

Inclusive nursing assessment in a new era of healthcare
- Collecting information about race, ethnicity, sexual orientation, and gender identity is a critical step for building an inclusive and equitable healthcare system.
- Initial nursing assessment is a great opportunity to gather information about race, ethnicity, sexual orientation, and gender identity.
- Nursing assessment can be used as an opportunity for nurses to demonstrate sensibility and sensitivity and to convey messages of caring, health, and inclusion.
Nurses play a prominent role in building equitable healthcare systems that address diversity and inclusion. Collecting information about race, ethnicity, sexual orientation, and gender identity can help organizations and nurses improve care and outcomes. From an organizational perspective, accurate patient data aid inclusive service design, provide insight into areas that require additional services, and inform strategic hiring. From a nursing perspective, awareness about a patient’s race, ethnicity, sexual orientation, and gender identity helps to ensure individualized care tailored to a patient’s unique needs and determine appropriate available services (for example, LGBTQ support care services generally are available to LGBTQ patients only). In addition, nurses gain insight into how the patient’s personal history may shape their healthcare choices and preferences.
In 2021, Park and colleagues outlined issues related to the concepts of race and ethnicity, and problematic ways in which those concepts are used in healthcare settings. Despite challenges, nearly all U.S. healthcare organizations collect data on race and ethnicity. In addition, state and federal governments recommend collecting voluntary information about patients’ sexual orientation and gender identity. For example, rules from the Centers for Medicare and Medicaid Services and the Office of the National Coordinator of Health Information Technology require all electronic health record (EHR) systems certified under Stage 2 criteria of meaningful use to allow patients to record, change, and access their sexual orientation and gender identity data.
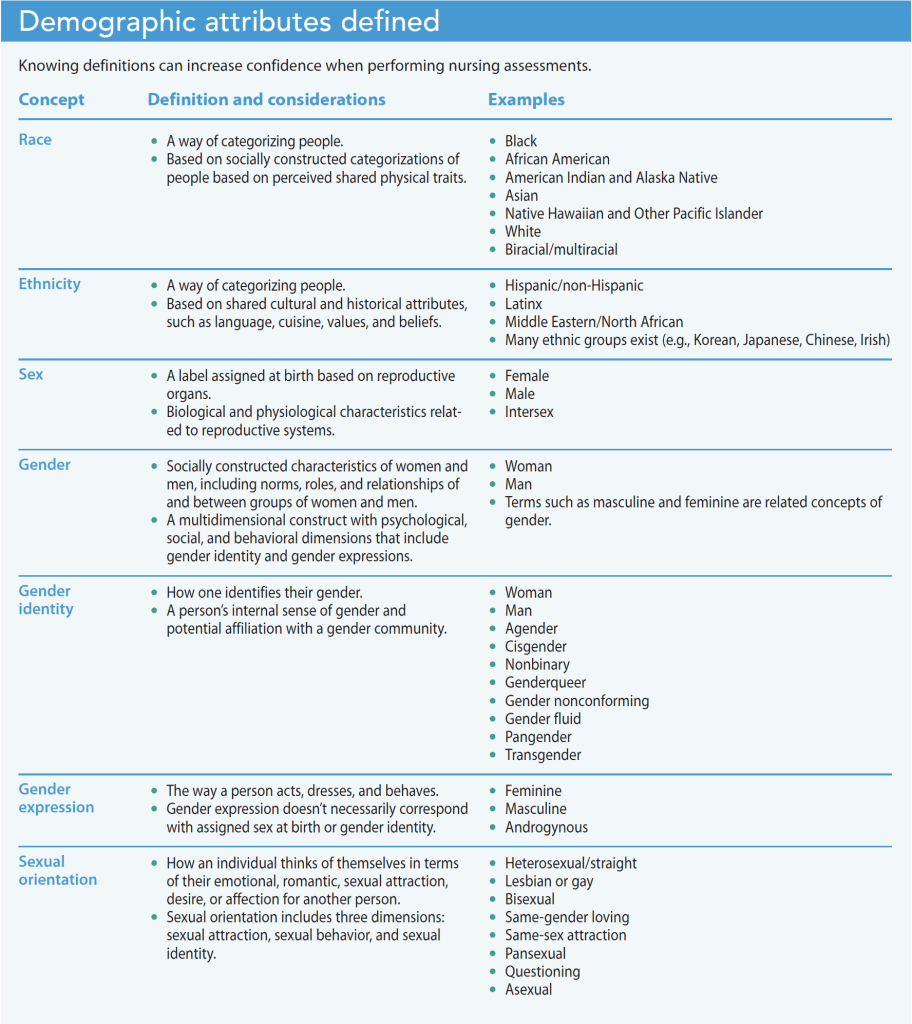
In most cases, nurses are the first healthcare providers patients and their loved ones meet, making initial nursing assessments perfect opportunities to gather information about race, ethnicity, sexual orientation, and gender identity. However, because this information traditionally has been considered private and sensitive, many nurses may feel unprepared to ask about it. In addition, nurses who are unfamiliar with new concepts and terminologies designed to better describe sexual orientations and gender identities may lack confidence. Implementing best practices can help boost nurse self-assurance and ensure this critical information is collected appropriately. (See Demographic attributes defined.)
