
A clinical judgment model and rubric
- Clinical judgment is declining in new graduate nurses, adversely affecting patient safety, liability, and quality care outcomes.
- Mentors should coach and evaluate clinical judgment in new graduate nurses using the Tanner Clinical Judgment Model and Lasater Clinical Judgment Rubric.
- The Mentor’s Clinical Judgment Coaching Tool guides new graduate nurses’ clinical judgment development.
Learning Objectives
- Explain the cognitive processes that form clinical judgment in Tanner’s Clinical Judgment Model.
- Describe the Mentor’s Clinical Judgment Coaching Tool questions and evaluation strategies.
- Describe coaching strategies that can help develop clinical judgment.
No relevant financial relationships were identified for any individuals with the ability to control content of the activity.
Expiration: 2/1/28
Ongoing research by Kavanagh and colleagues shows a decline in new graduate nurses’ clinical judgment. Less than 10% of new graduate nurses possess safe clinical judgment skills, 40% fail to recognize a patient’s urgent problem, and 50% don’t intervene appropriately. A study by the National Council of State Boards of Nursing revealed that 65% of new graduate nurses don’t notice a patient’s clinical deterioration and respond, and 50% of all medication errors arise from poor clinical judgment. Due to increasing patient safety concerns, the Next Generation NCLEX (NGN) evaluates clinical judgment.
New nurses and clinical judgment
New graduate nurse time management
Quality patient outcomes depend on sound clinical judgment. A systematic review by Burke and colleagues showed that many factors result in a failure to rescue, which leads to adverse patient outcomes. Those relevant to clinical judgment fall under three categories: lack of recognition, lack of proper communication, and lack of proper intervention. A study by Callihan and colleagues demonstrated that a breakdown in clinical judgment processes—noticing, interpreting, responding, and reflecting—among experienced emergency department nurses adversely affected patient outcomes. Failure to provide safe care has legal and ethical ramifications.
Precepting vs mentoring
The complex healthcare environment requires critical thinking, a prerequisite for clinical judgment. However, a large study by Zahner and colleagues of 50,000 nursing and non-nursing graduates revealed that only 47% had adequate critical thinking skills; 23% lacked those skills. Several factors result in declining clinical judgment in new graduate nurses, including ineffective mentorship and coaching.
