
Thorough understanding aids appropriate use.
We analyze peripheral oxygen saturation (SpO2), which represents the percentage of hemoglobin saturated with oxygen in the blood, with pulse oximetry. Hemoglobin delivers oxygen to tissues throughout the body via the circulatory system. Because tissue perfusion can’t be measured directly, SpO2 serves as a surrogate for tissue oxygenation and a basic indicator of a patient’s health. It’s crucial to patient care in various settings. The technology uses light transmission to measure blood oxygen saturation through a probe placed on the patient’s body, most commonly the finger or forehead. (See Oxygen transportation.)
Oxygen transportation
Oxygen molecules bind to hemoglobin molecules on red blood cells. Red blood cells then circulate, releasing oxygen to tissues throughout the body.
![]()
Pulse oximetry is standard practice in most inpatient, outpatient, and home care settings. It’s a widely accessible, noninvasive, and inexpensive assessment tool compared to obtaining an arterial oxygen saturation (SaO2) level via arterial puncture, which is the gold standard for assessing oxygenation. An arterial blood gas measures multiple values, including but not limited to pH, PaCo2, PaO2, HCO3, and SaO2.The reliability of pulse oximetry to measure SpO2, typically within 3% to 4% of a patient’s SaO2, limits the need to perform the more invasive procedure.
Although nurses and other healthcare providers use SpO2 for clinical decision making, we should understand the limitations of pulse oximetry devices and how to use them appropriately.
History
The principles behind the use of oximetry technology have existed since the 1700s. Beer and Lambert’s study of light absorption and its relation to density established the Beer–Lambert law, which laid the groundwork for future technology.
In the late 1800s, researchers discovered that hemoglobin carries oxygen; however, not until the 1930s was the Beer–Lambert law used to confirm that light transmission could be used to measure oxygen saturation in blood. Scientists spent the mid-1900s trialing many methods to bring oximetry into patient care, with the first successful pulse oximeter created in 1981. Within 5 years, pulse oximetry became available worldwide with over a dozen brands on the market for use in healthcare settings.
Physiology and technology
Pulse oximetry measurement uses photoplethysmography (PPG) signals to measure and display SpO2. PPG signals use red light to measure light absorption via a direct current in body tissues and venous blood. It also uses infrared light to measure light absorption via an alternating current to gauge the changes in arterial blood flow. The ratio between the direct current and alternating current designates the oxygen saturation percentage expressed by a pulse oximetry sensor.
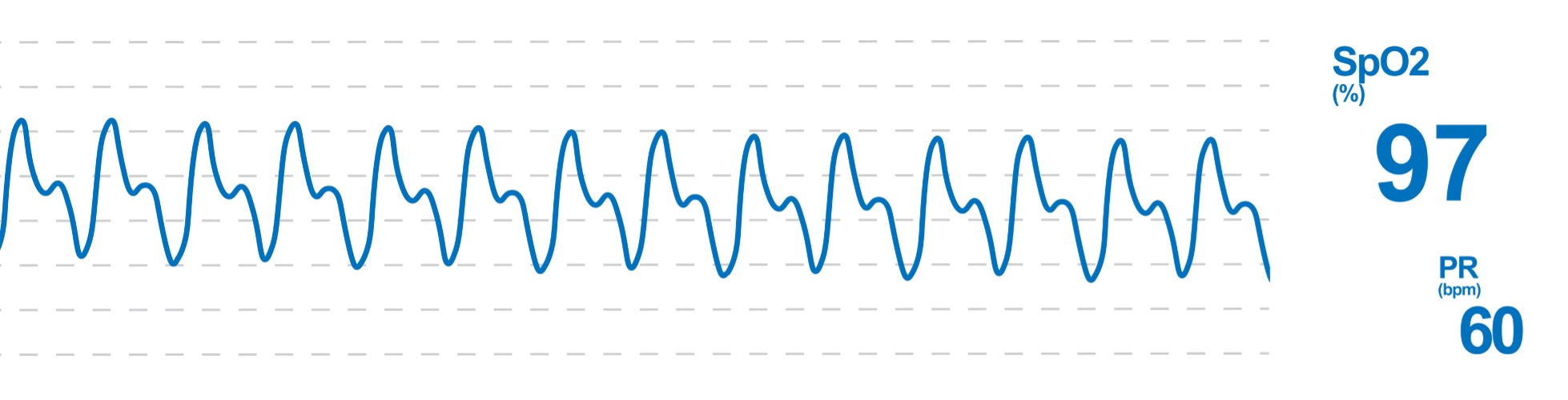
Frequently, SpO2 is characterized by a waveform called a plethysmograph (pleth). Analyzing the pleth can validate the accuracy of the value presented on the monitor. An adequate pleth exhibits one wave that correlates with each arterial pulse or heartbeat if an electrocardiogram is being monitored, with the exception of ectopic cardiac activity. Each wave should look similar in size and shape. (See Plethysmograph interpretation.)
