

Empathy and respect open the door to good outcomes.
CNE: 1.5 contact Hours
Objectives:
- Describe practices to provide equitable, quality, effective culture-sensitive and patient-centered (CS/PC) care.
- Discuss relationship building, assessment and care planning, and patient and caregiver education to promote CS/PC care.
- Describe strategies to enhance home health nurses’ cultural sensitivity and augment patient-centered care.
The authors and planners of this CNE activity have disclosed no relevant financial relationships with any commercial companies pertaining to this activity. See the last page of the article to learn how to earn CNE credit.
Expiration: 7/1/25
Takeaways:
- Nurses can help address healthcare inequities by incorporating culture-sensitive/patient-centered (CS/PC) strategies into their care.
- CS/PC strategies enhance the three essential skills of home health nursing: building a caring-trusting relationship with the patient, holistic and advanced assessment and care planning skills, and effective patient/caregiver education strategies.
- Actions that can help home health nurses develop CS/PC skills include cultivating CS/PC attitudes and values, understanding self and patient as cultural beings, communicating effectively, and incorporating CS/PC practices into assessment and care planning practices.
Patient diversity stems from race, ethnicity, religion, age, gender identity, sexual orientation, socioeconomic status, education, occupation, political affiliation, abilities, disabilities, stigmatized diagnoses, shared life experiences, or any of the many other ways people perceive themselves. Each diversity group has its own cultural norms, which include worldviews, beliefs, values, ethical systems, etiquette, aspirations, behaviors, and practices, including those related to healthcare.
No one person is an exemplar of any cultural group. Everyone belongs to multiple diversity groups, and each person may or may not adhere to the norms of each of their groups. In other words, each diversity group is, in turn, diverse. In addition, each patient (and nurse) develops their own unique culture—ways of thinking about, being, and acting in the world—which affects how they think about health, illness, and health promotion. Nurses must recognize patients as cultural beings and adapt their care to each patient’s culture.
Prevalent and harmful healthcare disparities place many vulnerable and marginalized groups at risk for poor health outcomes, including those in home settings. According to the Future of Nursing 2020–2030 report, the top priority for nursing in the upcoming decade is to address and mitigate health inequities. Providing equitable, quality, effective care requires nurses to enhance the culture-sensitivity and patient-centeredness of their care processes.
Three skills—relationship building, assessment and care planning, and patient and caregiver education—can help home health nurses (HHNs) deliver evidence-based, culture-sensitive/patient-centered (CS/PC) care. (This article replaces “culturally competent care” with “culture-sensitive care” because it’s more patient-centered.) In addition, six strategies can enhance HHNs’ cultural sensitivity and augment patient-centered care. Although written for HHNs, much of this guidance is relevant to nurses and clinicians in all settings.
Relationship-building skills
Most HHNs manage and visit patients over weeks and even months. They report that developing high-quality caring and trusting relationships with patients is more important in home care than in other settings. HHNs quickly learn that they’re not in control of the patient’s environment or what the patient does.
As a guest in the patient’s home, your ability to help the patient achieve the best health grows out of the bond you create with them. This relationship enables patients to reveal important assessment data that they otherwise might conceal; engage in care planning, which in turn promotes adherence; and to be open to your teaching and recommendations about disease management and health promotion.
A strong patient–nurse bond, which relies on your caring attitude and behavior, helps the patient perceive that you care for them as a unique, valued individual and answers the question, “Why should I trust you?” Because we display respect for one another through proper etiquette, exhibit good guest behavior and adapt to the patient’s etiquette norms.
Assessment and care planning skills
Because HHNs frequently are the only professional care providers who see medically fragile patients in their homes, you must have advanced physical assessment skills. You also must perform a holistic assessment to ensure you discover all of the factors—home, community, safety, financial resources, and caregiver availability and competence—that promote or hinder the patient’s ability to achieve and maintain their best health. Which factors require assessment depend on the patient’s diagnoses, anticipated length of stay in home care, and their unique needs.
Perform an in-depth psychosocial assessment of the patients’ personal needs, preferences, values, and life/health goals. Also conduct a cultural assessment, which might include the patient’s ethical and etiquette systems, health/illness beliefs and values, spirituality, sexuality, medication/herbal/nutraceutical/alternative treatment practices, nutritional practices/food preferences, hygiene routines, modesty norms, pain-management practices, and language/literacy/health literacy. The information gathered can help you better understand the patient and plan care that’s acceptable and more likely to be followed.
