Preparation enhances nurse confidence.
- A fistula, an abnormal connection between two areas of connective tissue within the body, can occur spontaneously or be associated with surgery
- An interdisciplinary approach to care should include a Certified Wound Ostomy Continence Nurse, case manager/social worker, dietician, primary registered nurse, pharmacist, physician, and surgeon.
- Management options include pouching and negative pressure wound therapy.
As nurses, we care for various types of patients, but sometimes, we encounter patients with comorbidities we’ve only read about. We can feel overwhelmed when faced with unfamiliar diagnoses or treatments, but experience in practice allows us to gain confidence in our skills.
Patients with fistulas frequently fall into the category of conditions we’ve never seen before. To best prepare, refer to the basics of fistula management and consult an expert.
Wound care: Five evidence-based practices
What is a fistula?
A fistula is an abnormal connection between two areas of connective tissue within the body. Sometimes, a fistula occurs as a result of a disease process, such as Crohn’s disease or cancer, whereas others are inadvertently caused by surgical trauma. According to Metcalf, 75% to 85% of enterocutaneous fistulas occur during surgery. Some fistulas must be fixed surgically, while others can be managed with different modalities.
Care coordination requires an interdisciplinary approach, including a Certified Wound Ostomy Continence Nurse (CWOCN), case manager/social worker, dietician, primary RN, pharmacist, physician, and surgeon. Knowing what kind of fistula your patient has is the first step in determining how to successfully manage and coordinate care.
It’s in the name
The first part of a fistula’s name indicates its origin, and the second part denotes its termination point. For example, “enterocutaneous” tells us that the fistula starts in the small bowel (entero) and ends at the skin (cutaneous). Some fistulas are internal. For example, a colovesical fistula begins in the colon (colo) but ends in the bladder (vesical). In this situation, the output exits the body through the urethra, the same as urine.
Fistula management
A successful treatment plan includes several critical interventions. The provider may order antibiotics to prevent or treat an infection and other medications or modalities to address potentially agonizing pain or discomfort.
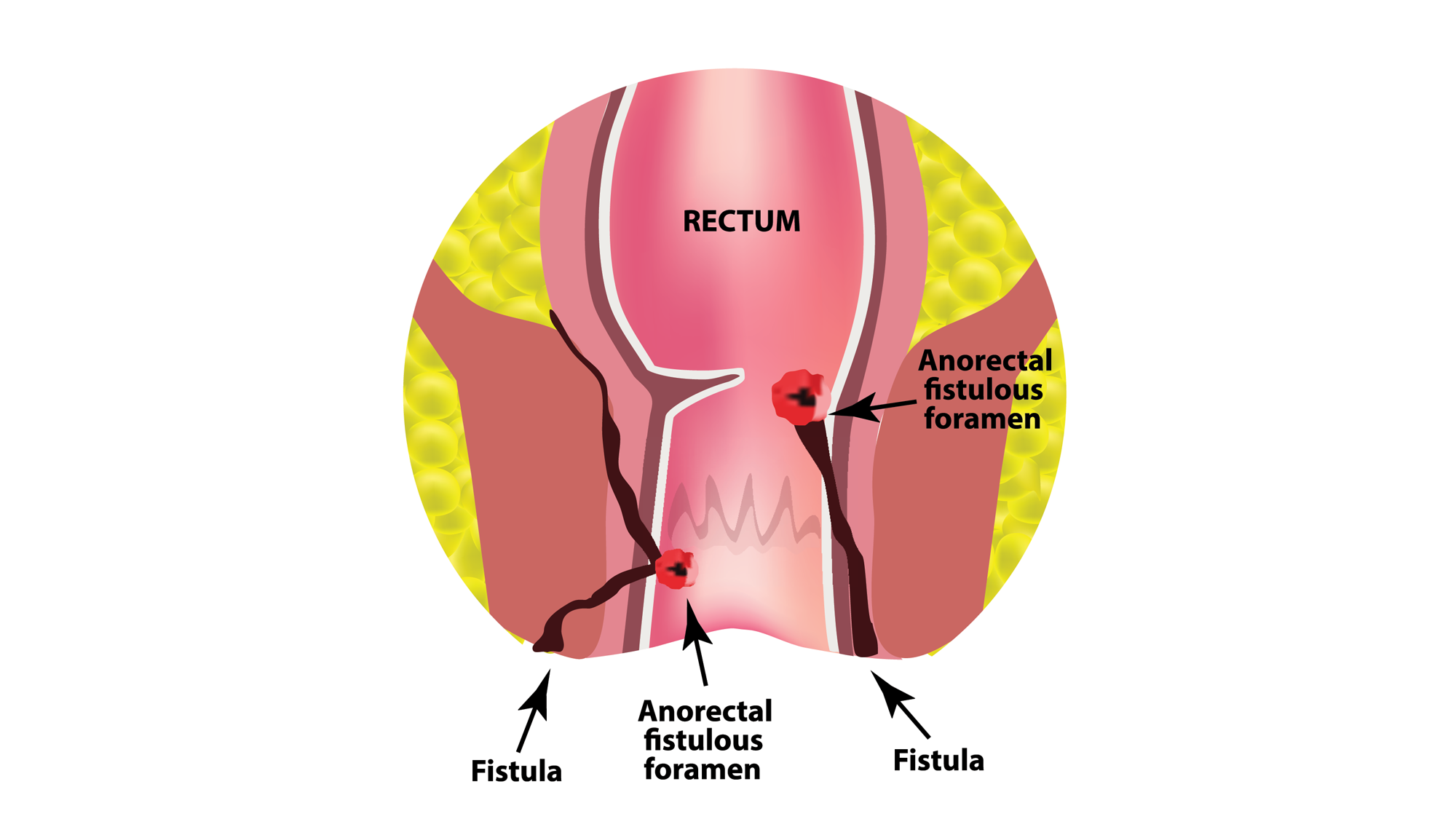
