
Every nurse should know about this life-saving maneuver.
- Prone positioning has been a treatment option for acute respiratory distress syndrome in critically ill patients.
- Since the COVID-19 pandemic, awake prone positioning has been utilized as a treatment option for non-intubated patients to improve oxygenation and to help prevent the need for mechanical ventilation.
- Moving patients to the prone position requires a team of caregivers to ensure patient and staff safety.
In 2013, prone positioning—which has been shown to reduce mortality, decrease or prevent lung injury, and improve oxygenation—was written into national and international guidelines as a frontline therapy for patients with ARDS. According to Guérin and colleagues and Mathews and colleagues, before the COVID-19 pandemic, prone positioning was used about 16% of the time to manage patients with ARDS who were mechanically ventilated. COVID-19 led to widespread use of the maneuver as a frontline therapy to reduce mortality.
Making prone positioning a priority
Preventing postoperative pulmonary complications
COVID-19 also led to the implementation of prone positioning with conscious patients not receiving mechanical ventilation to improve oxygenation and prevent or postpone the need for mechanical ventilation. The benefits of awake prone positioning (APP) in patients who don’t have COVID-19 or respiratory failure require additional research. APP, a nurse-led initiative, involves coaching patients into the proper prone position.
For patients who require mechanical ventilation, methods for placing them in the prone position include mechanical assist devices (such as specialized beds or positioners) and manual prone position (via lift assistance, transfer sheet, or linen method).
More about ARDS and prone positioning
ARDS is classified as mild, moderate, or severe based on the degree of hypoxemia and the amount of end expiratory support. The definition includes acute onset, chest x-ray finding, and the presence of non-cardiogenic pulmonary edema. An updated ARDS definition released in July 2023 added patients who require noninvasive ventilation with high-flow nasal oxygenation at 30 L/min with low levels of positive-expiratory end pressure, which can be measured by fraction of inspired oxygen (FiO₂)/oxygenation saturation (SpO₂).
In 2023, the European Society of Intensive Care Medicine guidelines recommended initial mechanical ventilatory strategies to protect the lungs and improve hypoxemia, including low tidal volume ventilation at 4 to 8 mL/kg predicted body weight and prone positioning early in the course of the disease.
Prone positioning involves strategically moving patients from lying on their back and placing them on their abdomen to improve ventilation of the lower portions of the lungs and increase oxygenation. The benefits of prone positioning include improved oxygenation, reduced lung stress, and lowered right ventricular strain. (See Indications and contraindications.)
Indications and contraindications
Nurses should be aware of the following indications and contraindications for prone positioning:
Indications
- Acute respiratory distress syndrome diagnosis with or without COVID-19 after implementation of 12 to 24 hours of mechanical ventilation optimization with lung-protective strategies
- Moderate-to-severe hypoxemia (PaO₂:FiO₂ ratio <150, with FiO₂ >60%, positive expiratory pressure ≥5 cm H₂O, and tidal volume close to 6 mL/kg predicted body weight)
Absolute contraindications
- Goals of care focused on comfort and allowing natural death
- Unstable cervical, thoracic, or lumbar fractures
Relative contraindications
- Acute venous thrombosis treated <48 hours ago
- Advanced arthritis
- Bronchopleural fistula, unstable airway, tracheal surgery within 2 weeks
- Burns >20% of the ventral body surface
- Cardiac abnormalities (life-threatening arrhythmias, ventricular assist devices, intra-aortic balloon pump, extracorporeal membrane oxygenation, fresh pacemaker, recent heart surgery)
- Hemodynamically unstable patient (as defined by systolic blood pressure <90 mmHg or mean arterial pressure <60) with fluid or vasoactive support in place
- Increased intracranial pressure
- Massive bleeding or hemoptysis
- Ophthalmic surgery/increased intraocular pressure
- Pelvic fracture
- Pregnancy (2nd or 3rd trimester) or extremely distended abdomen (padding above and below the distension may offset unnecessary pressure)
- Severe facial injury
- Uncontrolled intracranial pressure or poorly controlled seizures
- Unstable chest wall, open abdomen
- Weight 160 kg or greater (weigh the risk-vs-benefit ratio for patient and caregivers)
Guerin and colleagues conducted a large, randomized control trial of prone positioning in patients with ARDS for 16 to 18 hours per day until it was no longer needed based on inclusion criteria. The patients were randomized within the first 24 to 48 hours of the ARDS diagnosis. Prone positioning demonstrated a significant reduction in 28-day and 90-day mortalities.
