

A framework of discernment can aid decision-making.
- Nurses in all roles and specialties are questioning whether it’s time to stay or go.
- A tendency exists to abruptly decide to leave without sufficient discernment.
- Nurses can apply a model for determining whether a marriage can survive to their discernment process.
- Questions that inform the discernment process can support nurses to make integrity-preserving decisions that they can live with.
The challenge
Many nurses continue to struggle with the decision of whether to stay or leave. However, the specifics of that struggle vary depending on your role within the profession.
Re-imagining nursing’s social contract with the public
Nurses at the point of care
During the pandemic, nurses at the bedside experienced feelings of betrayal when asked to assume additional risk to their own and their family’s health as they cared for those in need. At the same time, fluctuating policies governed the allocation of scarce resources, including personal protective equipment (PPE), which required clinicians to re-use masks beyond their effectiveness.
New patterns of care delivery arose because of PPE scarcity, resulting in fewer people being permitted in isolation rooms. In most cases, nurses remained in direct contact with patients diagnosed with COVID-19, while families and other members of the team, including physicians, looked on from outside the isolation room windows. Nurses accompanied dying patients in their final hours, frequently without their families present.
Healthcare organization leaders
Frontline workers weren’t the only ones to suffer during the pandemic. Leaders entered crisis management mode, forced to allocate scarce resources and balance multiple commitments to patients, staff, governing boards, and the broader community. They suffered in ways invisible to many of those delivering care.
Some in leadership positions found their skills challenged or outmatched. Acting on incomplete or inaccurate information, they made and re-made decisions as more data became available. Leaders assumed that those employed in their organizations would show up to serve the needs of the community—because “that’s what they signed up for.”
Watching their coffers deplete as they tried to keep the ship afloat, some leaders acknowledged staff efforts with pizza parties and public expressions of gratitude. Although well-intentioned, communication frequently became transactional and divisive as leaders attempted to guide their organizations through an unprecedented crisis. Rather than acknowledging fear and uncertainty with empathy and understanding, many leaders responded to the pressure by adopting a command-and-control style of communication with limited opportunities for relational engagement.
The pandemic created a threshold moment for nurses and the organizations in which they practiced. Determining whether those relationships can be healed and improved or should be ended requires more than raw emotion, pent-up grievances, or reaction.
Parallel decision-making: Nursing and marriage
The commitment nurses make to their patients, their profession, and the healthcare system is similar to the oath a person makes at the marriage altar. When nurses graduate and become licensed, they commit to upholding the standards and ethical values of the profession.
The healthcare organizations where they practice make implicit and explicit commitments to provide the necessary resources, infrastructure, and leadership to enable nurses to practice in accordance with their code of ethics, regulatory and legal mandates, and standards of practice. Healthcare organizations commit to on-boarding, orientation, preceptorships, nurse residency programs, and other systems to support nurses’ competence and professional development.
At the beginning of their careers and in their first positions in healthcare organizations, nurses serve as hopeful and generous problem-solvers. They’re willing to overlook the blemishes of their jobs or profession because the benefits of seeing patients heal, the appreciation from patients and their families, and the professional development outweigh the burdens.
All relationships have their ups and downs, including those between nurses and healthcare systems. Like newlyweds, they may have entered the profession with a naïve clarity of purpose and commitment. After the honeymoon, they begin to see the situation with greater accuracy and perhaps invest in additional skills and tools to improve their relationships and well-being in service of their ultimate purpose and goals.
Rarely does this process follow a straight line, but sufficient professional and personal benefits and positive outcomes accrue when a nurse remains in the job or in the profession, especially if they can re-invent themselves and recalibrate their expectations to find the right fit within the profession and the wider community. Over time, innocence evolves into a more mature and balanced appraisal of the field and employers.