Effective mentorship plays a crucial role in ensuring patient safety while new nurses develop clinical judgment skills. The terms “preceptor” and “mentor” sometimes are used interchangeably, but the American Psychiatric Nurses Association distinguishes between these roles. A preceptor orients a new graduate nurse to the clinical facility. A mentor is an experienced nurse who maintains a long-term relationship with a new nurse via coaching and evaluation to assist in professional development. Mentoring promotes patient safety, and Tanner’s Clinical Judgment Model can serve as a framework for developing these vital skills. (See Tanner’s Clinical Judgment Model.)
Tanner’s Clinical Judgment Model
Tanner’s model describes how expert nurses use clinical judgment.
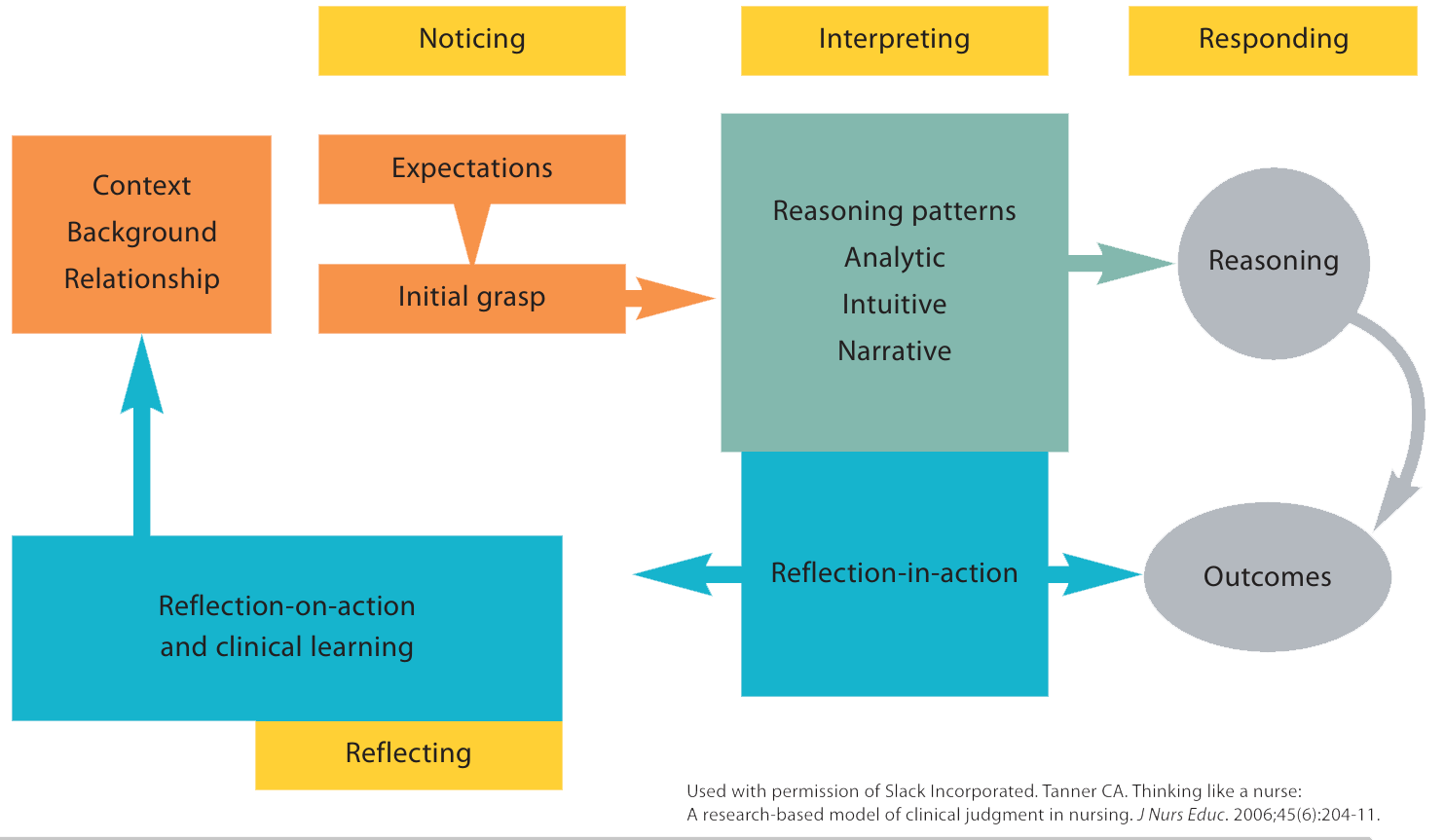
Tanner’s Clinical Judgment Model
Christine Tanner developed the Tanner Clinical Judgment Model in 2006 based on decades of research by many researchers, dating from 1950 through the 1970s. The National Council of State Boards of Nursing Clinical Judgment Measurement Model, which the NGN is based on, incorporates the Tanner model. According to a national survey by Jessee and colleagues, the Tanner Clinical Judgment Model is the most frequently used model to teach clinical judgment. It describes four processes of expert clinical judgment: noticing, interpreting, responding, and reflecting.
The model’s importance to nursing lies in its description of nurses recognizing a patient’s deterioration and acting appropriately to provide safe care. It can help new graduate nurses develop foundational clinical judgment, which enables them to recognize changes in their patients and intervene appropriately. However, new graduate nurses think slowly and methodically rather than quickly and intuitively. Nielsen recommends coaching strategies to develop clinical judgment based on Tanner’s model. (See Coaching strategies.)
Coaching strategies
Tanner’s Clinical Judgment Model incorporates the following coaching strategies:
- Advising
- Discussion
- Examples
- Feedback
- Reflection
- Role modeling
- Questioning
- Thinking out loud
Coaching clinical judgment with new graduate nurses requires a detailed understanding of noticing, interpreting, responding, and reflecting. Although all four processes have a role in patient situations, mentors take advantage of teachable moments to focus on the most appropriate. In clinical practice, nurses use the processes iteratively, going back and forth between them or even temporarily skipping one depending on the patient’s status. Mentors coach within a situated context, which means questions and answers depend on the situation. (See Follow the process.)
Clinical judgment evaluation
 Each section of the Tanner model includes detailed guidance on coaching clinical judgment. The model provides structure to help new graduate nurses organize their thinking and consistent terminology for communication with their mentors.
Each section of the Tanner model includes detailed guidance on coaching clinical judgment. The model provides structure to help new graduate nurses organize their thinking and consistent terminology for communication with their mentors.