General considerations
Questions about race, ethnicity, sexual orientation, and gender identity remain sensitive and personal to some patients, so convey a nonjudgmental attitude and a spirit of inclusivity. Before you begin, check the patient’s EHR to see if the information has been collected already.
Data collection policy
Start by examining why you’re asking the questions. Does your organization have a policy about collecting diversity and inclusion data? If so, share it with patients and colleagues. If the policy isn’t available, speak with the public relations department and recommend adding it to the organization’s website.
Patient options and privacy
Ensure that answering questions about gender, race, and sexual orientation is optional and not tied to receiving healthcare services. Health forms should include opt-out options (for example, “Prefer not to disclose” or “Decline to answer”). Ask patients for their permission to include information about race, ethnicity, sexual orientation, and gender identity in their EHR. Information about a patient’s sexual orientation and gender identity are protected under the Health Insurance Portability and Accountability Act (HIPAA). Be prepared to advocate for patients and to protect them by educating yourself about how your organization secures sensitive information, its policy for handling confidentiality breaches, and how to report violations.
Familiarize yourself with patient options for answering questions about race, sexual orientation, and gender identity. If your organization provides online demographic forms, share access information with patients. Some organizations offer mobile devices in the clinic so patients can answer questions privately.
Inclusivity, assumptions, and personal experiences
Be as inclusive as possible. Open-ended questions are the most inclusive way to collect data about race, ethnicity, sexual orientation, and gender identity. Be direct, and ask questions such as, “What is your gender identity?”, “What is your race?”, and “How do you identify your ethnic heritage?”. Ask about each identity separately. Rather than asking “What is your race and ethnicity,” first ask about race and then ask about ethnicity.
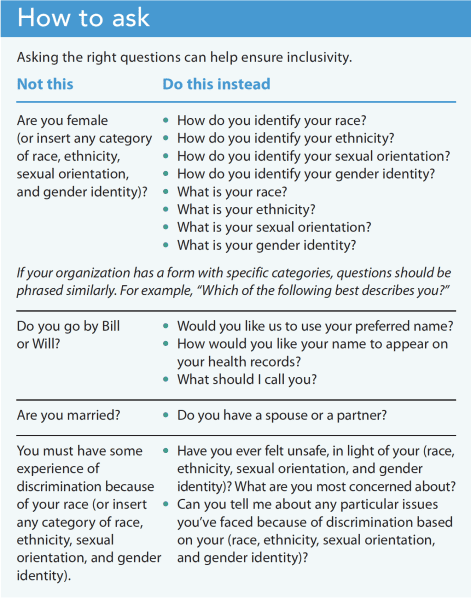
Don’t assume a patient’s race, ethnicity, sexual orientation, or gender identity based on stereotypical mannerisms or characteristics. Never assume that all patients within the same group have similar life experiences or share a common sense of community. Each individual has their own experience and unique perspectives. Explore with patients how their personal experiences related to their race, ethnicity, sexual orientation, and gender identity may have shaped their actions, behaviors, choices, and preferences around health-related issues. (See How to ask.)
Asking about race and ethnicity
Many patients agree that healthcare organizations should document patients’ race and ethnicity, but they may feel more comfortable when they know exactly why it’s being collected. The concepts of race and ethnicity vary significantly, and data collection reflects that. For example, the U.S. Office of Management and Budget (OMB) has set the standard on race and ethnicity data, which other federal organizations, such as the National Institutes of Health and the Census Bureau, follow. The OMB standard includes two categories of ethnicity (Hispanic vs. non-Hispanic), and six categories of race (American Indian or Alaska Native, Asian, Black or African American, Native Hawaiian or Other Pacific Islander, and White). Information on race and ethnicity is gathered in two separate questions to generate different race/ethnicity categories (for example, non-Hispanic White). Under OBM’s definition, individuals who identify themselves as American Indian or Alaska Native, Asian, Pacific Islander, and many European subgroups are ethnically categorized in the non-Hispanic group. Such a simplistic categorization reflects politics around race and ethnicity, rather than a spirit of inclusion and diversity.
