

Train in a safe environment to increase new nurse confidence.
- According to The Bureau of Labor Statistics, healthcare workers are five times more prone to experience workplace violence than any other occupation, and they have a 20% higher chance of being assaulted.
- Nurses require training and proper tools to navigate episodes of workplace violence.
- The simulation environment provides a safe learning experience for students and current nurses to develop strategies for safely managing workplace violence.
Workplace violence (WPV) in healthcare remains a serious concern, and most healthcare workers will experience violence—physical acts, verbal intimidation, harassment, or threatening statements—committed by patients. (See WPV stats.)
The National Institute for Occupational Safety and Health and The Joint Commission recommend that healthcare facilities implement training programs to prepare staff in the event of WPV. However, research and training alone won’t address the issue. Nurses require evidence-based tools not only for their safety but also to ensure they remain in their role and the profession. Nurse educators, who have responsibility for educating and preparing nurses for the workplace, should begin WPV training in nursing school to prepare new nurses for the workplace.
WPV simulations allow educators to expose students to real-life scenarios in safe learning environments. They also help students develop foundational knowledge and skills associated with diffusing WPV, whether it involves patients, other coworkers, family members, or the general public. To better understand the benefits of simulation in preparing nurses to confront and manage WPV, we conducted a study focused on violence perpetrated by patients.
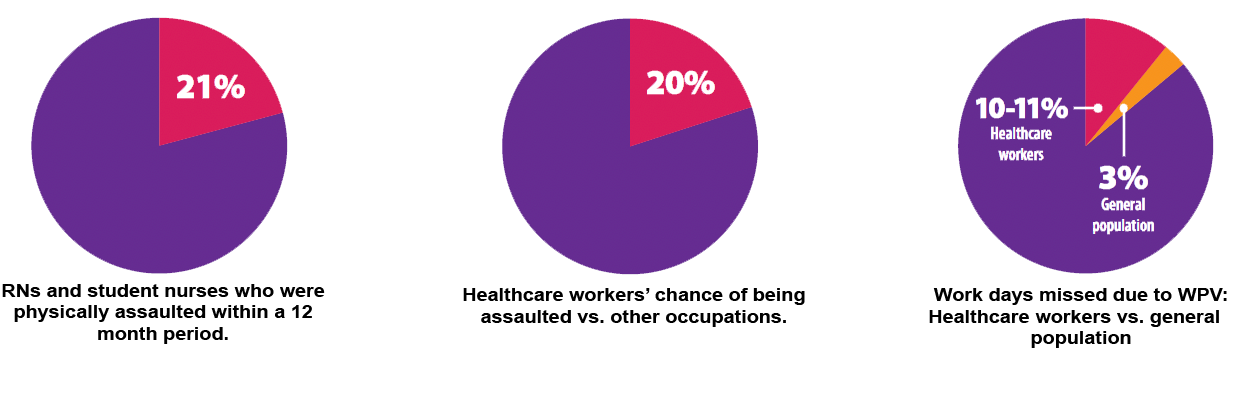
WPV stats
Jeong and Lee surveyed RNs (n=45) and student nurses (n=22) and found that 21% had been physically assaulted within a 12-month period. According to The Bureau of Labor Statistics, healthcare workers are five times more prone to experience workplace violence (WPV) than any other occupation, and they have a 20% higher chance of being assaulted.
WPV impacts employers as well. According to the Bureau of Labor Statistics, healthcare workers who missed days from work related to WPV were 10% to 11% (n=10,000) of the reported cases compared with 3% of the general population. Organizations must pay time off to those employees and pay for additional staff to cover their shifts.
Of more concern is WPV-associated stress, which can contribute to burnout and job dissatisfaction. When nurses experience burnout, their mental and physical health may suffer, which can lead to increased medical errors and patient safety issues.
What we learned from a literature review
Several studies note the benefits of simulation when training for WPV. A review of the literature indicates an increased ability to recognize both verbal and physical WPV after training exercises. Simulation participants also showed increased knowledge of WPV and appropriate responses, as well as increased coping skills and confidence when responding to these scenarios.
The controlled environment of simulation provides a physically and emotionally safe space for students to practice responding to WPV. Self-confidence and satisfaction in particular appear to increase with simulation activities. Students who participate in mental health simulation experiences related to WPV before starting their clinicals reported feeling self-confident and more prepared for the workplace environment.