In response to COVID-19, providers ordered APP for patients who didn’t require mechanical ventilation. Studies indicate that APP proves beneficial for improving oxygenation and decreasing the need for mechanical ventilation. A meta-analysis performed by Sryma and colleagues reviewed eight studies and concluded that APP is a low-risk, cost-effective treatment option for these patients and could help prevent respiratory failure. Ongoing research will help determine long-term patient outcomes and benefits of APP for patients with non-COVID ARDS.
Ventilated vs non-ventilated prone positioning
Several methods exist for placing patients in the prone position, including the Sheet–Arm Tuck (Burrito) Method, for those receiving mechanical ventilation. For patients who don’t require mechanical ventilation, you can coach them to perform APP.
Mechanically ventilated prone positioning
The American Association of Critical Care Nurses (AACN) Procedural Manual for Progressive and Critical Care describes the step-by-step process for placing patients who require mechanical ventilation into the prone position. (See Manual proning process.)
Manual proning process
The following steps describe how to manually turn a patient to the prone position using the Sheet–Arm Tuck (Burrito) method:
- Verify that at least five healthcare team members are available to assist with the procedure. Add more staff if needed based on the patient’s body habitus and your organization’s patient safety guidelines.
- One team member (usually a respiratory therapist) coordinates the procedure steps and manages the head of the patient, the endotracheal tube, and the ventilator lines.
- At least two team members position themselves on each side of the bed, always maintaining body contact with the bed and acting as side rails to ensure a safe environment.
- If the bed has a low air-loss surface function, maximally inflate the mattress to ease the turn process.
- Remove the patient’s gown and ECG electrodes.
- Place an absorbent pad and a flat sheet on top of the patient from shoulders down. Tuck the patient’s arms tightly against their body and snugly roll the outside of the top and bottom flat sheets together like a burrito.
- Move the patient laterally away from the ventilator while the respiratory therapist monitors the patient’s airway and head; move on the therapist’s count.
- Under the guidance of the respiratory therapist, turn the patient to the full side-lying position, facing the ventilator.
- The team furthest away from the ventilator (delivering team) pulls the flat sheets under the patient while the team closest to the ventilator (receiving team) lowers the patient into the prone position.
- Ensure that ventilator tubing is free of any kinks and secured per your organization’s guidelines.
- Apply ECG electrodes to the patient’s back.
- Ensure the patient is centered in the bed.
- Place offloading devices or pillows under the head, chest, and pelvic area to support proper body alignment and pressure relief.
- Correctly position all tubes, drains, and lines. Resume tube feeding if the patient isn’t post-pyloric.
- Place the patient in swimmer’s pose. Move up the patient’s arm on the side which their head is facing. Keep the shoulder neutral and place the elbow at 90 degrees. Extend the other arm with palm up and elevated on an offloading device or pillow.
- Place pillows under the patient’s shins to raise their toes off the bed and maintain their feet in a dorsiflexed position.
- Place a sheet and/or blanket over the patient.
- Return the mattress to low air-loss surface.
- Position the bed in reverse Trendelenburg position (between 10 to 30 degrees).
- Assess, treat, and reassess pain, sedation, and/or paralytic if applicable.
- Document the procedure in the patient’s record.
- Every 2 hours, while the patient is in the prone position, gather team members (respiratory therapist and at least two caregivers) to place the patient in swimmer’s pose on the opposite side. Readjust any offloading devices and pillows as needed.
- Document the turn in the patient’s record.
- When the patient has remained prone for the ordered amount of time, work with the care team, based on the patient’s condition, to return them to the supine position. Follow the step-by-step process in the reverse order.
Adapted from Vollman and colleagues. AACN Procedural Manual for Progressive and Critical Care. Copyright Elsevier.
