Nursing knowledge prompts timely intervention.
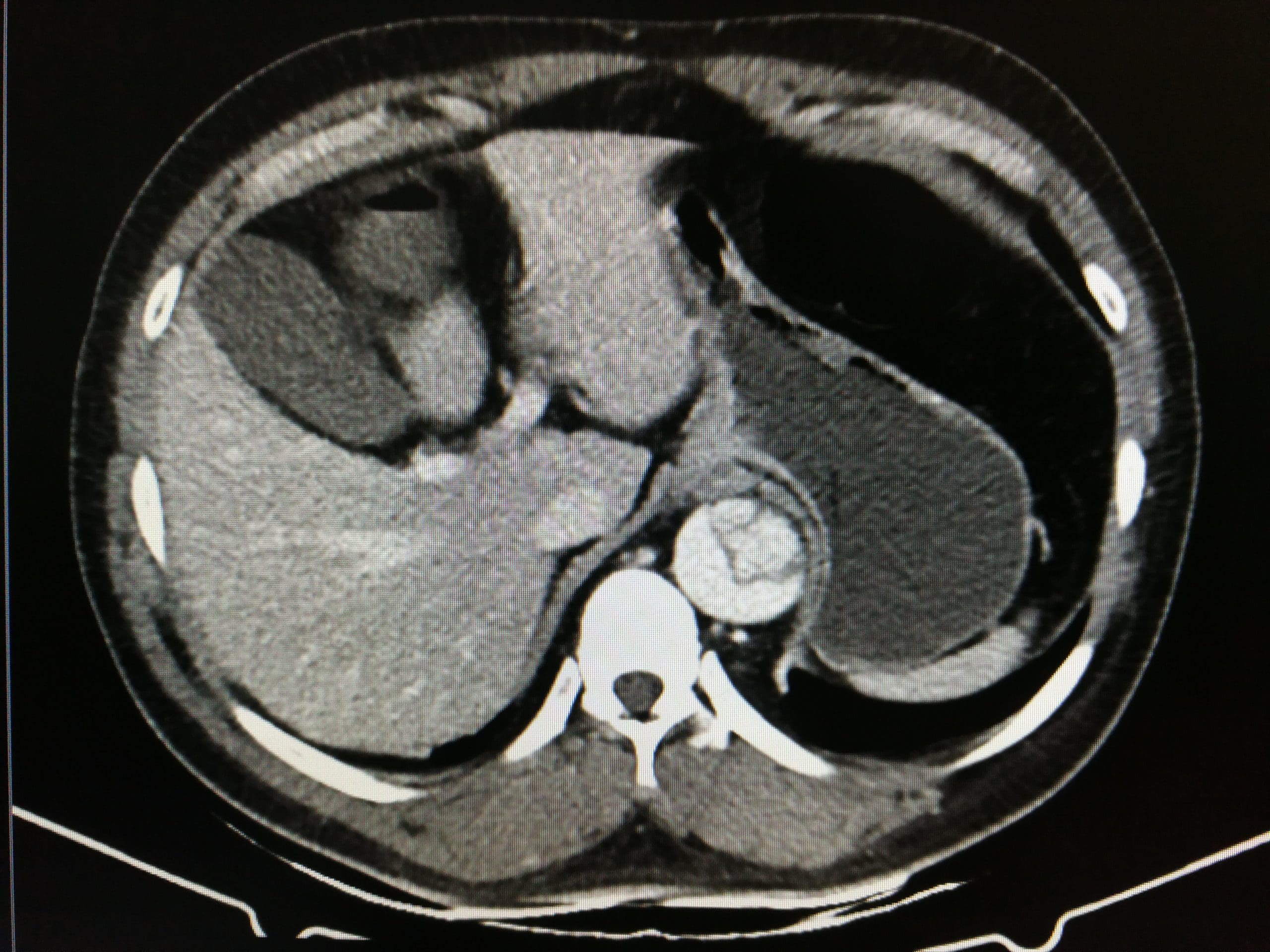
- An aortic dissection is caused by a tear in the intimal wall of the aorta forcing blood to flow between layers of the aorta to create a false lumen.
- Type A aortic dissections occur in the ascending aorta. Type B dissections occur distal to the subclavian artery and involve the descending aorta.
- Signs and symptoms of a dissection depend on the extent and location of affected structures and typically present as sharp chest or back pain.