However, periods of disillusionment remain in which they sense a lack of appreciation and respect—they feel taken for granted. Some nurses find that their healthcare organization has leveraged their commitment to patients to wrest greater effort from them. In the extreme, they may feel that the organization sacrifices their welfare to maintain a functioning system. For most nurses, that recognition represents an unfortunate but usually tolerable aspect of the relationship, because they derive sufficient benefit from the nature of their service.
In the past, these affronts typically occurred episodically with periods of intensity balanced by reward or progress. The pandemic, however, precipitated a crisis of faith and commitment. Just as cumulative disengagement, infidelity, or domestic violence challenge the marital vow, the pandemic has driven many nurses to ask the question, “Can this marriage be saved?” They may wonder, “Do I still belong in this profession or this job? Am I being respected and valued? Are commitments being honored? Does anyone care?”
Just as useful parallels exist between partners contemplating whether they can salvage their marriage and nurses discerning if their relationship to their employer or profession is likely to create a mutually beneficial future, leaders and organizations also may reassess their commitment to frontline staff. They may question whether they’ve achieved a sufficient return on their investment.
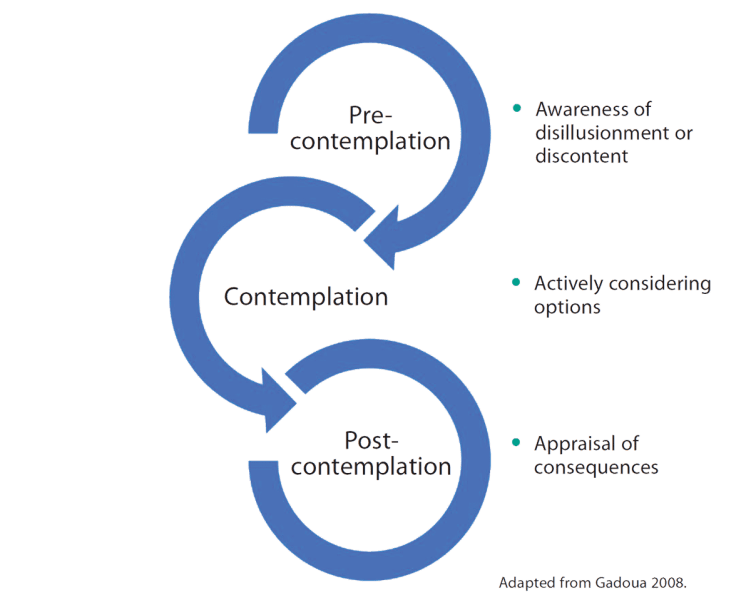
As is true in marriage, few professional relationships end in a precipitous and certain fashion. Instead, as Gadoua describes, one or both partners in a marital or professional relationship transition through a continuum from precontemplation through post-contemplation, with each stage holding defining questions and pitfalls.
A framework for discernment
Gadoua’s model, developed to assist couples in assessing the viability of their marriage, can serve as a template for a nurse’s discernment process. The model includes three stages: pre-contemplation (awareness of disillusionment or discontent), contemplation (actively considering options), and post-contemplation (appraisal of consequences). Nurses, especially those who served during the pandemic, may wonder if they still belong in their healthcare organizations or even in the profession. Many ask, “Should I stay or leave?” Reina and Reina note that the instigator of this question may be a single incident or a cascade of small and large betrayals that erode trust. (See Stages of discernment.)
Stages of discernment
Nurses can apply three stages of discernment when considering whether to stay or leave their organization or the profession.
Pre-contemplation
In pre-contemplation, partners hold the vague notion that something has changed or that something is wrong in the marriage. The infatuation has ended. One or both partners feel dissatisfied but can’t name its source. They have no compulsion to act dramatically. When they do act, they make gentle or incremental interventions, looking to resources and solutions within the marriage.
Pre-COVID, many nurses lived in this state for years, periodically dissatisfied and discontented but never questioning the commitment they’d made to their patients, their organization, or their profession. If nurses advocated for change, it was from within. They accepted the challenges. Driven by commitment to their patients and a desire to make the system work, nurses have contributed to their own exploitation by the system, creating workarounds, abandoning their own needs, and filling organizational gaps to keep everything functioning.
