methods are widely accepted as standard practice, and the high level of technology makes it easy to choose and use any of them. In other words, thermometry has become a clinical commodity: temperature measurements are accurate and precise, and we are comfortable with their results. However, the normal ranges of each method are poorly agreed upon, except in rectal, and guidelines that unify criteria are not universal or widely accepted.
Numerous publications have compared thermometry methods, including two meta-studies that highlight their limitations due to the wide variety of methodologies used across the studies. The studies focus on accuracy, i.e. bias versus a gold standard. No study includes the inter- and intraobserver variability to examine the precision of the methods and minimize or eliminate user-dependent variability when comparing different methods. Most studies use rectal thermometry as the gold standard instead of pulmonary artery thermometry. There is on the different thermometry methods and the few guides mostly refer to rectal thermometry for fever definitions and severity levels, but rectal thermometry can be intrusive, psychologically aggressive, and has limited, but certain, risks for patients. In the comparison of SOC thermometry methods, there is a need for a comprehensive study that addresses accuracy and precision, that lays the foundation for a more effective clinical optimization of thermometry and proves with empirical evidence how important it is to use every technique correctly for maximum precision.
Such comprehensive studies are rare and impractical for most hospitals, and most rely on already published peer-reviewed studies such as the 100+ studies on successful use of temporal artery thermometers. Hospitals typically accept the studies, then conduct a practical internal study on their own patients to confirm that temporal artery thermometers work for them.
With fever thermometry is essential
Ninety-five percent of ER consultations in pediatrics are related to fever. The patient is already coming in with a high temperature, which leads the family to seek care. The pediatrician will trust more the temperature feeling touching the patient than any thermometry reading, and the most critical aspect of the patient evaluation is the clinical context of the fever: level of consciousness, responsiveness, attitude, color, HR, RR, perfusion, SpO2, etc.
Clinically, nosocomial infections are usually abrupt and severe. Therefore, the clinical evaluation of a patient is key, since a fever can be detected clinically well before the temperature can be measured (shivering, tachycardia, tachypnoea, perfusion, etc.).
The previous statements are reflected in several documents.
– NICE (National Institute for Health and Care Excellence) is a global beacon for medical practice. “Fever in under 5s: assessment and initial management”(2) emphasizes safety of the methods and anatomical adequacy over accuracy and precision (paragraph 1.1 Thermometers and fever detection). This guideline defines fever as “an elevation of body temperature above the normal daily variation.” No cut-off values are provided.
The document recommends against routinely using oral or rectal thermometry. Under 4 weeks of age, only axillary electronic thermometry is used, and from 4weeks to 5years of age, chemical dot axillary and IR tympanic thermometry are used. It is recommended that medical professionals use alternative methods to the chemical dot axillary and forehead chemical because they are rated as unreliable. The IR non- contact thermometers are not mentioned.
– The Royal Marsden Manual of Clinical Nursing Procedures (3) contains a precise and relevant chapter on body temperature physiology and assessment (page 634). The following remarks are important as a guide for diagnosing and managing pyrexia.
First, the differences between core and skin body temperatures are explained in a practical and graphic manner.
The document also covers the methods of recording temperature in depth. There is a blunt statement before the description of the different methods: “Unfortunately, an accurate, non-invasive method for measuring core temperature has yet to be developed, as current instruments produce a wide range of temperatures”(4).
Additionally, when discussing pre-procedural considerations, one key statement stands out: “When using any thermometer, it is essential to ensure that the factors affecting the accuracy and precision of the measurement are controlled.”
This is one of the few documents that address and alert about the bias versus the ground truth core temperature (accuracy) and user-dependent variability (precision).
Pyrexia (fever) is categorized as low-grade, “Normal” to 38°C, moderate to high-grade from 38 to 40°C, and hyperpyrexia above 40°C. The method used or if these are core temperatures are not specified.
– According to the Spanish Society of Paediatrics, fever is defined as 38°C measured at the rectum in family practice(5). In this paper, they acknowledge that the commonly used methods of axillary and oral have a negative bias that has not been well established or standardized. Tympanic IR thermometers are not recommended for domestic use due to their lack of reliability. They conclude that outside of rectal thermometry there is no uniformity in the recommendation of methods neither on the cut-off values for fever.