Patient and caregiver education skills
HHNs teach patients and families how to perform some of the procedures nurses normally provide. They also educate and coach patients about diet, activity and exercise, medications, disease-management strategies, and early recognition of disease exacerbation signs and symptoms.
To successfully help patients develop daily care independence, you’ll need well-developed teaching–learning skills that mirror the nursing process: assessment (learning needs, facilitators, and barriers), diagnosis (knowledge deficits), expected outcomes (learning goals), planning (teaching strategy that strengthens learning facilitators and addresses barriers), implementation (use of teaching–learning principles), and evaluation (teach-backs, return demonstrations, behavior changes).
Learning facilitators include a desire to learn, advanced education, high health literacy, and supportive caregivers. In addition to a lack of learning facilitators, barriers among patients include factors such as pain, fatigue, limited cognitive abilities, and a chaotic environment. These barriers may require you to adapt the learning plan.
Effective planning requires knowing what, where, when, and how to teach. It includes methods for adapting to a patient’s physical, cognitive, and emotional needs. Several teaching–learning principles can aid implementation. For example, Suter and Suter developed a list of 10 timeless principles. These principles include linking new knowledge with old knowledge (such as building on a patient’s occupational knowledge as a plumber to make analogies about how the heart functions as a pump), using physical action to aid topic retention, providing supportive feedback, building on the therapeutic relationship to promote collaborative learning, discussing how the topic relates to the patient’s quality of life, and using problem solving in hypothetical situations.
Assessing a patient’s learning needs starts with effective communication, which requires adapting to the patient’s language by securing an interpreter for teaching sessions and providing translated educational resources (to ensure the patient understands), literacy (to determine appropriate educational resources and the ability to follow written instructions), and health literacy (to determine where you should start with health education). Assess the patients’ understanding of their health issues, what “health” means to the patient, and their personal, cultural, and diversity values and preferences related to learning needs.
Enhancing CS/PC care
CS/PC care aims to help the patient achieve not only health, but also a sense of well-being. Three principles guide CS/PC care: establishing a warm, caring, trusting relationship with the patient; assessing the patient to understand their unique story, aspirations, values, needs, and cultural preferences; and collaborating with the patient as an equal partner to develop a plan that promotes their health. You can enhance your ability to include these principles in patient care by following six strategies: cultivate CS/PC attitudes and values, know yourself, understand how culture impacts patients and their care, communicate effectively, implement assessment approaches, and implement care planning tactics.
Cultivate CS/PC attitudes and values
According to the American Nurses Association’s Code of Ethics for Nurses with Interpretive Statements, “The nurse practices with compassion and respect for the inherent dignity, worth, and unique attributes of every person.” You can cultivate the attitudes, values, and behaviors inherent to this standard by committing to CS/PC care, which encompasses empathy, compassion, and acceptance. Approach patients with an egalitarian attitude and cultural humility, and acknowledge them as experts in their culture and care needs. In addition, be open to patients’ beliefs, values, aspirations, and practices, and adapt care to their norms.
Know yourself
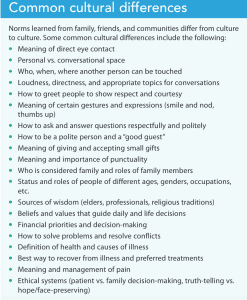
Cultural sensitivity grows when we understand ourselves as cultural beings with biases. Consider why you have the beliefs, values, and preferences that you do. We tend to learn norms from families, friends, teachers, and communities, so they feel like the “right” ones; and they are right when within our groups. However, most cultural norms are neither right nor wrong in and of themselves, they’re just different from others’ norms. In every patient encounter, two cultures (nurse’s and patient’s) interact. Because nurses are guests in patients’ homes (their domains) and because we have an obligation to facilitate patients’ well-being, we must adapt to their cultural norms. Doing this helps build a caring–trusting relationship. (See Common cultural differences.)
Recognize and manage implicit bias. Since many of our deepest beliefs and values have been ingrained in us from an early age, we have biases, both positive and negative. Implicit biases aren’t bad per se; they’re part of the human condition, and everyone has them. They become bad when they manifest in discriminatory thinking and actions. Every nurse has an obligation to acknowledge their intrinsic biases and then successfully manage them.
Pay attention to your feelings when assigned to a patient of a different diversity group. If we feel discomfort, distaste, or fear, or make negative assumptions about the patient before getting to know them, we probably have an implicit bias that might be harmful to the patient. To prevent harm, recognize the bias so you can mindfully manage it. To manage bias, intentionally commit to CS/PC values each day. Also consider taking a moment at the patient’s doorstep to ask yourself about any negative feelings, acknowledge them, and then commit to practice egalitarian, quality care for this patient.