Healthcare organizations and their leaders have questions about staff engagement as they attempt to stop the nurse exodus. Organizations and leaders may feel betrayed by the nurses they invested in and gave opportunities to, who then resigned before the organization captured its return on that investment. Some leaders may believe that the investments they made in addressing nurses’ concerns went unacknowledged and unappreciated or that extra compensation or other perks should be enough. They may defend their policies and decisions as necessary to remain solvent amid unprecedented clinical and fiscal challenges.
Contemplation
In contemplation, at least one of the partners actively considers leaving the marriage. This stage is defined by indecision, a distressing state in its own right. Frequently, individuals feel thrust into contemplating divorce by a fundamental betrayal, such as infidelity or abuse. Remarkably, even these events seldom result in a quick split. In this phase, the blinders are removed and one or both partners seek to understand the dynamic that brought them to this point. They articulate betrayals, large and small; experience high emotions; and sense the inevitable presence of fear. The partners may overtly or covertly acknowledge transgressions with varying degrees of volume and intensity.
Signals of distress
As signals of the costs of the fracture in the relationship begin to emerge, physical, emotional, spiritual, and moral consequences become evident. This stage is characterized by a vacillation between acting on the decision to leave and embracing any hint of progress as a reason to stay, at least until another threshold moment arrives. Each subsequent moment leads to a new cycle of contemplation, in which the partners reassess the benefits and burdens of staying or going. (See Signs of distress.)
Signs of distress
Consequences of a broken relationship may include physical, emotional, spiritual, and moral distress.
Physical
- Fatigue
- GI distress
- Immune dysfunction
- Insomnia
- Muscle aches
- Weight changes
Cognitive
- Cognitive rigidity
- Compartmentalization
- Confusion/brain fog
- Distraction
- Preoccupation/rumination
Emotional
- Anger/outbursts
- Anxiety
- Depression
- Numbing/apathy
- Shame
Spiritual
- Cynicism
- Despair
- Existential crisis
- Loss of faith
- Loss of meaning or purpose
Moral
- Conflicting values
- Erosion of moral identity
- Loss of integrity
- Misplaced responsibility
- Moral outrage
Adapted from the Substance Abuse and Mental Health Services Administration 2023, Rushton 2018, and Yaribeygi et al 2017.
Should I stay or go?
The pandemic catapulted many nurses into actively contemplating departure from a system they felt had betrayed or abused them. Turnover rates, problematic before COVID-19, accelerated during and after. However, just like the struggling partner in a marriage, nurses hesitate, sometimes out of concern for their livelihood, but more frequently and wrenchingly, out of concern for patients, colleagues, or their own families. The fear of acting carries with it confusion, uncertain outcomes, and anxiety. Living in that cycle can feel like an emotional meat grinder, teetering between certainty and ambivalence, hope and despair, determination and helplessness.
Within the contemplation phase, alternating periods of protest/airing grievances and being heard/accommodation can occur, as do periods of disillusionment and re-commitment. Feeling heard and understood fuels hope, making progress seem possible. In the absence of hope, a nurse feels more disillusioned, self-denigrated, and defeated. In extreme circumstances, they begin to feel oppressed and abused by the system. Like a partner in a relationship that involves domestic violence, the abused can come to feel responsible for their own abuse. They may see no way forward.
Vacillation and uncertainty
Living in a state of uncertainty can prove exhausting; it’s tempting to impulsively take the leap just to end the pain or indecision. Many nurses took this path during the pandemic because of frustration with the situations they found themselves in; they saw no opportunity for change or reconciliation. However, some may find it valuable to take a pause, accept the discomfort (for a time), and follow a deliberate path toward a conscious and informed decision.