How our study worked
Our study aimed to examine the satisfaction and self-confidence levels of BSN students before and after participating in WPV simulation. To guide the study, we selected the NLN [National League of Nursing]/Jeffries Simulation Framework and the Stevens STAR Model of Knowledge Transformation as the middle-range nursing theory and evidence-based practice (EBP) model. The NLN/Jeffries Simulation Framework guides educators in using appropriate standards and measurements to implement successful simulation exercises. The Stevens STAR Model aids evaluation and understanding of the stages of knowledge and how they’re used in evidence-based nursing practice. We recruited second semester BSN students (n=65) enrolled in a psychiatric/mental health nursing course because it included a WPV module. Our study contained no exclusion criteria.
The simulation scenario
The 20-minute simulation used for the training involved a hospitalized patient with schizophrenia who develops paranoia. The 28-year-old man, who was diagnosed with schizophrenia 10 years ago, becomes violent at home with his mother and is transported to the hospital for further evaluation. After admission, the patient becomes increasingly paranoid, which could easily result in a violent episode. During the simulation exercise, the students complete a focused mental status exam on the patient, use deescalating techniques, and maintain a safe environment for themselves and the patient.
Tools
We used a basic demographics tool to collect data about the participants, including their age, gender, ethnicity, and race. We also gathered information about participants’ education level, healthcare experience, and previous exposure to WPV.
Using the NLN/Jeffries Student Satisfaction and Self-Confidence in Learning tool, a 13-item instrument based on a Likert scale, we asked students to rate their level of agreement/disagreement with statements that gauge satisfaction and self-confidence. Five items concerned student satisfaction with the simulation and its suitability with regard to teaching methods and materials. The other eight items focused on self-confidence in learning by addressing mastery of content, skills development, and knowledge acquisition. (See Tool reliability and study results)
Ethical considerations
We obtained informed consent from all participants 1 week before the study. We found little risk associated with the study; however, potential emotional risk existed due to the subject of WPV. The students received all data about the background of the study, as well as information about the simulation before participating. This allowed students time to remove themselves from participation. All students who continued with the study had access to university counselors to help them manage any emotional response.
Study implementation
We recruited students for the study via email during the first week of spring semester. Participants had access to information about the study via the learning management system during that week. The simulation was part of a class assignment, but study participation was voluntary. The principal investigator (PI) and faculty members who volunteered to assist were not course instructors. One week before the simulation, the PI spoke to the students to remind them about the study and the information available for their review.
Pre-briefing material available to the students included the simulation scenario, the patient’s diagnosis, and a list of his medications. We encouraged students to review and research these materials on their own before the simulation.
We divided the 65 students into approximately eight groups. The PI met the students and asked them to sign informed consents. Students then completed the demographic questionnaire and the NLN Jeffries Simulation Tool via Qualtrics on their cell phones. After the simulation, each student who agreed to participate in the study completed the NLN Jeffries Simulation Tool via Qualtrics on their cell phone, while the PI observed. Due to scheduling constraints, debriefing of all students took place at one time via Microsoft Teams.
Study results
The average age of the participants was 21 years, and nearly 90% identified as female. Most of the participants reported their ethnicity as Non-Hispanic or Latino and their race as White. Most had completed high school or had a GED while others also reported completion of some college, an associate’s degree, or trade school. Nearly half said that they had healthcare experience, and 10% stated they had experienced WPV.
Student satisfaction and self-confidence increased after the WPV simulation, congruent with findings from the literature. All five areas of student satisfaction increased postintervention (n=65; P<.05), as did all eight areas of self-confidence (n= 63; P=.011). These results indicate the effectiveness of the simulation activity.(See Tool reliability and study results)
Tool reliability and study results
Reliability of the NLN/Jeffries Student Satisfaction and Self-Confidence in Learning tool was confirmed as with a Cronbach’s alpha: satisfaction = 0.94; self-confidence = 0.8. In addition, Unver and colleagues conducted a study on the reliability and validity of this tool, which showed a Cronbach’s alpha: satisfaction = 0.73; self-confidence = 0.86.
Satisfaction and self-confidence
We used the Wilcoxon signed-rank test to measure the difference in levels of student satisfaction with current learning and self-confidence in learning pre- and post-intervention. We found a significant improvement in student satisfaction in all areas (Z= -2.81, -4.74, P= .000–.005), with pre-intervention median at 3.0 and post-intervention median at 4.0. We also found a significant improvement in student self-confidence in learning pre and post-intervention (Z=-3.20, -4.40, P=.000–.001).
When examining prior exposure to WPV and satisfaction with current learning, a Spearman’s rank-order correlation showed positive correlations and statistical significance in all areas except Jeffries Question 1 (The teaching methods used in this simulation were helpful and effective) (rs(8) =.-088, P=.492). The analysis of self-confidence in learning and prior exposure demonstrated positive correlations and statistical significance except for Jeffries Question 6 (I am confident that I am mastering the content of the simulation activity that my instructors presented to me) (rs(8)=.014, P=.915); the pre-intervention median was 3.0 and the post-intervention median 4.0.