Understand how culture impacts patients and their care
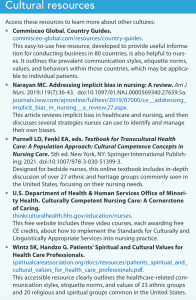
Just like you, your patients are cultural beings and their cultures affect how they think and behave. Although the best way to find out about a patient’s culture is directly from the patient, reviewing background information from cultural resources (books, journal articles, websites, group representatives) can be helpful. Seek this information not to pigeon-hole the patient, but to understand what you might otherwise misunderstand or overlook. For example, patients rarely articulate the nonverbal communication or etiquette norms of their cultural groups, but understanding these critical attributes help build a caring relationship with the patient. (See Cultural resources.)
However, remember that cultural guides won’t tell you what an individual patient thinks or does. Cultures are dynamic, and patients adapt to new cultures in their own unique ways. Don’t assume that a patient adheres to all, or even any, of the norms of their culture of origin. The best way to know the patient’s culture is to ask them.
Communicate effectively
According to the U.S. Department of Health & Human Services’ Office of Minority Health’s Standards for Culturally and Linguistically Appropriate Services, healthcare providers must ensure “meaningful communication” with limited-English proficient (LEP) patients. Most home health agencies contract with telephonic language services who employ medical interpreters to meet this mandate. Medical interpreters are the gold standard when communicating with LEP patients, but many patients prefer family interpreters. If you have any concerns about the competency or care (for example if you suspect abuse) of family or lay interpreters, use medical interpretation services.
When relying on family interpreters, you must be confident that they can clearly convey assessment questions and answers as well as patient education instructions regarding safety and disease management. Keep in mind that family members may not have the vocabulary necessary in both languages to accurately convey health information, and their emotions may color their interpretations. Never rely on nonadult children to interpret. Placing children in this role is unethical and may be illegal. Inadequate interpretation may prevent relationship-building, assessment and care planning, and patient education, which can jeopardize care.
Implement assessment approaches
Effective assessment requires caring and trusting relationships. As soon as you arrive at the home, greet the patient or caregiver with a friendly smile. Be alert for the patient’s nonverbal communication and etiquette norms and mirror them.
When entering the patient’s home, begin your assessment. Assess the home (shoes at the door, cultural or spiritual artifacts), interactions between family members, and patient behaviors. Assess the social determinants of health (neighborhood safety and resources, financial resources, access to nutrition and transportation). Ask the patient to tell you their story about why the doctor recommended a nursing visit, what concerns them about their health problem, and what they hope the outcome will be.
Determine how well the patient understands and speaks English. They must be able to read in English or their native language (if they’re not English proficient) for consents and education. Also assess the patient’s health literacy and make adaptations so you can communicate using words, concepts, and aids that they’ll understand.
As part of the assessment, ask, “I want to be respectful of you and what’s important to you. What should I know about your culture [or family, religion, daily routines, life challenges as appropriate to the patient] to ensure that respect?” Or ask, “Can you teach me what I need to know about your culture [or substitute word] to best help you with your care and health problems?”
For all Medicare patients, home care nurses must complete an Outcomes and Assessment Information Set (OASIS). However, a truly comprehensive assessment should include questions important to a patient’s cultural perspective that aren’t part of OASIS. Don’t be afraid to ask a patient about how their culture (or other diversity element) might affect their care. For example, some people who practice Islam may not use their right hand during toileting, so asking about hygiene practices can inform how you teach ostomy care.
Implement care planning tactics
Collaborate with the patient as an equal partner to create a care plan that reflects their values and health goals. The transcultural nursing literature describes a powerful CS/PC care planning framework: Strengthen–Accommodate–Restructure. This strategy promotes care planning that honors the patient as a partner, helps build the caring–trusting relationship, and encourages patient engagement and adherence to the care plan.
Strengthen the helpful. Note the patient’s cultural norms (from any of the patient’s diversity groups) while performing the assessment. Evidence indicates that many cultural norms, such as large families living in multigenerational households and meditative spiritual practices promote good health and well-being outcomes. Including these helpful cultural norms into the care plan aids trust building with the patient when discussing other elements of care.
Accommodate the neutral. Most cultural norms are neither helpful nor harmful, but actively accommodating them into care plans acknowledges patients as unique individuals and helps build trust. For example, if you have a patient who practices Islam and prefers not to use their right hand for ostomy care based on those religious beliefs, accommodate that preference. Brainstorm with the patient about how ostomy care can be performed without violating that cultural norm. Perhaps gloves are an option, or consider consulting with an occupational therapist. Accommodating these neutral cultural norms will help you when it comes time to address beliefs or practices that may be harmful.
