A med–surg telemetry unit takes on patient safety.
- Nationwide, nearly one million falls occur in the hospital-setting each year.
- A medical-surgical telemetry unit implemented the Fall TIPS (Tailoring Interventions for Patient Safety) toolkit to help reduce falls.
- Data collection and analysis indicated a consistent and growing reduction in falls.
One unit’s challenge
In 2022, an 800-bed New Jersey hospital experienced 357 inpatient falls and 79 related injuries. The med–surg telemetry unit had the fifth highest number of falls among the hospital’s 34 inpatient units. Improper ambulation and inadequate patient education accounted for half of the unit’s falls.
Tailored falls prevention plans
Although the Fall TIPS (Tailoring Interventions for Patient Safety) program, based on the Morse Fall Scale, offers an evidence-based fall-risk assessment, the hospital’s nurses determine a patient’s fall risk using the Hendrich II assessment tool, which calls for placing all patients who score 5 or higher on universal fall precautions with additional protections (such as bed alarms or video monitors). These patients receive a yellow high-fall-risk wristband. Per the hospital’s policy, the Hendrich assessment occurs at admission and transfer, during every shift, if the patient’s status changes, and after a fall event.
However, limitations exist in identifying the degree of risk based on a wristband or any other indicators in the patient room. For example, non-primary nurses and nurse ancillary staff can’t easily determine the extent of a patient’s ambulatory status or fall prevention plan. This poses a potential safety issue for healthcare team members when they enter a patient’s room for the first time. In addition, family members or visitors don’t have easy access to this information. Without familiarity of a patient’s fall assessment and prevention plan, nurses and others can’t reliably enact appropriate preventive measures. Ultimately, the risk of falling increases.
The Agency for Healthcare Research and Quality (AHRQ) states that fall prevention should include three steps: assess fall risk, develop a personalized prevention plan, and consistently implement the plan. To reduce its fall rate, this hospital initiated a quality improvement project using the Fall TIPS toolkit to address the following question: Within the inpatient med–surg telemetry unit, how does the implementation of the evidence-based Fall TIPS toolkit compare to current practice and impact the rate of falls within a 1-year period?
What we did
The QI project included all patients on the med–surg telemetry unit in the Fall TIPS program. All full-time, part-time, and per diem nurses and nursing assistants participated in education about the program. We excluded any nurses or nursing assistants who didn’t serve as dedicated unit staff as well as all non-nurse and non-nursing assistant staff.
Using the Plan-Do-Study-Act model, we followed these implementation steps:
- During admission, transfer, bedside report, and patient status change, nurses engage with patients and families to assess fall risks.
- In collaboration with patients and families, nurses tailor a personalized fall prevention plan.
- Patient care team members consistently note fall risks and interventions using the bedside communication tool.
In addition, nursing assistants confirm completion of the communication (a printed and laminated blank tool hangs in each patient room to allow for on-the-spot customization using dry-erase markers). Nursing assistants also have responsibility for engaging with the patient and family to ensure their understanding and for reporting to nurses any changes noted in the patient’s status. (See Bedside communication tool.)
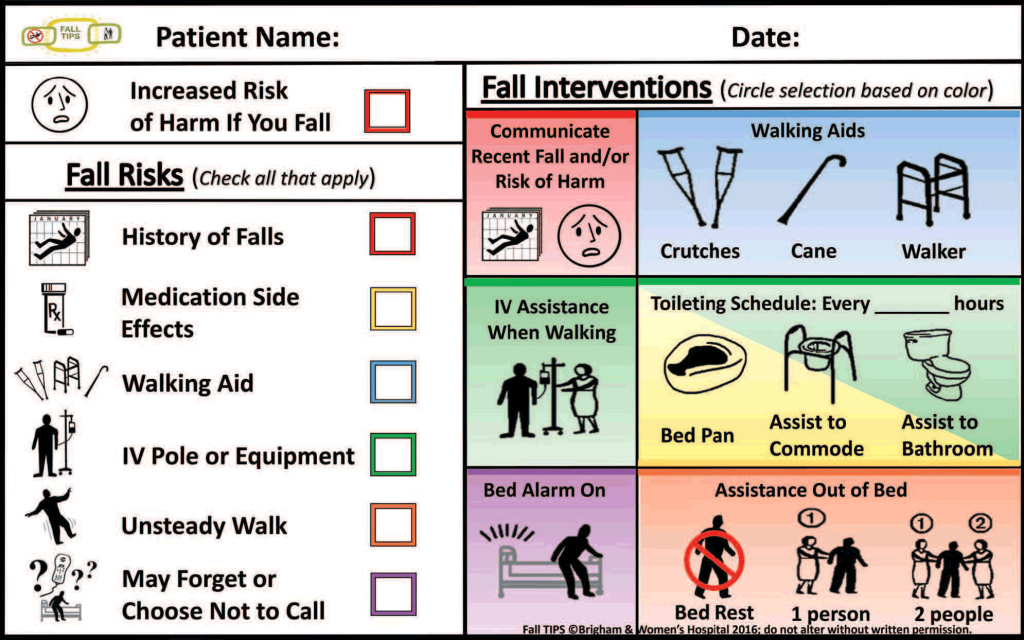
Bedside communication tool
We printed and laminated the following bedside falls communication tool to hang on the wall in all med–surg telemetry unit patient rooms. Nursing assistants ensure tool completion and use it to engage with patients and family members.