This pause is essential, not only because so much rides on the decision, but also because the nurse should examine their motivations in making the call. Integrity requires us to examine our values and patterns of action and inaction and to be explicit in the reasons that justify our choices. A deliberative process may reveal new insights and expose areas that make integrity-preserving compromise possible.
Research by Kwasnicka and colleagues indicates that changes made in alignment with an individual’s identity, beliefs, and values and that result in positive events carry greater weight and resilience than decisions made simply to avoid or escape a negative situation. Within this contemplation phase, distinguishing the antecedents of individual anxiety and despair from the systemic contributions to them can prove valuable. This phase requires the ability to live with discomfort, confusion, and uncertainty until the path forward becomes clear.
As crazy-making as the hamster wheel of contemplation may feel for a marital partner, Gadoua points out that limited options exist: stay, separate, or divorce. How each of these choices plays out for the individual nurse has multiple permutations. A parallel process is likely consciously or unconsciously occurring within healthcare organizations and among their leadership.
Weighing options
A nurse can stay in their job and simply trust that things will improve. This isn’t as indefensible as it sounds. With the easing of pandemic caseloads, conditions have improved in many organizations. Rays of hope emerge as some organizations make changes in response to nurses’ concerns. Some leaders actively listen to nurses and involve them in new models of care delivery and decision-making. Nursing organizations have joined to shine a light on the plight of nurses and advocate for systemic change. Leaders have begun investing in nursing salaries and infrastructure.
However, many nurses may be living in the equivalent of a loveless marriage, a partnership without trust, forever waiting for the next shoe to drop. Unreflected optimism has limits as a sustainable strategy, as does feeling paralyzed by fear of the unknown. Inertia has costs, including a pervasive sense of powerlessness, exploitation, and isolation. At worst, a nurse living and working in these circumstances comes to believe that they’re getting what they deserve and that no viable alternative exists. Assessing the full range of options informs the contemplation phase.
Investing in self-stewardship
Throughout the contemplation process, a nurse must invest in self-stewardship to ensure decisions arise from a clear, nonreactive, values-driven foundation rather than from reaction or projection. To do so requires exquisite awareness of who they are, what they stand for, whether their values align, and their personal signals of distress, overload, and dysregulation. From this awareness, as noted by Rushton in 2024, they can turn toward their limitations with compassion rather than judgement and choose healthy and wholesome actions.
Rejecting the belief that they can make others change or that systems will transform quickly and accepting that their integrity isn’t singularly dependent on the decisions of others can help set more realistic expectations. By relinquishing sole responsibility for or accountability to circumstances beyond their control, the nurse can create space for seeing things in new ways.
This may be a juncture at which the nurse should seek support from employee assistance programs or mental health professionals, especially if they notice signs of depression, unremitting fatigue, sustained anxiety, or numbness. Counseling provides a forum in which to monitor the impact of the process of discernment and prepares the nurse to enter a negotiation.
Accessing resources
Nurses can stay and work on the relationship with their organization, using resources inside or outside the system. Inside their organization, nurses can use their voices to bring awareness to the systemic issues that degrade patient care and nurse well-being. Leadership will have difficulty discounting, marginalizing, or individually punishing nurses’ collective voices.
Integrity requires that we use our voice constructively rather than spew anger or intensify alienation. Establishing clear boundaries that reflect core professional values through shared governance and creating accountability mechanisms to monitor the consequences of decisions can begin to empower those who feel voiceless.
Throughout this process, individual nurses must determine their own thresholds of accommodation and determine when they’ve reached or exceeded them and how to respond rather than react. Employee assistance programs, human resources, organizational committees, and mentors can serve as allies to nurses exercising their voice. Effectiveness requires clear processes, norms, and accountabilities honored by all stakeholders.
Processes for change
As nurses change themselves and their attitudes and assumptions, healthcare organizations inevitably change as well. A social ecological approach, as described by Davidson and colleagues, posits that as members of a system change (and maintain that change), all parts of the ecosystem adjust accordingly.