Managing the fistula output—which could be stool or mucous—involves protecting the skin and containing the output. The enzymes in stool that help break down food also cause skin breakdown, which introduces the potential for infection. If the fistula terminates near or in the rectum or urethra, skin breakdown can occur at an alarming rate. Skin protectants, such as those with petrolatum or zinc oxide, can help prevent skin breakdown and support healing. An absorbent pad also will facilitate wicking the output away from the skin; frequency of pad changes depends on the amount of output.
If the patient is bedbound, they must be turned and repositioned every 2 hours to prevent further skin breakdown in the form of a pressure injury. Placing the patient on a specialty air mattress will allow air circulation and offload the bony prominences.
Pouching
Depending on the amount of output from fistulas that terminate at the skin, the provider may order pouching. This entails applying a pouch or bag system to collect output and also protect the skin. Pouching options sometimes include a standard ostomy bag or a large ostomy bag (wound manager system).
In the presence of body folds or creases, a pouch system may not work due to the inability to create a seal. Fistula location also can preclude pouching. For example, perirectal fistulas are difficult to pouch. Most fistulas on the anterior side of the body trunk can be managed with a wound manager system or an ostomy pouch. A CWOCN can help the patient and staff determine the appropriate type of pouch.
Fistulas change over time, so selecting the appropriate pouch system can prove challenging. The best pouch system depends on several factors, including fistula location, output amount, and skin contours around the fistula opening (perifistula skin). These factors can affect how well the pouch seals and how long that seal will last. (See Pouch application.)
Pouch application
Before pouch application, cleanse the perifistula skin (skin surrounding the fistula) with warm water and then apply a protective barrier film. Cut the wafer of the wound manager or pouch system no larger than 1⁄8″ beyond the size of the fistula opening.
Application of barrier rings or stoma paste to the perifistula skin can help prevent output from leaking under the wafer. It acts as an extra sealant for the pouch system and increases wear time.
Sometimes, the wound manager or pouch system may be hooked up to a drainage bag (usually a foley bag) to ensure adequate output measurement. Drainage also allows for increased pouch wear time because the output has little contact with the wafer or the sealants.
Pouch system challenges
No two fistulas are the same, so care plans should be individualized. Working with a CWOCN can help identify the best approach, which may involve trying different products or adjusting the pouch system’s application process.