In addition, many organizations use different categories of race and ethnicity. For example, the general public may consider Korean, Japanese, and Chinese as ethnic categories, but the OMB considers them racial categories. Such variations may create confusion and discordance across data collected by different organizations.
Considering the wide range of variation in categorizing race and ethnicity, nurses should familiarize themselves with their organization’s standard practice. Before asking patients about their race and ethnicity, review the form your organization uses and become familiar with the racial and ethnic categories included. Assess whether the race and ethnicity categories are broad enough to include the major race and ethnic groups you encounter. Also consider whether biracial/multiracial and multiethnicity options are included.
Examine how questions are phrased and what purpose they may serve. Patients may perceive questions such as “Where were you born?” and “Where are you from?” as proxies for determining immigration status or nativity. Instead ask open-ended questions, such as, “What is your race?” or “How do you identify your race?”
Be sensitive to the fact that some patients may not identify themselves by the categories provided on your organization’s demographic form. Ideally, these forms should include a “None of the above” option with room for the patient to write the categories they think best describe them.
Asking about sexual orientation and gender identity
The debate continues over whether we should ask a person’s sexual orientation and gender identity. For example, the Centers for Disease and Control and Prevention (CDC) describes collecting this information as critical. Without it, the CDC argues, “lesbian, gay, bisexual, and transgender (LGBT) patients and their specific healthcare needs cannot be identified, the health disparities they experience cannot be addressed, and important healthcare services may not be delivered.” Others argue that we must be mindful that collecting information about sexual orientation and gender identity may lead to unintentional consequences, such as improper and unnecessary disclosure of private information (despite HIPAA protections), which may lead to discrimination.
Historically, sexual orientation and gender identity data weren’t part of routine nursing assessments in the United States. This omission may have contributed to health disparities. When questions about sex and gender were asked, they frequently reinforced incorrect beliefs about binary (only men and women) concepts. Sex refers to biological characteristics related to human reproduction, and gender refers to a socio-cultural concept associated with sex. Using sex and gender interchangeably perpetuates erroneous assumptions that all females are women and all males are men. Such assumptions have alienated a segment of the population who don’t identify themselves within this binary.
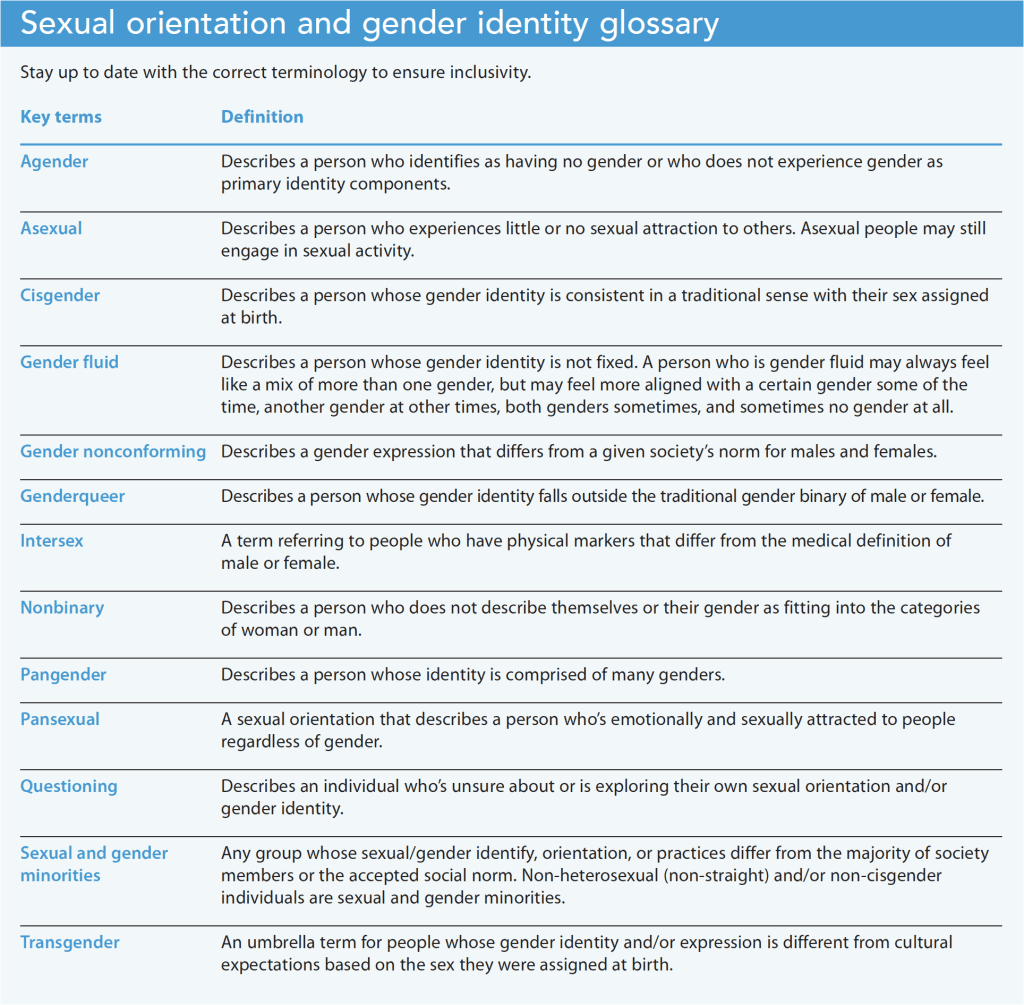
These assumptions have shaped decisions around nursing care, deepening the health inequity among gender and sexual minorities. The phrasing of questions around sex and gender can signal judgment and discrimination, causing unintentional harm. To help ensure inclusion within your organization, review the form used to collect information about sexual orientation and gender identity and reach out to leadership to consider updates based on evolving concepts and definitions. (See Sexual orientation and gender identity glossary.)