Calls for nurses to focus on and resource themselves frequently are discounted as blaming the victim or giving the healthcare organization a pass. This kind of either/or dichotomy assumes that focusing on either the individual or the system relieves the other of responsibility. Nurses are members of the system as much as the inhabitants of the C-suite. This means frontline nurses and leaders share responsibility for discovering a path forward that preserves everyone’s integrity and well-being. Both sides must be held accountable for enacting sustainable solutions.
Optimally, this stage includes a reconciliation process for determining responsibility for betrayals, misunderstandings, or missteps. Amends or apologies may be necessary. Reconciliation typically requires an outside mediator or consultant. All couples counselors know that treatment success involves both parties entering the setting in good faith, open to the possibility of change rather than using it to justify or cover for a decision already made.
The same standard holds true for any arbitrated process in a healthcare organization. Management and frontline workers must enter the dialogue with a focus on their values, interests, and needs, without cemented positions. Both must listen, and neither can interpret concession as defeat. The facilitator of the process must be a neutral party with no allegiances. This might include an ombudsman, a skilled and trusted internal facilitator, or an external consultant.
Reconciliation and arbitration can prove intense and uncomfortable for both parties, but it offers the possibility of discovering a path previously unforeseen. Concessions by both sides can result in new terms of engagement and relationship. Within healthcare, the most common arbitration occurs via union representation. However, union negotiations are adversarial by nature, and union negotiators focus on advancing the interests of their members rather than those of healthcare organizations or the public they serve. Whether it’s possible to create mutually beneficial outcomes for both parties requires further examination.
Range of choices
Divorcing themselves from their healthcare organization and even from the profession is a legitimate option for nurses. No position or role is worth perpetually compromising fundamental values or depleting one’s life force. Leaving the profession may present a seductive choice because it puts a hard stop to the cycle of pain. It also may serve to express the anger and indignation that’s accumulated over time.
Completing the split may allow the nurse to disassociate from the distress they’ve experienced and witnessed in their patients and colleagues. Departing can feel liberating and empowering. However, similar to dissolving a marriage, divorcing oneself from the healthcare organization or the profession can have a dark side. For many, leaving nursing carries stigma within their community, survivor’s guilt, or a sense of failure. It may rob the nurse of financial stability and disconnect them from the social network that’s buoyed them through hardship. It also can create a disorienting identity crisis and personal or professional instability.
As Gadoua points out, a middle way exists. Nurses, like marriage partners, can separate, either with the hope/intention/plan to return or as a transitional stage toward divorce. For nurses, that might involve transferring to a less stressful position or setting, accepting a time-limited travelling nurse contract, or working in an unrelated field while maintaining their licensure.
Some nurses may find it impossible to view the situation objectively until they’re outside of it. Also, there’s the common wisdom that you can’t be in an authentic and voluntary relationship until you’re willing to live without it. Time away may serve to restore energy, reestablish objectivity, and offer a sense of life outside of healthcare. When a nurse gives themself the space and time to reflect and heal, while keeping their options open for the future, they can preserve and honor the path taken so far. This option doesn’t preclude re-evaluation or returning to questions they’ve considered during this phase.
Post-contemplation
In the final stage, post-contemplation, the nurse has made the call one way or the other and is living with the consequences. They’ve chosen to stay or go, inevitably feeling some mixture of regret and jubilation either way. They may have stayed and committed themselves to actively seek the transformation of the unit, organization, or the system at large into a setting that sustains them. They may have invested in learning new skills to speak up and advocate for their interests or engaged with collective voices within the profession for systemic change. The nurse may have found peace in accepting their own limitations and those of the organization and profession.
Alternatively, the nurse may have decided that it’s best to remove themselves temporarily or permanently from their role or profession. Although it’s best not to make a precipitate decision to end the distress of contemplation, Gadoua warns against a toxic compromise in post-contemplation.