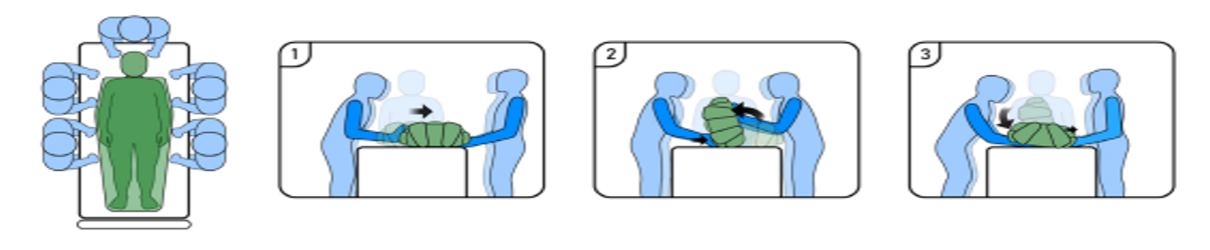
Figure used with permission of Wiggerman and colleagues. Illustration by Susana Peredo-Muniz
Before the turn. A provider must place an order to move a patient into the prone position.
- Before placing the order, the healthcare team (provider, respiratory therapist, nurse) should conduct interprofessional safety rounds.
- This collaboration should include a review of current ventilation settings, body habitus, and case scenario, as well as risk vs. benefit analysis of prone positioning based on indications and absolute and relative contraindications.
- Recommended prone positioning time is 12 to 16 hours.
- When the decision is made to move the patient into the prone position, provide patient and family education (the rationale for the position, its benefits, the procedure, and the treatment plan). Gather all necessary supplies, including sheets, pads, telemetry patches and leads, offloading devices (for example, lift/transfer sheet, pillows, cushions, positioners), and any other materials based on your organization’s protocol.
- Prone positioning should stop when the patient no longer demonstrates benefits from the position change or meets specific criteria. (See When to stop manual proning.)
When to stop manual proning
Stop manual proning when any of the following occurs:
- Improved oxygenation, as defined by PaO2/FiO2 ratio >150 mm Hg, with FiO2<60% and 10 cm of positive end-expiratory pressure after a minimum of 4 hours in the supine position.
- Complication occurs during a prone session that leads to an immediate interruption.
- Improvements in oxygenation cease or the goals of care have changed to palliative or end-of-life.
Patient safety. Take the following steps to ensure patient safety during and after the procedure.
- Physical assessment:
- Perform a comprehensive physical assessment.
- Perform eye care, including lubricating and horizontal taping of the eyes per your organization’s protocol.
- Assess pain, agitation, and delirium per your organization’s assessment tools. Ensure adequate applicable analgesic, sedation, and paralytics are ordered and that the patient meets the provider ordered goal.
- Assess body habitus and weight to ensure patient and caregiver safety during the procedure.
- Assess for contraindications and collaborate with the care team if you identify any.
- Stop enteral feeding unless post-pyloric feeding.
- Suction the patient’s oral cavity.
- Skin: Apply prophylactic foam dressings to the face and all bony prominences as needed to prevent deterioration of existing skin abnormalities and development of new injuries. (See Protecting the skin.)
- Dressings: Change dressings prior to pronation therapy.
- Drains and bags: Empty all drains and bags, including the following:
- Ileostomy or colostomy bags; place a pad around the stoma to prevent direct pressure
- Indwelling urinary drainage devices
- Chest tube
- Surgical drains
- Fecal containment device
- Secure lines, tubes, and drains:
- Ensure all peripheral I.V. lines are secure and that central venous and arterial lines are sutured or secured via a securement device based on organization protocol.
- Reposition all lines, tubes, and drains to prevent dislodgement.
- Remove any securement devices (such as StatLocks) that can cause medical device–related pressure injuries.
- Secure the endotracheal tube based on organization protocol. Ensure the patient’s tongue is inside the mouth. If the tongue is swollen or protruding, insert a bite block or an oropharyngeal airway.
Protecting the skin
The following diagram illustrates all areas of the skin that require protection when a patient is in the prone position.
![]()
Safe patient handling method. Selection of the handling method should be based on equipment and caregiver availability. However, consider consulting others (such as physical or respiratory therapists); more people may be required to safely perform the procedure due to patient body habitus and additional lines and drains. Options include the following:
- Ceiling lift (3 people minimum)
- Linen (5 people minimum)
- Transfer sheet (5 people minimum)
Awake prone positioning
Check your organization’s policy for APP; some have nurse-driven policies while others require provider orders. (See Awake proning.)