Use inclusive language and pose open-ended questions that allow patients to provide their own definitions and descriptions about their sexual orientation and gender identity. Understand that a patient’s sexual orientation and gender identity may be fluid and may change from time to time. Assess whether they continue to identify themselves with the sexual orientation and gender they reported in a previous encounter.
Whenever asking a patient about their sexual orientation and gender identity, reassure them that their information will be kept confidential and that it’s protected under HIPAA.
Caring and healing through inclusion
As nurses we bring our own personal experiences, beliefs, and feelings around race, ethnicity, sexual orientation, and gender identity into our practice. We must examine how they impact our ability to care for patients from diverse backgrounds. If you realize that your personal views may hinder your ability to be the best nurse you can be, seek mentorship to learn how to overcome these challenges, and educate yourself about these topics so that you’re more informed.
Nursing assessment is a process for understanding patients and their health concerns from their perspective. When you approach assessment as an opportunity for discovery, you learn about a patient’s unique circumstances. Nurses meet patients and loved ones at a time of vulnerability, which requires trust to ensure good care. This moment of vulnerability is the precise opportunity for nurses to demonstrate sensibility and sensitivity and to convey messages of caring and healing through inclusion. AN
Mijung Park is an associate professor at the University of California San Francisco School of Nursing.
References
American Psychological Association. APA Guidelines on Race and Ethnicity in Psychology. 2019. apa.org/about/policy/guidelines-race-ethnicity.pdf
Centers for Disease Control and Prevention. Lesbian, gay, bisexual and transgender health. July 25, 2022. cdc.gov/lgbthealth/index.htm
Kiran T, Sandhu P, Aratangy T, Devotta K, Lofters A, Pinto AD. Patient perspectives on routinely being asked about their race and ethnicity: Qualitative study in primary care. Can Fam Physician. 2019;65(8):e363-9.
National LGBTQIA+ Health Education Center. LGBTQIA+ Glossary of Terms for Health Care Teams. lgbtqiahealtheducation.org/wp-content/uploads/2020/02/Glossary-2022.02.22-1.pdf
Office of Management and Budget. Revisions to the standards for the classification of federal data on race and ethnicity. October 30, 1997. obamawhitehouse.archives.gov/omb/fedreg_1997standards
Park M, Alston AD, Washington-Brown L. Toward rational conversation about race, health risk, and nursing. Am Nurse J. 2021;16(1):
5-7;58.
U.S. Department of Health and Human Services. Remarks by HHS Assistant Secretary for Health ADM Rachel Levine for the 2022 Out for Health Conference. April 30, 2022. hhs.gov/about/news/2022/04/30/remarks-by-hhs-assistant-secretary-for-health-adm-rachel-levine-for-the-2022-out-for-health-conference.html
World Health Organization. Gender. who.int/europe/health-topics/gender#tab=tab_1
Key words: nursing assessment, race, ethnicity, sex, gender, sexual orientation, gender identity, inclusive healthcare, diversity, inclusion.












1 Comment. Leave new
Thank you for such an informative article. I will share with my colleagues.