New graduate nurse clinical judgment development requires evaluation. The Lasater Clinical Judgment Rubric for evaluating clinical judgment serves as a valid and reliable resource aligned with the Tanner model. Lasater developed the rubric in 2007 for use in high-fidelity simulation with nursing students, but Nielsen and colleagues successfully used it with new graduate nurses.
Using the Lasater rubric, mentors can track new graduate nurses’ progress and provide objective feedback that describes them as beginning, developing, accomplished, or exemplary within each of Tanner’s clinical judgment processes. Based on a study by Nielsen, beginning and developing nurses require intensive coaching to achieve exemplary level clinical judgment. (See Coaching tool.)
Noticing
Noticing involves more complex reasoning than merely performing an accurate complete assessment. A nurse should recognize the most important cues that stand out in a patient situation. Noticing is based on the nurse’s knowledge and experience combined with understanding an individual patient. Influencing factors include the type of healthcare facility, clinical specialty, sociocultural context, personal values, and practice standards. Because a nurse’s background influences their noticing, mentors ask new graduates about their nursing experience to build on prior learning.
According to Caputi, a mentor coaches new graduate nurses to scan the patient’s room for unsafe situations. For example, the mentor coaches the new nurse to take one minute when they enter the room to view the overall patient presentation, equipment, bed, and floor to notice problems such as a leaking I.V. catheter, an empty I.V. fluids bag, lowered side rail, disconnected oxygen tubing, or a saturated dressing.
A mentor coaches noticing before or after the new nurse performs an assessment. Before entering the room, they ask which body systems the nurse should assess and why. After the assessment, the mentor points out subtle changes that differ from the expected. For example, vague patient complaints, small changes in skin color or moisture, a changed vital sign, or altered mental status. The mentor and nurse discuss subtle changes within the context of the patient’s situation; without context, changes lack meaning.
Because new graduate nurses feel overwhelmed and lack extensive experience, they can overlook important information. Therefore, the mentor coaches the new nurse to adapt the assessment based on the emerging situation. For example, if a patient with a cardiac issue develops difficulty breathing but the new nurse remains focused on taking a blood pressure, the mentor can use this teachable moment to call attention to the unrecognized cue.
Successful coaches frequently ask new nurses to think out loud. This strategy helps the mentor understand how the nurse thinks so they can provide insights for improvement. Mentors can use thinking out loud for any phase of the Tanner model.
Lasater evaluation. The Lasater Clinical Judgment rubric describes three characteristics of exemplary noticing: a focused assessment based on the context, adjusted assessment based on unexpected findings and subtle cues, and additional information gathered by talking with the patient and family.
Interpreting
Interpreting refers to analyzing the patient’s information and identifying the priority problem. According to Caputi, mentors coach new graduate nurses to compare changes across time, sort through information to distinguish the important from the unimportant, cluster information around a concept or body system to build a case for a suspected patient problem, and determine the patient’s priority problem or potential complication. The mentor asks the new graduate nurse why they think patient findings are significant and how their significance supports the identified problem.
Situational awareness, a component of clinical judgment, describes a nurse’s ability to recognize a patient’s deterioration and respond in a timely and appropriate manner. Essential components of situational awareness include recognizing signs that indicate a patient is deteriorating, understanding the meaning of those signs, and knowing what will happen to the patient without rapid intervention. According to a study by White, teaching nursing students to look for specific signs of deterioration and initiate the setting’s protocol promotes patient safety.
Laster evaluation. Two characteristics indicate exemplary interpreting: The new graduate nurse determines which patient information is most important and most relevant and they determine the information’s meaning. To make meaning of the information, the new graduate nurse looks for patterns in information, clusters related information, compares the information to a reliable source (such as the literature or the mentor’s experience), and develops a strategy to stabilize the patient.
Responding
Responding involves nursing actions with sound rationales. Mentors coach new graduate nurses on indicated, contraindicated, and preventive nursing actions based on the context of the patient situation. The mentor also questions the nurse about the expected outcomes of planned interventions. If the patient doesn’t respond as anticipated, the mentor coaches the nurse to consider why and then adjust their actions accordingly.
In addition, the mentor coaches the new graduate nurse to think through the consequences of failing to assess and intervene by asking “what if” questions. Thinking through these scenarios out loud enables the nurse to rehearse clinical decision-making through mental role-play. This mental activity (metacognition) helps new nurses to “think about their thinking” and provides insights into their clinical judgment.
Mentors can role model good communication via patient and caregiver education as well as through calm reassurance and explanations to the patient and family. The mentor also explains the roles of team members and the principles of safe, efficient delegation.