Creases at the perifistula skin may present problems with the pouch seal. Filling these uneven areas with barrier rings (by molding) or stoma paste can provide a flat, pouchable surface. Pouching systems require a dry surface for good adherence, so all output must be removed from the perifistula skin. During pouch application, suction at the bedside helps keep the skin clean and dry, especially from a high-output fistula.
When a patient moves or stands up, the perifistula skin may stretch or fold, causing it to change shape and compromise the pouch system’s seal. In addition, fistulas evolve as the body heals, altering the pattern or shape that must be cut into the wafer. Remind patients and their caregivers of these changes and how to adapt their pouch systems accordingly.
Actively leaking pouch systems must be changed. Trying to reinforce the pouch with tape or adhesive increases the chances of skin breakdown. Stool output trapped under the skin allows enzymes in the stool to break down the perifistula skin. In cases of perifistula skin breakdown, a pouch system over the fistula requires more frequent changes as the skin heals.
Negative pressure wound therapy
In some cases, negative pressure wound therapy can help heal wounds with a fistula. Rather than containing or managing fistula output as occurs with pouching, negative pressure dressing aims to assist in healing the wound in and around the fistula. A CWOCN can help determine whether the fistula (chronic or acute) can be separated or integrated into the dressing.
In certain situations, applying a negative pressure dressing can significantly improve outcomes for an acute low-output fistula, especially when protective dressings are placed over the fistula tract in advance. Negative pressure promotes compression of the abnormal opening, thus allowing the fistula to close. If the fistula can’t be incorporated into the negative pressure dressing, the wound can heal but the fistula will require pouching and management, much like an ostomy.
Fluid and electrolytes
High-output fistulas cause fluid and electrolyte imbalances, which require replacement. Patient and family education can help prevent imbalances. Some patients may require infusion services at home for total parenteral nutrition or I.V. fluids. If allowed, these patients should also drink water, broth, or juice to help manage the daily fluid and electrolyte imbalances they may experience. Our bodies naturally dictate how to offset imbalances, but patients with high-output fistulas must replenish them during daily activities.
Nutrition
Patients with a GI fistula who are permitted to eat should consume a diet low in residue and fiber to decrease output. Abnormally increased output can result in imbalances and challenges with pouch management. In the event of an output increase that requires frequent pouch changes, consider a foley bag to help drain the contents. In addition to allowing output measurement, this option prevents leaks near the patient’s skin.
Ask an expert
When caring for a patient with a fistula, many nurses feel unsure. These patients require a tremendous amount of care. Ask the provider for help in understanding the rationale behind a patient’s care plan. Some patients may share the cause of their fistula and how they manage at home. Talk to a CWOCN, who will prove a valuable resource in explaining the many intricate details associated with each type of fistula and how they’re managed.
When creating a care plan for a patient with a fistula, observe a CWOCN perform an assessment and begin the appropriate treatment. As wound care specialists, they blend clinical skills with evidence-based practices to effectively serve this patient population. Many fistula patients value this care, knowing it comes from a specialized area in nursing. This reassurance fosters trust and contributes to an overall positive patient experience.
Kristen Benavides is a wound care specialist and nurse manager at Dell Seton Medical Center at the University of Texas in Austin.
American Nurse Journal. 2024; 19(11). Doi: 10.51256/ANJ112444
References
Gefen R, Garoufalia Z, Zhou P, Watson K, Emile SH, Wexner SD. Treatment of enterocutaneous fistula: A systematic review and meta-analysis. Tech Coloproctol. 2022;26(11):863-74. doi:10.1007/s10151-022-02656-3
Ghimire P. Management of enterocutaneous fistula: A review. JNMA J Nepal Med Assoc. 2022;60(245):93-100. doi:10.31729/jnma.5780
Metcalf C. Considerations for the management of enterocutaneous fistula. Gastrointest Nurs. 2019;17(4):36-42. doi:10.12968/gasn.2019.17.4.36
Pepe G, Chiarello MM, Bianchi V, et al. Entero-cutaneous and entero-atmospheric fistulas: Insights into management using negative pressure wound therapy. J Cl Med. 2024; 13(5):1279. doi:10.3390/jcm13051279
Key words: fistula, pouching, negative pressure wound therapy, Certified Wound Ostomy Continence Nurse