Remaining in a position but simply going through the motions—disengaged emotionally, morally, and spiritually—leads to a purgatory in which the goal moves from service and excellence to survival. Although making this choice is understandable and potentially justified, the consequences for the nurse, their families and colleagues, and for the people they serve can prove significant. It can represent “quiet quitting,” moral disengagement, or presenteeism.
However, a reasoned decision to leave a situation that’s not aligned with who the nurse is and what they stand for can result in an acceptance of the decision, forgiveness, and release. It can allow the nurse to move on without the burden of regret, shame, guilt, or anger. Leaving a job or even the profession can be an integrity-preserving act when it’s approached through a deliberate, committed process. Regardless of the decision, the nurse should accept the consequences and grant themselves permission to move on.
They should anticipate such post-contemplation questions as, “What does it mean to be a nurse now?” and “To whom or what do I belong to now?” Accessing internal and external resources to engage these questions will support the process of creating a new identity and transforming the past into the fuel for the future.
Ask questions
What may prove helpful at this juncture is to determine where in the contemplation continuum you fall and ask yourself a few relevant questions related to each stage. Unpacking this process may reveal opportunities for intervention. (See Questions to ponder.)
Questions to ponder
Depending on which stage of discernment you find yourself, ask the following questions:
Pre-contemplation
- What brought me into nursing? What inspired me?
- What is most important to me in my role as a nurse?
- How will my core values guide my decisions?
- Am I being honest about what I want or need? Am I getting it?
- What would make things better?
- Who or what would need to change for me to be satisfied with my work situation?
- Are my expectations clear, realistic, and attainable?
- Are my boundaries clearly communicated?
- What would be true if nothing ever changed in me or my work setting?
- What resources do I have within myself or in my control that would support me right now?
- What information do I need to understand my situation or choices more clearly?
- What other resources or mentors could I engage as I consider my decision?
Contemplation
- Can I tolerate the distress long enough to make a deliberated decision?
- What additional resources or information do I need to make an informed decision?
- What physical, emotional, cognitive, spiritual, or moral signals am I noticing?
- What additional resources do I need to access to support me in this process?
- To what extent are my values and commitments guiding my discernment? What additional guidance can they provide?
- What will it mean for me if I stay and neither I nor my situation changes?
- Have I surfaced my concerns and exerted sufficient effort in seeking solutions?
- Are my expectations clear, realistic, and feasible?
- Are processes in place to raise issues without retaliation or shame?
- Do channels exist to promote mutual appreciation and commitment?
- Are the parties bringing mutual appreciation and commitment?
- Are the parties bringing mutual energy or investment to the relationship?
- When things go wrong, what processes of mediation and integrity-preserving compromise can I pursue?
- Is management open to substantive change? How would I know?
- What resources, internal and external, might facilitate change?
Post-contemplation
- Can I live with this outcome?
- How were my values and integrity visible in the decision-making process and the decision itself?
- How has my health and well-being been impacted? What do I need to do to be a good steward of my own resources and well-being?
- Have I used all resources open to me? What’s missing?
- What have I sacrificed in this process and what have I gained?
- Have I forgiven myself and others?
- What residual am I taking into my next phase of life and work? What do I need to do to release this?
- Can I stay in the profession and redefine my identity as a nurse?
- Is there another role or profession that I wish to pursue?
- Am I at peace?
Copyright Cynda Hylton Rushton and Weare A. Zwemer.
If none of the stages characterizes you and you’re blissfully content in your life position, you’re in the non-contemplation stage. Don’t do or ask a thing. Celebrate your clarity, commitment, and resolve.
A moment of recalibration
We’re living though a time of profound challenge and change in nursing and healthcare. The physical, emotional, moral, and spiritual injuries experienced by nurses at the point of care during the pandemic and the healthcare system’s struggle to address them have had an indelible impact. The social contract binding nurses to their patients and their organizations has been breached, leaving clinicians disillusioned and distrustful. If the healthcare system fails to renegotiate its relationship to its largest profession, it runs the risk of collapse from vacancies on its units. Individually, nurses will decide whether to hang in or divorce themselves from their organization or from the profession.