Tympanic IR thermometry was investigated by the Norwegian Knowledge Center for the Health Services in 2009(6) due to the increased use of the method in Norwegian hospitals. According to them, “Correct and observer-independent use of infrared tympanic thermometry in clinical settings can be challenging. Also, comparing temperature measurements taken at different body sites may be problematic since they are all estimates of what we want to know, the core temperature. This review acknowledges that rectal measurements are imperfect in many ways, despite being considered a reference standard.”
A roadmap for successfully selling Temporal Artery Thermometers
Changes in thermometry methods in any health care facility with a fever protocol are a practical challenge with elements that may be essential or accidental, but each is important. Getting it done requires alignment or best negotiation between all stakeholders involved.
- Since temperature measurement is not always seen as an essential part of fever treatment protocols it is imperative to determine if the status quo at the hospital you are selling to is questionable before considering any changes.
- Checking the relevance and level of discomfort with the standard of care is the starting point. Taking a solid challenge to both aspects is the go- no-go of any protocol change.
- In order to make a decision on a protocol change, the primary stakeholder is the clinician. They play a key role in any protocol change. Following that, other internal stakeholders (biomedical engineering, procurement, management, etc.) join the discussion.
- A commercial process for changing a hospital’s standard of thermometry involves two phases, which can be found in figure 1.
- These estimated times are standard for complicated sales processes involving hospital budgeting and tendering, such as a thermometer for a large hospital. In order to avoid wasting t ime and resources in the second phase, the qualification phase is an important step. One of the worst mistakes here is to focus on the wrong customers. Before working on a strategic sales map and plan, a thorough and fast qualification is essential.
- There will be benefits associated with changing the thermometry, but there will also be costs associated with it. All of them must be clearly defined, outlined, and supported by solid evidence. Exergen’s Temporal Artery flag thermometer has the benefits and costs as shown in figure 2.
- It is vital to have a thorough understanding of and knowledge of the players and interactions involved on the customer side of everything. In figure 3 is a generic map for strategic accounts management. When an entry is not answered, it has a red flag, and all items should have a green.
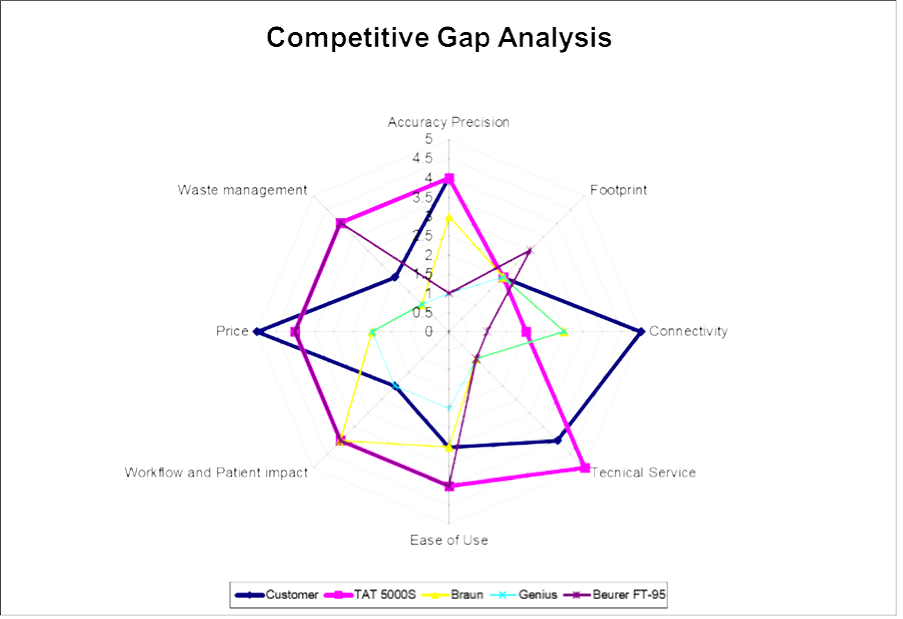
- Based on the information in the strategic map, a competitive gap analysis can be drawn like in figure 4.
- A gap analysis (figure 5) will be conducted by comparing the current thermometry with competing solutions. Every discrepancy in this analysis is a challenge, regardless of whether the Temporal Artery Thermometer, in this example, exceeds (waste management) or lags (connectivity) with respect to the expectations and requirements of the client. In the second case, it fails to deliver, and in the first case, it provides what isn’t needed. Working on aligning both gaps will shape the competitive profile to a better fit.
