

The nurse’s role in supporting patients and their families.
Takeaways:
- Dissociative disorders are a group of psychiatric disorders that result from experiencing or witnessing trauma; affects up to 10% of the general population.
- As essential partners in the care of individuals with dissociative disorders, nurses perform safety and suicide assessments, teach emotion-regulation skills, help manage pain, and implement other crucial interventions.
- COVID-19 has caused an increase in traumatic experiences for the general public, including nurses, who must be vigilant in assessing for the possibility of DDs and other mental illnesses for months and years to come.
Have you ever driven home after a long day at work, lost in your thoughts, and missed your turn or exit? Have you ever found yourself so engrossed in a book or television show that you didn’t notice your dinner burning on the stove? These relatively benign experiences are examples of dissociation, or disruptions in our normal consciousness, memory, perception, emotion, and behavior. Dissociation exists on a continuum, and at the extreme end, pathological dissociation can cause debilitating impairment that affects all aspects of an individual’s life. Severe, persistent symptoms can lead to a diagnosis of a dissociative disorder (DD).
What are DDs?
This group of psychiatric disorders results from experiencing or witnessing trauma, including child abuse and neglect, intimate partner violence, accidents, natural disasters, and human trafficking. In an effort to survive these overwhelming traumatic experiences, the brain attempts to self-protect by “numbing out” or “going away” (dissociating). This strategy may be adaptive in the moment, but prolonged and repeated dissociation episodes that continue to occur months or years after a traumatic experience can severely impair an individual’s daily functioning in work, school, and relationships.
The experience of trauma is subjective and individualized, so what one person experiences as a traumatic event may not be considered traumatic by another. Similarly, not all traumatic experiences lead to DDs. According to the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), this diagnostic group includes dissociative identity disorder (formerly multiple personality disorder), dissociative amnesia, depersonalization/derealization disorder, and other specified/unspecified dissociative disorders.
In adulthood, DDs commonly are misdiagnosed as mood disorders (such as bipolar disorder) or psychotic disorders (such as schizophrenia). Due to stigma, a shortage of trained providers, and a variety of other factors, an individual might not be accurately diagnosed for up to an average of 7 years.
Children can be diagnosed with DDs, but diagnosis is more common in adulthood. Children frequently are misdiagnosed as having oppositional defiant disorder, conduct disorder, or attention-deficit/hyperactivity disorder. The Structured Clinical Interview for DSM-IV Dissociative Disorders, Revised is the gold standard for accurate diagnosis. It can be completed on its own or with other diagnostic tests, such as the Multidimensional Inventory of Dissociation or Dissociative Experiences Scale. Common DD comorbidities include depression, anxiety disorders, posttraumatic stress disorder, eating disorders, personality disorders, and other trauma-related disorders.
The International Society for the Study of Trauma and Dissociation estimates that DDs affect up to 10% of the U.S. population (about 32 million people). Due to the prevalence of these disorders and the significant risk for self-harm and suicide, nurses must know how to recognize the signs and symptoms of DDs and intervene appropriately.
Educational and support resources
Nurses should use and refer patients and families to resources for education and support, as well as outpatient and inpatient healthcare provider directories.
- An Infinite Mind® aninfinitemind.com
- International Society for the Study of Trauma and Dissociation isst-d.org
- International Society for Traumatic Stress Studies istss.org
- National Alliance on Mental Illness—COVID-19 Resource and Information Guide nami.org/Support-Education/NAMI-HelpLine/COVID-19-Information-and-Resources/COVID-19-Resource-and-Information-Guide
- National Alliance on Mental Illness—Dissociative Disorders nami.org/Learn-More/Mental-Health-Conditions/Dissociative-Disorders
- Trauma Disorders Program at Sheppard Pratt sheppardpratt.org/care-finder/the-trauma-disorders-program
- Treatment of Patients with Dissociative Disorders topddstudy.com
Signs and symptoms
DD symptoms include dissociation, depersonalization, derealization, amnesia, and other distressing, intrusive symptoms that impair daily functioning.
Individuals with DDs sometimes describe dissociation as “losing time,” which causes memory gaps that can last minutes to days to years.
Depersonalization causes individuals to feel as though parts or all of their body aren’t real or to feel detached. Individuals frequently describe it as having an out-of-body experience or like watching a movie of themselves.
Derealization causes things and people in one’s environment to feel unfamiliar or unreal. Individuals with DDs may not recognize their own apartment or their friends and acquaintances.
Amnesia refers to significant memory impairment above and beyond normal forgetfulness, such as forgetting one’s wedding, home address, the birth of a child, or the purchase of a new car. Related to amnesia, a dissociative fugue occurs when individuals find themselves having traveled to another location, such as another city or state, with no memory of how they arrived or who they are.
These distressing symptoms lead to high rates of self-harm (cutting, burning, scratching, hair-pulling, headbanging) and suicide. For example, according to the DSM-5, over 70% of individuals with dissociative identity disorder (the most extreme manifestation of DD) attempt suicide as outpatients.
Many individuals with DDs feel intense shame and may not be forthcoming about their symptoms. You can build trust and rapport using therapeutic communication skills and trauma-informed considerations, such as refraining from touching a patient without permission. During your assessment, you may notice confusion and disorientation related to dissociation and memory impairment. Patients typically struggle with emotion regulation, so you may see mood lability, including patients who are emotionally numb and detached, as well as those who are overwhelmed and emotionally flooded. Individuals with DDs frequently experience distorted thinking, so you may notice intense negative self-talk (I’m not good enough, I deserve to get hurt, I’m stupid) and low self-esteem. Patients may report difficulty with flashbacks, nightmares, pain and various somatic symptoms, and intense feelings of shame, guilt, and worthlessness. Sensitively assess patients for evidence of self-harm and continued abuse. Look for open wounds, bruises, broken bones, and other injuries.