Crises are defined by the intersection of distress and opportunity. Honoring one’s health and integrity and serving in the healthcare system don’t have to be mutually exclusive. Using a systematic framework can support nurses in identifying their position in the decision-making process and proceeding mindfully as they weigh the options before them. No course of action is without risk, benefit, and sacrifice; however, some, like quiet quitting, hold little value for anyone.
The entire nursing workforce and the systems where they practice are recalibrating. Remembering what brought them to the profession and holding their moral compass as a guide, nurses can make intentional, integrity-preserving decisions that balance their needs and the demands of the healthcare system they serve. Healthcare organization leaders committed to sustaining the trained nurses they employ must consider parallel actions to create workplaces commensurate with nurses’ commitment to serve patients, families, and communities while honoring their well-being.
Cynda Hylton Rushton is the Anne and George L. Bunting Professor of Clinical Ethics and Nursing at Johns Hopkins University Berman Institute of Bioethics and the School of Nursing in Baltimore, Maryland. Weare A. Zwemer is a licensed clinical psychologist and forensic examiner in Virginia Beach, Virginia.
American Nurse Journal. 2024; 19(12). Doi: 10.51256/ANJ122406
References
Davidson P, Rushton CH, Kurtz M, et al. A social–ecological framework: A model for addressing ethical practice in nursing. J Clinical Nurs. 2018;27(5-6):e1233–41. doi:10.1111/jocn.14158
Fry-Bowers E, Rushton CH. Reimagining nursing’s social contract with the public. Am Nurse J. 2023;18(9):14-20. doi:10.51256/ANJ092314 https://www.myamericannurse.com/re-imagining-nursings-social-contract-with-the-public/
Gadoua S. Contemplating Divorce: A Step-by-Step Guide to Deciding Whether to Stay or Go. Oakland, CA: New Harbinger Publications; 2008.
Kwasnicka D, Dombrowski SU, White M, Sniehotta F. Theoretical explanations for maintenance of behaviour change: A systematic review of behaviour theories. Health Psychol Rev. 2016;10(3):277-96. doi:10.1080/17437199.2016.1151372
Martin B, Kaminski-Ozturk N, O’Hara C, Smiley R. Examining the impact of the COVID-19 Pandemic on burnout and stress among U.S. nurses. J Nurs Regul. 2023;14(1):4-12. doi:10.1016/S2155-8256(23)00063-7
Reina D, Reina M. Trust and Betrayal in the Workplace: Building Effective Relationships in Your Organization. 3rd ed. Oakland, CA: Berrett-Koehler Publishers; 2015.
Rushton CH. Conceptualizing moral resilience. In: Rushton CH, ed. Moral Resilience: Transforming Moral Suffering in Healthcare. Oxford, UK: Oxford University Press; 2018; 125-49.
Rushton C. Self-stewardship: An ethical imperative for nurses. AACN Adv Crit Care. 2024;35(2):193-8. doi:10.4037/aacnacc2024727
Rushton CH. Do I still belong? Am Nurse J. 2023;18(3):48. doi:10.51256/ANJ032348 https://www.myamericannurse.com/do-i-still-belong/
Substance Abuse and Mental Health Services Administration. Warning signs and risk factors for emotional distress. June 9, 2023. samhsa.gov/find-help/disaster-distress-helpline/warning-signs-risk-factors.
Ulrich CM, Rushton CH, Grady C. Nurses confronting the coronavirus: Challenges met and lessons learned to date. Nurs Outlook. 2020;68(6):838-44. doi:10.1016/j.outlook.2020.08
Yaribeygi H, Panahi Y, Sahraei H, Johnston TP, Sahebkar A. The impact of stress on body function: A review.
EXCLI J. 2017;16:1057-72. doi:10.17179/excli2017-480
Key words: nurse turnover, decision-making, integrity