Limitations
This study was limited to students from one nursing course; future research should consider a sample size of students from various undergraduate nursing courses. In addition, this study had no control group. The use of a control group in future studies may provide more precise statistical data and help to expose any issues with internal validity and ensure that results are related to exposure to the simulated WPV event. In addition, students who know they’re being observed during a simulation may alter their normal responses, which could create a Hawthorne effect (modifying behavior because they’re being observed).
Implications for education and practice
Nurse educators are responsible for ensuring the safety and well-being of students and preparing them for the work environment. Implementing a WPV simulation scenario into nursing curricula can help prepare these vulnerable and inexperienced students. Simulations can increase their self-confidence and satisfaction levels to help them manage WPV incidents in the clinical setting. An authentic simulation delivered in a controlled and safe learning environment can help both students and practicing nurses prepare for WPV events.
Everyone deserves to work in a healthy and safe environment. The Joint Commission requires all accredited healthcare organizations to provide WPV response training to their healthcare workers. Organizations can accomplish this training by incorporating WPV simulations into annual employee competency evaluations.
Future research
Recommendations for future research include replication of this study with associate degree in nursing and graduate-level students to determine if the same results are obtained. Duplicating the study with other disciplines, such as social work students, might also provide insight into how simulation impacts satisfaction and self-confidence. In addition, quasi-experimental and longitudinal designs would help to assess participants’ future ability to manage WPV.
An effective tool
Simulation provides an effective tool for preparing nurses not only for their clinical role, but also to handle difficult professional situations. Given the frequency of WPV in healthcare, nurses should take advantage of every opportunity to prepare themselves to navigate these unsafe conditions. The training can help improve everyone’s experience, including patients’. With so many benefits, educators and employers should explore how to integrate WPV simulation training.
The authors are assistant professors at Troy University in Troy, Alabama.
References
Havaei F, Astivia OLO, MacPhee M. The impact of workplace violence on medical–surgical nurses’ health outcome: A moderated mediation model of work environment conditions and burnout using secondary data. Int J Nurs Stud. 2020;109:1-3666. doi:10.1016/j.ijnurstu. 2020.103666
Jeong Y, Lee K. The development and effectiveness of a clinical training violence prevention program for nursing students. Int J Environ Res Public Health. 2020;17(11):4004. doi:10.3390/ijerph17114004
The Joint Commission. Sentinel event alert 59: Physical and verbal violence against health workers. June 2021. jointcommission.org/resources/sentinel-event/sentinel-event-alert-newsletters/sentinel-event-alert-59-physical-and-verbal-violence-against-health-care-workers/
Martinez AJS. Implementing a workplace violence simulation for undergraduate nursing students: A pilot study. J Psychosoc Nurs Ment Health Serv. 2017;55(10):39-44. doi:10.3928/02793695-20170818-04
Martinez AJS. Enhancing nursing students’ competency skills with a workplace violence nursing simulation: Translating knowledge into practice. SAGE Open Nurs. 2019;5:2377960819843696. doi:10.1177/2377960819843696
Ming JL, Huang HM, Hung SP, et al. Using simulation training to promote nurses’ effective handling of workplace violence: A quasi-experimental study. Int J Environ Res Public Health. 2019;16(19):3648. doi:10.3390/ijerph16193648
National Institute for Occupational Safety and Health. About workplace violence. April 22, 2024. cdc.gov/niosh/violence/about/?CDC_AAref_Val=https://www.cdc.gov/niosh/topics/violence
National League for Nursing. Descriptions of available instruments. nln.org/education/teaching-resources/tools-and-instruments
Occupational Safety and Health Administration. Prevention of workplace violence in healthcare and social assistance. December 7, 2016. osha.gov/laws-regs/federalregister/2016-12-07
Unver V, Basak T, Watts P, et al. The reliability and validity of three questionnaires: The student satisfaction and self-confidence in learning scale, simulation design scale, and educational practices questionnaire. Contemp Nurse 2017;53(1): 60-74. doi:10.1080/10376178.2017.
1282319
Key words: workplace violence, simulation
















1 Comment. Leave new
WPV is very relevant and happens, especially in the area of mental/behavioral health (which is my area of expertise). As a Crisis Intervention Trainer, there’s no guaranteed ways of avoiding it. I love simulations and think that it broadens awareness of the possibilities and how to be proactive, as to stay safe and keep everyone safe. One of the big components I see often is staff not being vigilant and aware at all times of precursors the patient may be exhibiting. I think simulations and continuous trainings can help and decrease WPV.