Nursing interventions
After a thorough assessment, you can help individuals with DDs manage their symptoms and maintain safety. To mitigate dissociation and flashbacks, reorientation to the present can be achieved by encouraging the patient to use their five senses to ground themselves in the current moment. For example, encourage patients to look around and name objects in their environment or offer them a cold, flavored drink. Pointing out the date and time on a clock, calendar, or current newspaper is a useful orienting strategy.
Promote emotion regulation and help patients manage anxiety and agitation by teaching techniques such as deep breathing, therapeutic journaling, and progressive muscle relaxation. DDs fundamentally disrupt the mind–body connection, so you can provide education and resources related to meditation, mindfulness, and yoga to help patients improve interoception (perception of sensations inside the body).
Healthy sleep hygiene can be problematic for patients who experience hypervigilance and nightmares, so discuss nonpharmacologic methods to promote sleep, such as listening to soothing music, using calming aromatherapy, avoiding caffeine and vigorous exercise in the evening, and reducing late-night screen time.
Pain is the most commonly experienced symptom of survivors of child abuse. Offer nonpharmacologic pain management options, including heat or cold, stretching and repositioning, and guided imagery.
The high risk for self-harm and suicide in this population requires a careful safety assessment. Survey the environment and remove any objects (ligature risks and sharp objects) that pose a safety threat. For patients in acute crisis, stay with them until the crisis is resolved and imminent safety concerns have passed, or until they can receive a higher level of observation and care. (See Educational and support resources.)
Treatments
Psychotherapy is the gold standard for treating DDs. Outpatient treatment can continue for many years. In addition to individual therapy, group therapies like cognitive behavioral therapy and dialectical behavior therapy are useful.
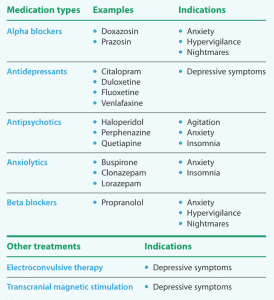
Currently, no drugs are available to treat dissociative disorders as a whole, but a variety of medications can be used as adjuncts to therapy to manage symptoms and improve individuals’ quality of life. Anxiolytics (for example, benzodiazepines) and antidepressants (for example, selective serotonin reuptake inhibitors and serotonin and norepinephrine reuptake inhibitors) can be used to manage mood fluctuations caused by intrusive symptoms, such as flashbacks. The sedating properties of some antipsychotics (such as perphenazine, quetiapine, and haloperidol) can be helpful in managing anxiety, agitation, and insomnia. Alpha blockers (such as doxazosin and prazosin) and beta blockers (such as propranolol) are useful in managing nightmares and hypervigilance. Teach patients and families about these medications and monitor for effectiveness, side effects, and adverse reactions.
Electroconvulsive therapy and transcranial magnetic stimulation have been shown to be effective in relieving depressive symptoms within this population. Occasionally, intensive inpatient psychiatric treatment is required to achieve basic safety and stabilization. (See Dissociative disorder treatment.)

Dissociative disorder treatment
Similar to many mental illnesses, no cure for dissociative disorders exists. In addition to individual and group psychotherapy, the following treatments can help individuals manage intrusive symptoms and improve their quality of life.
Take the opportunity
The mental health needs of the general population are growing. Nurses must be vigilant in assessing for the possibility of DDs and other mental illnesses. You have the opportunity to provide life-saving resources and support to individuals and families affected by DDs.
References
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Washington, DC: American Psychiatric Publishing; 2013.
Boon S, Steele K, van der Hart O. Coping with Trauma-Related Dissociation: Skills Training for Patients and Therapists. New York City, NY: W.W. Norton & Company; 2011.
Brand BL, Schielke HJ, Putnam KT, et al. An online educational program for individuals with dissociative disorders and their clinicians: 1-year and 2-year follow-up. J Trauma Stress. 2019;32(1):156-66. doi:10.1002/jts.22370
Brand BL, Webermann AR, Snyder BL, Kaliush PR. Detecting clinical and simulated dissociative identity disorder with the Test of Memory Malingering. Psychol Trauma. 2019;11(5):513-20. doi:10.1037/tra0000405
Haddock DB. The Dissociative Identity Disorder Sourcebook. New York City, NY: McGraw-Hill Education; 2001.
Loewenstein R, Wait, S. The trauma disorders unit. In: Sharfstein S, Dickerson FB, Oldham JM, eds. Textbook of Hospital Psychiatry. Washington, DC: American Psychiatric Publishing; 2008; 103-18.
Myrick AC, Webermann AR, Langeland W, Putnam FW, Brand BL. Treatment of dissociative disorders and reported changes in inpatient and outpatient cost estimates. Eur J Psychotraumatol. 2017;8(1):1375829. doi:10.1080/20008198.2017.1375829
Snyder BL. Women with dissociative identity disorder who experience intimate partner violence. J Psychosoc Nurs Ment Health Serv. 2018;56(5):26-32. doi:10.3928/02793695-20180212-06
Steinberg M. Structured Clinical Interview for DSM-IV Dissociative Disorders, Revised (SCID-D-R). Washington, DC: American Psychiatric Association; 1994.
van der Kolk BA. The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma. New York City, NY: Viking; 2015.
Briana L. Snyder is an assistant professor in the department of nursing at Towson University in Towson, Maryland, and a per diem RN at Sheppard Pratt Hospital in Towson.
















