Astute triage and timely treatment lead to a good outcome.
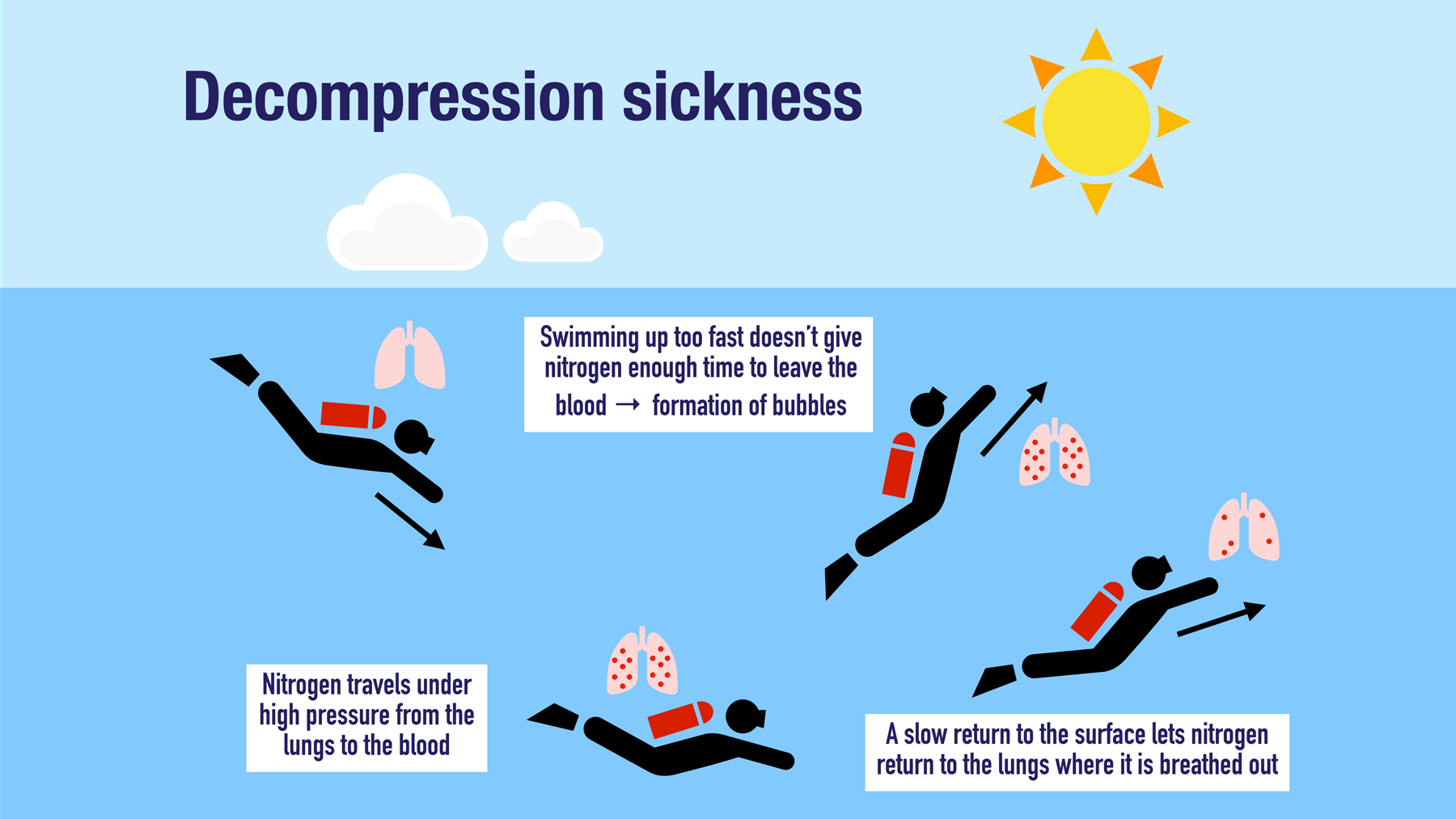
- Decompression sickness is caused by the formation of gas bubbles inside the body during depressurization (for example decompression during scuba diving and flying in an unpressurized aircraft).
- Decompression sickness is a clinical diagnosis, and the mainstay of treatment is 100% oxygen followed by hyperbaric oxygen therapy.