Awake proning
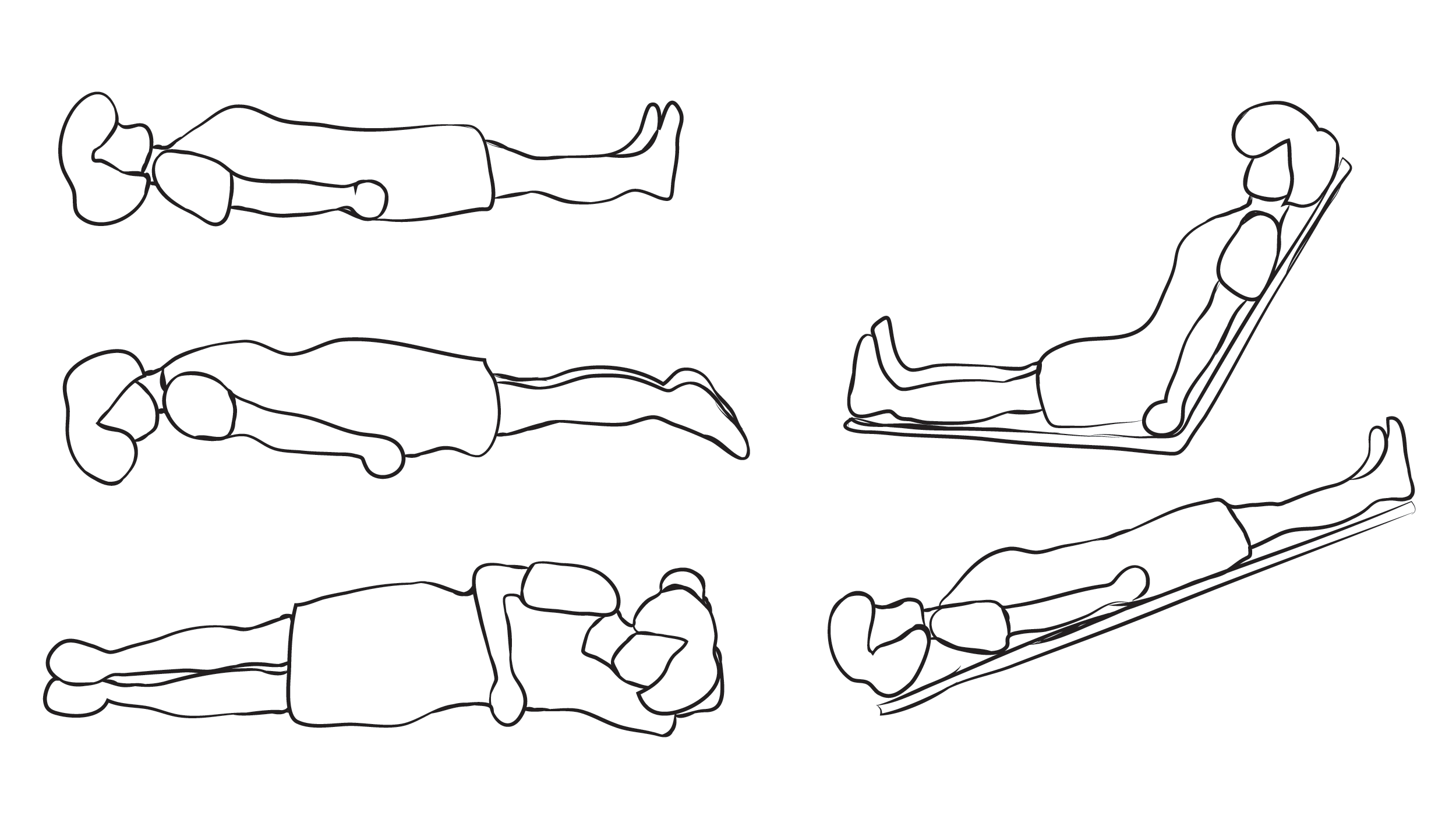
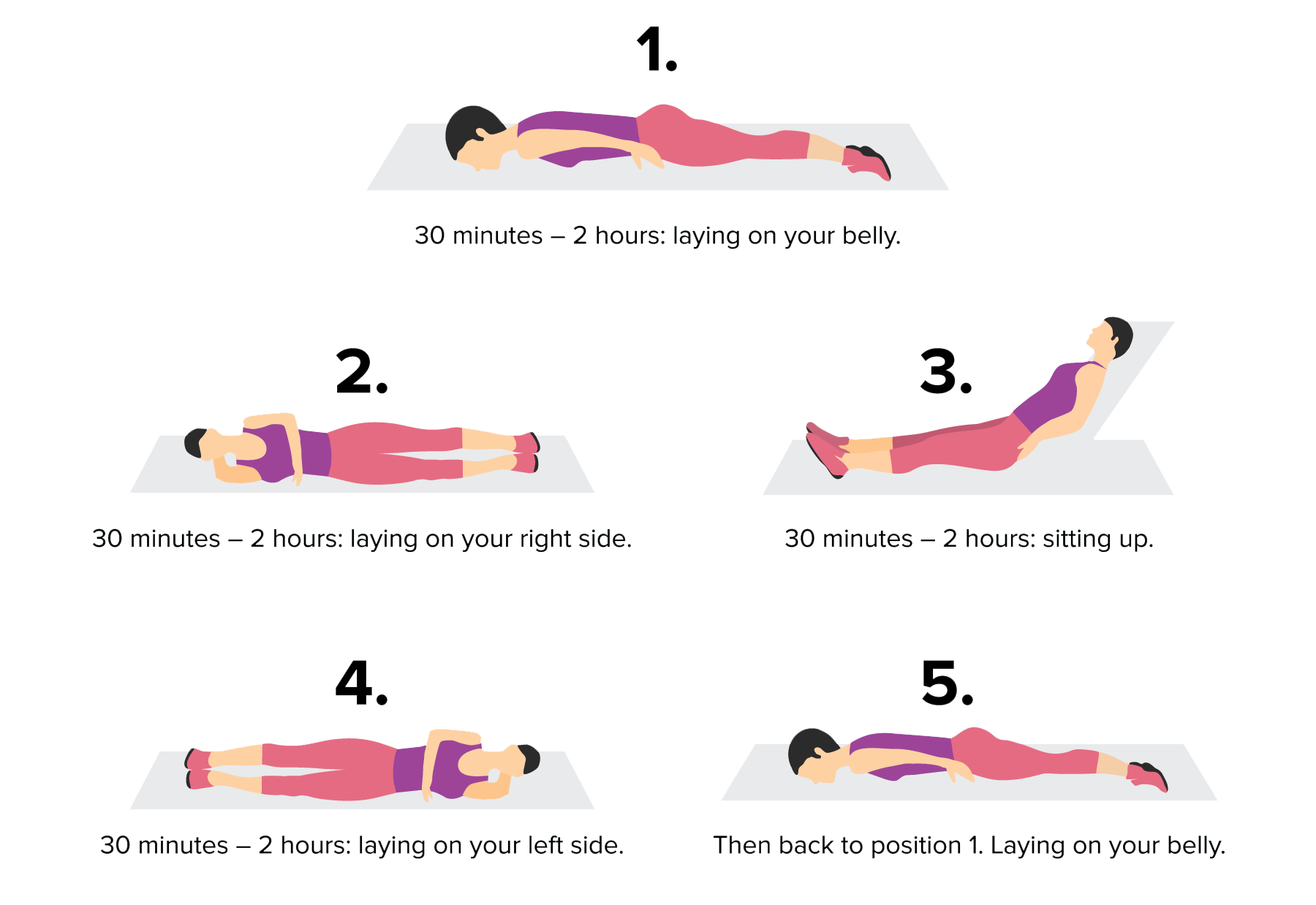
Implementing awake prone positioning with a patient who isn’t mechanically ventilated involves encouraging or minimally assisting them to lie on their abdomen or on their side to prevent further decline in respiratory status.
- Partner with the patient to change their position every 30 minutes to 2 hours—lying on their abdomen, on their right side, sitting up, and then lying on their left side. Keep this rotation schedule throughout the day.
- Ensure the patient hasn’t eaten anything for 30 minutes before lying on their abdomen.
- If the patient needs assistance, gather the proper number of caregivers based on the patient’s body habitus and your organization’s guidelines.
Before the turn. Perform the following nursing interventions before implementing APP:
- Obtain a provider order if needed at your organization or follow your nurse-driven protocol.
- Ensure the patient meets your organization’s inclusion criteria. In the case of contraindications, contact the provider.
- In collaboration with the provider, determine the goal length for APP. Recommended APP ranges from 30 minutes to 2 hours, two to three times a day depending on patient tolerance.
- Explain the reason for APP to the patient and family, its benefits, the procedure, and the treatment plan.
- Gather all necessary supplies, including sheets, pads, telemetry patches and leads, offloading devices (lift/transfer sheet, pillows, cushions, positioners), and any other materials based on your organization’s protocol.