Figure 1
Figure 2
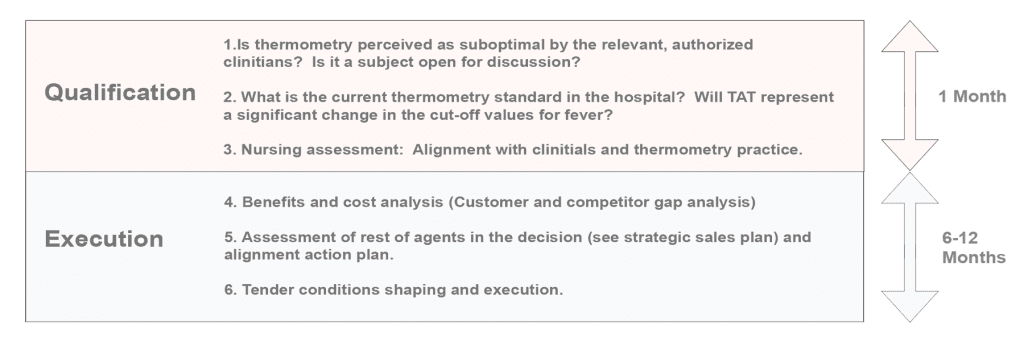
Figure 3
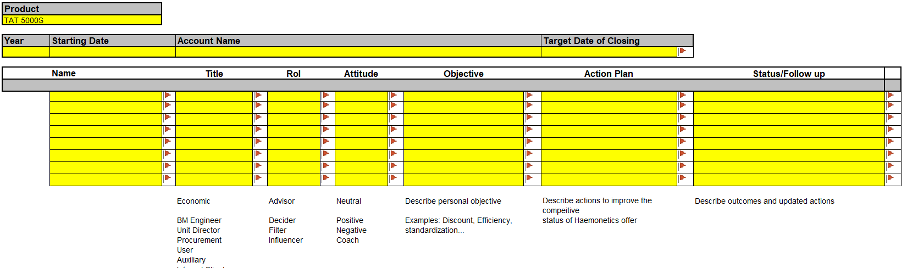
Figure 4
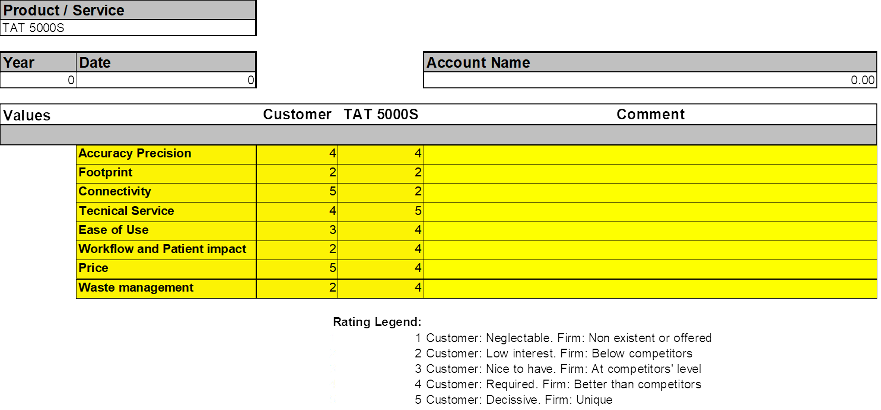
Figure 5
References
1. https://healthcare-in-europe.com/en/news/ blood-pressure-measurement-complex.html
2. NICE Guideline: “Fever in under 5s: assessment and initial management” Published November 2019 (Copyright NICE 2022) https://www.nice. org.uk/guidance/ng143
4. Hooper, V.D. & Andrews, J.O. (2006) Accuracy of noninvasive core temperature measurement in acutely ill adults: the state of the science biolological research for nursing. Biological Research for Nursing, 8(10), 24–34.
5. Ares Álvarez J, Morillo Gutiérrez B. Fiebre sin foco. Rev Pediatr Aten Primaria Supl. 2021;(30):19-28.
6. Holte TO, Vandvik PO, Elvsaas IKØ, Norderhaug IN. Diagnostisk. The diagnostic accuracy of infrared tympanic, oral, axillary and temporal thermometry, compared with rectal readings when identifying fever in adult hospitalized patients. Report from Kunnskapssenteret no. 19−2009. Oslo: Norwegian Knowledge Centre for the Health Services, 2009.