History and assessment
In the ED, Ms. Montgomery informs nurse Mark that she became anxious during her last 40-foot dive and wanted to get to the surface quickly. She describes her right shoulder pain as deep and throbbing, and she reports extreme fatigue. She hasn’t taken any over-the-counter medications for her symptoms.
Ms. Montgomery’s vital signs include temperature 97.9° F (36.6° C), heart rate 98 beats per minute, respiratory rate 20 breaths per minute, blood pressure 132/76 mmHg, and oxygen saturation 93% on room air. Concerned about decompression sickness (DCS), Mark places Ms. Montgomery on 100% oxygen via a non-rebreather mask and secures a bed for her in the treatment area.
Decompression sickness symptoms
Symptoms of Type I and II decompression sickness include the following:
Type I
- Cutis marmorata (itching or painful red-blue skin discoloration)
- Decreased appetite
- Fatigue
- Joint pain
- Lymphadenopathy
Type II
- Altered sensorium
- Ataxia
- Headache
- Hearing impairment
- Motor weakness
- Nausea
- Paresthesia
- Tinnitus
- Vertigo
- Visual impairment
Taking action
Mark notifies the attending ED physician about Ms. Montgomery’s arrival and promptly transports the patient for a STAT chest x-ray, which shows no abnormalities. Ms. Montgomery’s physical examination reveals right shoulder and localized muscle tenderness. Otherwise, her exam is unremarkable with no evidence of barotrauma on otoscopy. Mark initiates I.V. fluid hydration, and Ms. Montgomery is admitted for hyperbaric oxygen therapy.
Outcome
On the med-surg unit, nurses closely monitor Ms. Montgomery’s vital signs, and she’s weaned from supplemental oxygen. After a second hyperbaric oxygen therapy session, her symptoms resolve and she’s discharged to home with close primary care follow-up.
Education and follow up
DCS results from the formation of gas bubbles inside the body during depressurization. When formed in the circulation, these gas bubbles can lead to inflammation and vascular obstruction. DCS incidence is rare (one out of every 10,000 dives) and is more common in men than women. Risk factors include dehydration, alcohol consumption, obesity, pulmonary disease, cold temperatures, and patent foramen ovale. Those working in pressurized environments are at greatest risk for DCS.
The severity of DCS depends on the length and depth of dive, water temperature, intensity of exercise at depth, and the speed of ascent. Type I DCS includes skin, musculoskeletal, and/or lymphatic involvement. Type II is characterized by central nervous system symptoms. Type III DCS can result in frequently lethal pulmonary complications. Ms. Montgomery had Type I DCS. (See Decompression sickness symptoms)
DCS is a clinical diagnosis with symptom onset primarily within 1 hour. Treatment includes 100% oxygen followed by hyperbaric oxygen therapy to clear nitrogen accumulated in the vasculature and tissues. Before initiating hyperbaric oxygen therapy, a chest x-ray must be performed to rule out a pneumothorax. I.V. fluid administration addresses dehydration.
DCS frequently resembles other potentially fatal diagnoses such as pulmonary embolism and myocardial infarction. Mark’s astute triage assessment facilitated timely implementation of an evidence-based treatment plan.
*Names are fictitious.
Aaron M. Sebach is Dean of the College of Health Professions and Natural Sciences at Wilmington University in New Castle, Delaware, and a nurse practitioner at TidalHealth Peninsula Regional in Salisbury, Maryland.
References
Cooper JS, Hanson KC. Decompression sickness. StatPearls. December 13, 2023. ncbi.nlm.nih.gov/books/NBK537264/#:~:text=Decompression%20sickness%20(DCS)%20occurs%20when,inside%20the%20body%20on%20depressurization
Mitchell SJ. DCS or DCI? The difference and why it matters. Diving Hyperb Med. 2019;49(3):152-3. doi:10.28920/dhm49.3.152-153
Tawar A, Gokulakrishnan P. Decompression illness. J Marine Med Soc. 2019;21(2):112-5. doi:10.4103/jmms.jmms_32_19
Undersea and Hyperbaric Medical Society. Decompression sickness. uhms.org/5-decompression-sickness.html
Keywords: scuba diving, decompression sickness