Lasater evaluation. Four criteria describe exemplary responding: appropriate delegation; professional communication with patients, families, and the interdisciplinary team (calm confidence; thorough, clear, and accurate directives; evaluation of outcomes); appropriate interventions within the given situation and adjustments based on the patient’s response; and excellence in skill selection and performance.
Reflecting
Reflection-in-action and reflection-on-action play a role in clinical judgment coaching. In reflection-in-action, the new graduate nurse reassesses the effectiveness of their actions until the patient stabilizes. The mentor coaches this skill by discussing the expected outcome for the specific patient and what the nurse should anticipate as an outcome of their care. The mentor asks the nurse whether the patient improved and which assessment findings they used to make that determination.
Reflection-on-action involves two processes after patient care ends: debriefing and reflection. Using the evaluation questions from the Mentor’s Clinical Judgment Coaching Tool, the mentor debriefs with the new graduate nurse immediately after a patient encounter. Debriefing allows the nurse to learn from experience which interventions will likely work in similar future situations. The nurse also should determine how they can improve in similar situations by considering, along with a rationale, what they would do differently. As the nurse develops specific goals for improvement, the mentor should help the nurse evaluate their progress.
Reflection, a long-term self-evaluation activity, involves periodic discussions with the mentor. Maintaining a reflection journal can help new graduate nurses establish a habit of self-reflection. Monagle and colleagues recommend using the Lasater Clinical Judgment Rubric as a guide for reflection journals. The nurse should select nursing experiences in which they believe they used clinical judgment and write a reflection entry based on the evaluation criteria in the rubric. The nurse should provide thoughtful, detailed, and honest evidence that supports whether they met the rubric criteria.
The mentor then discusses the entries with the nurse. In the study by Monagle and colleagues, new graduate nurses met as a coach-led group 1 to 3 months after graduation for training in clinical judgment, use of the Lasater rubric, and reflective journaling. The group met again to discuss their self-reflection at 5 to 7 months and 10 to 12 months post-graduation. Clinical judgment development takes time, so the mentor and new nurse may not notice insight into certain aspects of the rubric until a year after graduation.
Benefits of reflection journaling, based on the Monagle and colleagues study, include new nurses’ noticing missing details in a patient’s emerging situation, wishing they had intervened earlier, lack of confidence inhibiting nursing actions, and lack of knowledge to make clinical decisions. Based on these findings and because clinical judgment develops over time, a new graduate nurses’ group could continue meeting after 1 year.
Lasater evaluation. Two criteria denote exemplary reflecting: The new graduate nurse self-evaluates key decision points throughout Tanner’s four clinical judgment processes and considers the potential effectiveness of alternative options. They also acknowledge their strengths and weaknesses and enact a specific plan for professional improvement.
Ongoing professional development
Clinical judgment requires experience and mentoring. Mentors use their expertise and the Mentor’s Clinical Judgment Coaching Tool to coach and evaluate clinical judgment. Using the Tanner Clinical Judgment Model and Lasater Clinical Judgment Rubric throughout a healthcare organization can help standardize terminology, coaching, and evaluating. Organizations can provide mentor training via workshops, online continuing education modules, or a mentoring certification course. In addition, organizations can incorporate the Tanner model and Lasater rubric into new graduate nurse orientation before the nurses receive a mentor.
Published internal research that monitors new graduate nurses’ clinical judgment development associated with patient safety can contribute to the nursing profession and provide further impetus for ongoing professional development in clinical judgment. Since acquiring expert clinical judgment takes years, all healthcare organizations should set continuing professional development on this subject as a goal to increase safety, decrease liability, and improve high-quality outcomes.
The authors work at the University of Alabama Capstone College of Nursing in Tuscaloosa. Carolyn Kerns is an assistant professor and Monika Wedgeworth is an associate professor.
American Nurse Journal. 2025; 20(2). Doi: 10.51256/ANJ022506
References
American Nurses Association. Nursing: Scope and Standards of Practice. 4th ed. Silver Spring, MD: American Nurses Association; 2021.
American Psychiatric Nurses Association. APNA guidance regarding precepting and mentorship. April 2022. apna.org/resources/apna-guidance-regarding-precepting-and-mentorship
Burke JR, Downey C, Almoudaris AM. Failure to rescue deteriorating patients: A systematic review of root causes and improvement strategies. J Patient Saf. 2022;18(1):e140-55. doi:10.1097/PTS.0000000000000720
Callihan ML, Wolf L, Cole H, et al. Determining clinical judgment among emergency nurses during a complex simulation. J Emerg Nurs. 2023;49(2):222-35. doi:10.1016/j.jen.2022.11.010
Caputi L. Think Like a Nurse: The Caputi Method for Learning Clinical Judgment. Chicago, IL: Windy City Publishers; 2022.