Michael Alexander*, a 25-year-old man, arrives in the emergency department (ED) with chest pain and dyspnea after sustaining a fall. A chest x-ray reveals three broken ribs and a small-to-moderate pneumothorax in the right lung. He’s admitted to the medical-surgical unit for overnight observation. The thoracic surgeon will evaluate the pneumothorax.
Mr. Alexander has no significant medical history and takes no medications. He has a family history of hypertension, valvular disease, and Marfan syndrome. You take Mr. Alexander’s vital signs, which are BP 117/78 mmHg, HR 67 bpm, oxygen saturation 95% on 2 liters of oxygen via nasal cannula, and RR 18 breaths per minute. He describes his pain level as 4/10.
Recognizing aortic dissection: A race against time
Aortic aneurysm: Causes, clues, and treatment options
Reassessment
Four hours later, Mr. Alexander reports increasing chest pressure and pain. His BP is now 134/82 mmHg and HR 99. You attribute this to pain and administer the next scheduled oxycodone dose.
A half hour later, Mr. Alexander reports significant pain and you note diaphoresis, tachycardia, and hypertension. You remember that Mr. Alexander has a family history of Marfan syndrome and that the condition increases the risk for an aortic aneurysm and dissection.
On the scene
You call the rapid response team and report your suspicion of a potential aortic aneurysm or dissection. The team physician orders esmolol 50 mcg/kg/min to control HR and BP. A computed tomography angiography confirms an acute Type B aortic dissection. Mr. Alexander is transferred to the intensive care unit for further management.
Outcome
Mr. Alexander’s BP stabilizes, and his pain is controlled. After evaluation, the cardiothoracic surgeon determines that emergent surgery isn’t indicated. The patient will be weaned off the esmolol infusion, started on oral beta blockers, and eventually discharged home. As an outpatient, Mr. Alexander will receive ongoing monitoring and a workup for Marfan syndrome. The patient thanks you for your reassessment, knowledge, and prompt recognition of his condition.
Education
A tear in the intimal wall of the aorta can result in aortic dissection. This, in turn, forces blood to flow between layers of the aorta, creating a false lumen. Type A dissections occur in the ascending aorta and can involve the aortic arch; Type B dissections occur distal to the subclavian artery and involve the descending aorta.
Type A dissections require immediate recognition and intervention and carry a high mortality rate. Many Type B dissections can be managed medically unless they’re deemed complicated. Treatment includes endovascular repair and medications to manage BP, HR, and pain. Risk factors for Type B dissections include severe hypertension, connective tissue disorders (such as Marfan syndrome), and a family history of aortic aneurysm or dissection. Signs and symptoms, which depend on the extent and location of the dissection, typically include sharp chest or back pain.
Knowledge of the risk factors for a dissection and common signs and symptoms can help nurses act quickly to ensure patients receive the care they need. Patient education should include explanation of common signs and symptoms and referrals for counseling about strenuous activity and family planning.
*Names are fictitious.
Bernadette Sosnowski-Funk is an assistant professor of nursing at Hofstra University in Hempstead, New York, and an acute care nurse practitioner in cardiothoracic surgery at NYU Langone Health in New York City.
American Nurse Journal. 2024; 19(6). Doi: 10.51256/ANJ062455
References
Black JH. Clinical features and diagnosis of acute aortic dissection. UpToDate. August 1, 2022. bit.ly/3QcR8qU
Black JH, Burke CR. Management of acute type B aortic dissection. UpToDate. December 13, 2022. bit.ly/3UvzL6V
Carrel T, Sundt TM, von Kodolitsch Y, Czerny M. Acute aortic dissection. Lancet. 2023;401 (10378):773-88. doi:10.1016/S0140-6736(22)01970-5
Juraszek A, Czerny M, Rylski B. Update in aortic dissection. Trends Cardiovasc Med. 2022;32(7):456-61. doi: 10.1016/j.tcm.2021.08.008
Milewicz DM, Braverman AC, De Backer J, et al. Marfan syndrome. Nat Rev Dis Primers. 2021;7(64). doi:10.1038/s41572-021-00298-7
Sayed A, Munir M, Bahbah EI. Aortic dissection: A review of the pathophysiology, management and prospective advances. Curr Cardiol Rev. 2021;17(4):e230421186875. doi:10.2174/1573403X16666201014142930
Key words: aortic dissection, hypertension, Marfan syndrome, aneurysm