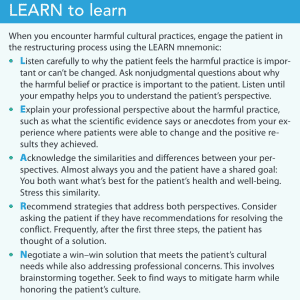
Restructure the harmful. Some cultural practices and outlooks—such as eating high-fat or high-sodium foods or having a fatalistic outlook (“Adhering or not adhering to the diet won’t make a difference in my outcomes.”)—can be harmful to the patient’s health. Patients have a right to their autonomous decisions, but sometimes nonadherence results from a lack of knowledge or motivation. You have the tools—such as motivational interviewing/coaching practices and the LEARN technique for providing science-based information—to overcome these challenges. (See LEARN to learn.)
Meet your obligations
HHNs and nurses in all settings have an obligation to provide equitable, high-quality care, address inequalities, and mitigate disparities. CS/PC care aids these efforts and ensures that the care plan is the patient’s care plan. You may not be able to accomplish all you want for patients, but you can help make their lives better.
Mary Curry Narayan is a home health clinical nurse specialist and transcultural nursing consultant at Narayan Associates in Vienna, Virginia.
Acknowledgment
Some of the recommendations described here are based on research findings funded by the Research Institute for Home Care.
References
American Nurses Association. Code of Ethics for Nurses with Interpretive Statements. Silver Spring, MD: American Nurses Association; 2015.
American Nurses Association. Home Health Nursing: Scope and Standards of Practice. Silver Spring, MD: American Nurses Association; 2014.
Berlin EA, Fowkes Jr WC. A teaching framework for cross-cultural health care—Application in family practice. West J Med. 1983;139(6):934-8.
Graffigna G, Barello S. Spotlight on the patient health engagement model (PHE model): A psychosocial theory to understand people’s meaningful engagement in their own health care. Patient Prefer Adherence. 2018;12:1261-71. doi:10.2147/PPA.S145646
Marrelli TM. The Handbook of Home Health Standards: Quality, Documentation and Reimbursement. 6th ed. Englewood, CA: Marrelli & Associates; 2018.
McFarland MR, Wehbe-Alamah HB. Leininger’s Transcultural Nursing: Concepts, Theories, Research & Practice. 4th ed. New York, NY: McGraw-Hill Education; 2018.
Narayan MC. Addressing implicit bias in nursing: A review. Am J Nurs. 2019;119(7):36-43. doi:10.1097/01.NAJ.0000569340.27659.5a
Narayan MC. Cultural competence in home healthcare nursing: Disparity, cost, regulatory, accreditation, ethical, and practice issues. Home Healthc Manag & Pract. 2020;32(2):76-80. doi:10.1177/1084822319883818
Narayan MC. Six steps towards cultural competence: A clinician’s guide. Home Healthc Manag Pract. 2002;14(5):378-86. doi:10.1177/1084822302014005010
Narayan MC, Mallinson RK. Transcultural nurse views on culture-sensitive/patient-centered assessment and care-planning: A descriptive study. J Transcult Nurs. 2022;33(2):150-60. doi:10.1177/10436596211046986
Narayan MC, Scafide KN. Systematic review of racial/ethnic outcome disparities in home health care. J Transcult Nurs. 2017;28(6):598-607. doi:10.1177/1043659617700710
Ray MA. Transcultural Caring Dynamics in Nursing and Health Care. 2nd ed. Philadelphia, PA: F.A. Davis; 2016.
Suter PM, Suter WN. Patient education. Timeless principles of learning: A solid foundation for enhancing chronic disease self-management. Home Healthc Nurse. 2008;26(2):82-8. doi:10.1097/01.NHH.0000311024.11023.09
U.S. Department of Health & Human Services. National culturally and linguistically appropriate services standards. thinkculturalhealth.hhs.gov/clas/standards
Wakefield MK, Williams DR, Le Menestrel S, Falubert, JL. The Future of Nursing 2020-2030: Charting a Path to Achieve Health Equity. Washington, DC: National Academies Press; 2021. doi:10.17226/25982
Key words: culturally competent care, patient-centered care, home health nursing, healthcare inequities, health care disparities















2 Comments. Leave new
Excellent reminder ; “Meet people where they are”, then the healing begins.
I found this article helpful and a good reminder in how to be culture sensitive and patient centered in giving education and care for individual patient needs.