Dickison P, Haerling KA, Lasater K. Integrating the National Council of State Boards of Nursing Clinical Judgment Model into nursing educational frameworks. J Nurs Educ. 2019;58(2):72-8. doi:10.3928/01484834-20190122-03
Gonzalez L, Nielsen A, Lasater K. Developing students’ clinical reasoning skills: A faculty guide. J Nurs Educ. 2021;60(9):1-10. doi:10.3928/01484834-20210708-01
Hensel D, Billings DM. Strategies to teach the National Council of State Boards of Nursing Clinical Judgment Model. Nurs Educ. 2020;45(3):128-32. doi:10.1097/NNE.0000000000000773
Jessee MA, Nielsen A, Monagle J, Gonzalez L, Lasater K, Dickison P. A national report on clinical judgment model use in prelicensure nursing curricula. Nurs Educ Perspect. 2023; 44(1):4-10. doi:10.1097/01.NEP.0000000000001062
Jessee MA. An update on clinical judgment in nursing and implications for education, practice, and regulation. J Nurs Reg. 2021;12(3):50-60. doi:10.1016/s2155-8256(21) 00116-2
Kavanagh JM, Sharpnack PA. Crisis in competency: A defining moment in nursing education. Online J Issues Nurs. 2021;26(1):1-11. doi:10.3912/OJIN.Vol26No01Man02
Kavanagh JM, Szweda C. A crisis in competency: The strategic and ethical imperative to assessing new graduate nurses’ clinical reasoning. Nurs Educ Perspect. 2017;38(2): 57-62. doi:10.1097/01.Nep.0000000000000112
Lasater K. Clinical judgment development: Using simulation to create an assessment rubric. J Nurs Educ. 2007;46(11):496-503. doi:10.3928/01484834-20071101-04
Monagle JL, Lasater K, Stoyles S, Dieckmann N. New graduate nurse experiences in clinical judgment: What academic and practice educators need to know. Nurs Educ Perspect. 2018;39(4):201-7. doi:10.1097/01.NEP.0000000000000336
Nielsen A, Lasater K, Stock M. A framework to support mentors’ evaluation and development of new nurses’ clinical judgment. Nurs Educ Pract. 2016;19:84-90. doi:10.1016/j.nepr.2016.03.012
Reebals C, Wood T, Markaki A. Transition to practice for new nurse graduates: Barriers and mitigating strategies. West J Nurs Res. 2022;44(4):416-29. doi:10.1177/0193945921997925
Tanner CA. Thinking like a nurse: A research-based model of clinical judgment in nursing. J Nurs Educ. 2006;45(6):204-11. doi:10.3928/01484834-20060601-04
Van Damme D. Do higher education students acquire the skills that matter? In: Van Damme D, Zahner D, eds. Does Higher Education Teach Students to Think Critically? Paris, France: Organisation for Economic Co-operation and Development Publishing; 2022:18-38. doi:10.1787/cc9fa6aa-en
White A, Maguire MBR, Branna J, Brown A. Situational awareness in acute patient deterioration. Nurs Educ. 2021;46(2):82-6. doi:10.1097/NNE.0000000000000968
Zahner D, Cortellini O, Rotholz K, Dawber T. CLA+ in the United States. In: Van Damme D, Zahner D, eds. Does Higher Education Teach Students to Think Critically? Paris, France: Organisation for Economic Co-operation and Development Publishing; 2022:142-159. doi:10.1787/cc9fa6aa-en
Key words: clinical judgment, new graduate nurses, preceptors, mentors, Tanner’s Clinical Judgment Model, Lasater Clinical Judgment Rubric


















2 Comments. Leave new
I really enjoyed this article! As a long-time nurse and healthcare educator, I can truly relate to how vital effective mentoring is in helping new nurses feel confident and ready to care for patients independently. Kudos to my early mentors in the 70s who guided me with patience and wisdom, even though we didn’t have the structured evaluation tools that are available today. This article highlights the value of strong coaching and the need for ongoing professional development to support safe, high-quality care.
This was a great article for a new nurse graduate like myself. Very helpful information