- Stop prone positioning when the patient no longer demonstrates benefits or when the patient maintains optimal SpO₂ levels based on your organization’s protocol.
Patient safety. Take the following steps to ensure patient safety:
- Physical assessment:
- Perform a comprehensive physical assessment
- Ensure hemodynamic stability; collaborate with the provider if you note any abnormal findings.
- Assess pain, agitation, and delirium per your organization’s assessment tools.
- Assess body habitus and weight to ensure patient and caregiver safety during the procedure.
- Ensure the patient hasn’t eaten within the past 30 minutes.
- Skin: Apply prophylactic foam dressings to the face and all bony prominences as needed to prevent deterioration of existing skin abnormalities and the development of new injuries.
- Dressings: Change all dressings before pronation therapy.
- Drains and bags: Empty all drains and bags, including the following:
- Ileostomy or colostomy bags; place a pad around the stoma to prevent direct pressure.
- Indwelling urinary drainage devices
- Chest tube
- Surgical drains
- Fecal containment device
- Secure lines, tubes, and drains:
- Secure all peripheral I.V. lines and ensure that central venous and arterial lines are sutured or secured via a securement device based on organization protocol.
- Reposition all lines, tubes, and drains to prevent dislodgement.
- Remove any securement devices (such as StatLocks) that can cause medical device–related pressure injuries.
Prone positioning complications
In most cases, the benefits of prone positioning outweigh the risks; however, complications can occur, with patients who require mechanical ventilation at highest risk.
The most common complications associated with proning patients receiving mechanical ventilation include pressure injuries, airway dislodgement or endotracheal tube (ETT) obstruction, ocular and nerve injury, and caregiver injury. Several evidence-based nursing interventions can help reduce complication risk. In 2023, AACN distributed a prone practice alert, which provides details about potential complications and appropriate nursing interventions.
Always follow your organization’s prone positioning guidelines or protocols, and ensure healthcare team members have the resources they need to maintain patient and caregiver safety. If your organization doesn’t have a prone positioning protocol, work to develop one.
To prevent airway dislodgement or ETT obstruction, designate someone, preferably a respiratory therapist, to provide monitoring during the move from supine to prone, as well as every time the patent is repositioned. The management and visibility of all lines helps to prevent dislodgement and infection.
To avoid new or worsening skin breakdown, apply preventive dressings to all bony prominences or potential pressure points. These dressing help to reduce skin and subdermal soft-tissue loads by absorbing and wicking away extra moisture, which can lead to skin breakdown. Based on the patient’s anatomy, apply offloading devices to protect bony prominences. In addition, follow your organization’s protocols for eye care, lubrication, and taping to reduce the risk of ocular injury. Reverse Trendelenburg position can help minimize eye edema.
To ensure the safety of all healthcare team members, everyone should receive education about how to use the equipment available in your organization. For example, knowing whether mattress surfaces allow for maximum inflation can help make turning the patient easier. At a minimum, five team members must work together to turn patients who are mechanically ventilated; however, more may be required based on the patient’s condition, including body habitus, lines, and drains. For patients positioning themselves with APP, at least one team member (usually a nurse) should provide coaching and assistance.
The nurse’s role
Nurses monitor patients, perform assessments, document care, and ensure all team members follow safe patient handling procedures.
After the patient has achieved the proper prone position, monitor their response. With the first turn, the patient may experience a change in hemodynamic stability as a result of increased pressure on the cardiovascular system. To minimize this change, ensure the patient receives adequate sedation and preoxygenation before the move. Follow your organization’s guidelines and protocols for performing comprehensive physical assessments and vital sign requirements. If a patient experiences a cardiac arrest event, follow your organization’s guidelines regarding cardiopulmonary resuscitation in the prone or supine position.
Documentation should include a comprehensive physical assessment, including SpO₂, oxygen requirements and mode of delivery. Chart this information each time the patient is repositioned, along with off-loading, the devices used, and the angle of the bed. Report the patients’ ability to tolerate the procedure and repositioning, and any complications. In addition, note prone start time and return to supine, as well as all patient and family education.
Effective treatment
Manual prone positioning, which increased during the COVID-19 pandemic, has proven effective for patients with ARDS and ARDS COVID-19. In addition, APP was introduced for patients who don’t require mechanical ventilation and are experiencing hypoxic respiratory failure. Nurses aid identification of patients who meet prone position criteria and collaborate with the interprofessional team to initiate this invention early in the disease process. Additional research will evaluate the impact of APP on all patients with ARDS, not just those with COVID-19.