Trained Fall TIPS champions completed audits throughout the intervention. They also served as resources to the team, answering questions and providing any required additional direction. Their presence ensured adherence and helped to identify obstacles.
We established several outcome pre- and post-intervention measures for this QI project, including the number of falls and staff knowledge. We measured staff knowledge of fall risks and reduction strategies using the validated Fall Prevention Knowledge Test (FPKT), which we administered before providing education and 8 weeks after Fall TIPS implementation. We also used the FPKT to measure staff members’ perceived confidence in their ability to prevent falls.
Using the Fall Prevention Efficiency Scale (FPES), we measured staff opinion regarding the unit’s fall prevention methods and efficacy before protocol education and 8 weeks after implementation.
What we learned
We used the hospital’s Research Electronic Data Capture survey software to gather FPKT, FPES, and audit data in a central and secure location. We then used IBM SPSS Statistics 27 to analyze the data and draw conclusions on statistical significance. An initial analysis was conducted after 8 weeks of implementation; we performed additional analysis after 1 year and after 15 months.
The 8-week analysis of surveys and test scores revealed an increase in staff knowledge of fall risks and reduction strategies. We also found an increase in staff confidence in their ability to prevent falls. In addition, the analysis showed a maintained satisfaction with the unit’s fall prevention methods.
The analysis of all audits performed by Fall TIPS champions within the initial 8 weeks suggested 100% adherence with all aspects of the project by all staff. Compared to the unit’s 2022 falls, we saw a 29.4% reduction during the implementation period. In addition, the two falls that occurred weren’t related to improper ambulation or fall education (the cause of half of the unit’s falls before implementation).
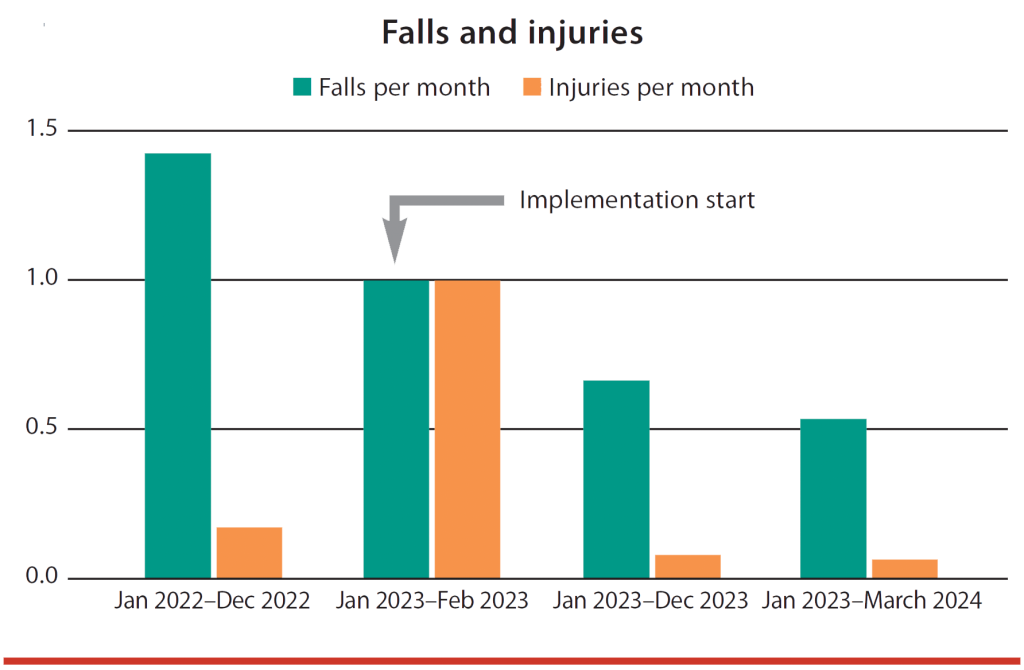
The 1-year assessment revealed that falls reduction had improved by 53%. In addition, we saw a 51% reduction in injurious falls (those that cause new signs/symptoms ranging from minor swelling to major fractures) compared to 2022. The 15-month reassessment showed 63% falls reduction and a 64% injurious falls reduction. (See QI project outcomes.)
QI project outcomes
We saw a reduction in falls and injuries per month 8 weeks after implementation of the Fall TIPS protocol. That reduction continued at 12 and 15 months.
Limitations. Project limitations include the 8-week implementation period. Studies indicate that as more implementation time transpires, greater adherence occurs among staff, which leads to more significant fall reduction. Our 12- and 15-month data support this. A longer implementation period will better reflect the impact of the Fall TIPS program, specifically regarding the FPES and FPKT results, which weren’t repeated at 12 and 15 months. Repeating these assessments will lend more validity to the results.
In addition, education should occur over a longer period and be offered throughout the year for those who’ve already participated, new hires, and anyone who missed the initial education. Repeating the pre-implementation education would ensure more staff have access to it and serve as a refresher.
Staff satisfaction and adherence
The implementation of the Fall TIPS program on the med–surg telemetry unit had a positive impact within the initial 8-week implementation period, and it continues to yield promising results. Staff members’ knowledge and confidence in fall prevention increased, which improved the staff’s practice and their ability to educate patients and families. This allows a lasting impact on fall reduction.
Adherence to any new protocol requires staff satisfaction. In this case, staff will more likely continue fall-prevention actions in their daily workflow. Overall, the data gathered by the QI team aligns with the project’s overarching goal and the supporting research—a substantial and continuing reduction in falls, fewer injuries, and elimination of factors that once caused half of the units falls.
Keep patients safe
We will continue to track the rate of falls on this unit to analyze maintenance and improvement. If positive effects persist, we’ll have substantial evidence for implementation throughout the hospital and even within the entire healthcare network.
This further implementation might include integration within the electronic health record to accommodate higher technology areas, as well as throughout several other aspects of patient care. As this expansion of the Fall TIPS program occurs, we’ll gather more data to determine efficacy for other patient populations, which would translate into consistent collaboration among nurses, patients, and families throughout a hospital stay. Ultimately, this would allow for a standardized improvement of nursing care in all areas. The goal remains to eliminate preventable falls and keep patients safe.
Hannah Pathan is manager of nursing quality at Hackensack University Medical Center in Hackensack, New Jersey. April Camiling-Burke is a nurse scientist at Hackensack University Medical Center. Carolene Stephenson is a nurse scientist and nurse practitioner at Hackensack Meridian Health. Julie Romano is a nurse manager at Hackensack University Medical Center. Ahmad Singer is an administrative director at Hackensack University Medical Center.
American Nurse Journal. 2025; 20(4). Doi: 10.51256/ANJ042533
References
Agency for Healthcare Research and Quality. About Fall TIPS. falltips.org/about-fall-tips
Agency for Healthcare Research and Quality. Fall TIPS: A patient-centered fall prevention toolkit. February 2021. ahrq.gov/patient-safety/settings/hospital/fall-tips/index.html
Agency for Healthcare Research and Quality. Preventing falls in hospitals. February 2024. ahrq.gov/patient-safety/settings/hospital/fall-prevention/toolkit/index.html
Dykes PC, Adelman JS, Alfieri L, et al. The Fall TIPS (Tailoring Interventions for Patient Safety) program: A collaboration to end the persistent problem of patient falls. Nurse Lead. 2019; 17(4):365-370. 10.1016/j.mnl.2018.11.006
Dykes PC, Burns Z, Adelman J, et al. Evaluation of a patient-centered fall-prevention tool kit to reduce falls and injuries: A nonrandomized controlled trial. JAMA Netw Open. 2020;3(11):e2025889. doi:10.1001/ jamanetworkopen.2020.25889
Dykes PC, Duckworth M, Cunningham S, et al. Pilot testing Fall TIPS (Tailoring Interventions for Patient Safety): A patient-centered fall prevention toolkit. Jt Comm J Qual Patient Saf. 2017;43(8):403-13. doi:10.1016/j.jcjq.2017.05.002
Venema DM, Skinner AM, Nailon R, Conley D, High R, Jones KJ. Patient and system factors associated with unassisted and injurious falls in hospitals: An observational study. BMC Geriatr. 2019;19(1):348. doi: 10.1186/s12877-019-1368-8
Key words: fall prevention, fall reduction, in-patient falls, Fall TIPS toolkit