Jennifer Rechter is a clinical nurse specialist at Parkview Health in Fort Wayne, Indiana. Amanda Dauscher is a nursing professional development practitioner at Parkview Health. Kathleen M. Vollman is a clinical nurse specialist/consultant at Advancing Nursing LLC in Northville, Michigan.
American Nurse Journal. 2024; 19(11). Doi: 10.51256/ANJ112415
References
Bentley SK, Iavicoli L, Cherkas D, et al. Guidance and patient instructions for proning and repositioning of awake, nonintubated covid-19 patients. Soc Acad Emerg Med. 2020;27(8): 787-91. doi:10.1111/acem.14067
Gordon A, Rabold E, Thirumala R, et al. Prone positioning in ARDS. Crit Care Nurs Q. 2019;42(4):371-5. doi:10.1097/CNQ.0000000000000277
Grasselli G, Calfee CS, Camporota L, et al. ESICM guidelines on acute respiratory distress syndrome: Definition, phenotyping and respiratory support strategies. Intensive Care Med. 2023;49(7):727-59. doi:10.1007/s00134-023-07050-7
Guérin C, Reignier J, Richard JC, et al. Prone positioning in severe acute respiratory distress syndrome. New Engl J Med. 2013;368(23):2159-68. doi:10.1056/NEJMoa1214103
Malhotra A. Prone ventilation for adult patients with acute respiratory distress syndrome. UpToDate. June 28, 2024. bit.ly/3ZBWvFt
Mathews KS, Soh M, Shaefi S, et al. Prone positioning and survival in mechanically ventilated patients with coronavirus disease 2019-related respiratory failure. Crit Care Med. 2021;49(7):1026-37. doi:10.1097/CCM.0000000000004938
Morata L, Sole ML, Guido-Sanz F, Ogilvie C, Rich R. Manual vs automatic prone positioning and patient outcomes in acute respiratory distress syndrome. Am J Crit Care. 2021;30(2):104-12. doi:10.4037/ajcc2021674
Morata L, Vollman K, Rechter J, Cox J. Manual prone positioning in adults: Reducing the risk of harm through evidence-based practices. Crit Care Nurse. 2023;43(1):59-66. doi:10.4037/ccn2023174
National Pressure Injury Advisory Panel. Pressure injury prevention—PIP tips for prone positioning. bit.ly/3BeWDAN
Powers J, Chubinski S, Kadenko-Monirian M, Schultz S, Lung C, Carman T. Self-proning in non-intubated patients with COVID-19: A strategy to avoid intubation. MEDSURG Nurs. 2021;30(2):77-87.
Saguil A, Fargo MV. Acute respiratory distress syndrome: Diagnosis and management. Am Fam Physician. 2020;101(12):730-8.
Skin Integrity Research Group. Skin care considerations for the patient in prone position. 2020. hqsc.govt.nz/assets/Resource-library/COVID-19-Resource-hub/Publications-resources/Pronetect-practice-guidance-english-2020v2.pdf
Sryma PB, Mittal S, Mohan A, et al. Effect of proning in patients with COVID 19 acute hypoxemic respiratory failure receiving noninvasive oxygen therapy. Lung India. 2021;38(Suppl):S6-10. doi:10.4103/lungindia.lungindia_794_20
Vollman KM, Mitchell DA. Prone positioning for acute respiratory distress syndrome patients. In: Johnson KL, ed. AACN Procedure Manual for Progressive and Critical Care. 8th ed. Philadelphia, PA: Elsevier; 2024; 143-56.
Weatherald J, Parhar KKS, Al Duhailib Z, et al. Efficacy of awake prone positioning in patients with COVID-19 related hypoxemic respiratory failure: Systematic review and meta-analysis of randomized trials. Br Med J. 2022; 379:e071966. doi:10.1136/bmj-2022-071966
Wiggermann N, Zhou J, Kumpar D. Proning patients with COVID-19: A review of equipment and methods. Hum Factors. 2020;62(7):1069-76. doi:10.1177/0018720820950532
Key words: acute respiratory distress syndrome, ARDS, COVID-19, prone position, awake prone position
