Plethysmograph interpretation
The continuous pulse oximeter plethysmograph (pleth) should have one wave for every arterial pulsation. These waves are regular and of similar size and shape.
Nurses should know how to interpret the validity of oxygen saturation based on pleth characteristics, be able identify potential causes of variation, and understand appropriate nursing interventions.

Pulse oximetry limitations
Since pulse oximetry measurement relies on light transmission, any condition that alters light absorption can inhibit the oximeter’s ability to interpret SpO2. For example, the presence of nail polish, specifically darker colors, may block the light absorption needed to measure SpO2. Artificial nails are even more likely to impact light absorption. Excessive bright or fluorescent lights also may cause variability in light absorption, leading to false readings.
The effect of skin pigmentation on the accuracy of pulse oximetry has been long-studied. Originally, researchers found that patients with darker skin tones had lower reported SpO2 levels when using pulse oximeters. However, the research has since shifted to reflect that dark-skinned patients have overestimations in their reported SpO2 levels when compared to SaO2 levels obtained via blood draw. Occult hypoxemia occurs when an SaO2 registers less than 88%, despite a normally registering SpO2 of 92% or greater. These overestimations of SpO2 increase the risk of masking occult hypoxemia in patients with dark skin.
It is difficult to link and quantify how this healthcare bias impacts patients with dark skin, but occult hypoxemia leads to worsening patient outcomes, particularly when left untreated or when a delay in treatment occurs. According to Martin and colleagues, complications include prolonged hospitalizations, increased need for respiratory rehabilitation, and long-term oxygen requirements at home. Since this outcome disproportionality impacts patients with darker skin tones, as opposed to White patients, healthcare disparity occurs. The COVID-19 pandemic brought significant attention to this concern since SpO2 dictated most treatment.
Limitations associated with most available research include generalization of dark skin tones. Some evidence suggests that variability of pulse oximetry accuracy may exist among Asian, Latino or Hispanic, Native American or Indigenous, or mixed race/ethnicity patients compared to White patients. A tool such as the Fitzpatrick Scale can help classify skin by pigmentation rather than using the patient’s self-reported race. This scale separates skin pigmentation into six categories from lightest to darkest. Incorporating true pigmentation into future research may drive better understanding of variability sometimes represented by pulse oximetry measurement in patients of color. The Fitzpatrick Scale has some disadvantages. For example, it uses White skin as the baseline and it represents only six shades of pigmentation. Other scales, such as the Taylor Hyperpigmentation Scale, represents over 100.
Nursing considerations
Pulse oximetry sensors, typically placed on the fingers, toes, and earlobes because of the well-vascularized, pulsatile tissue, have a high level of accuracy. Patients find finger sensors relatively comfortable and convenient, and healthcare professionals find them simple to manage.
However, peripheral sensor placement can yield inaccuracy in the event of compromised perfusion. Chronic and acute conditions that limit blood flow can result in inaccurately transmitted light, making pulse oximetry measurement difficult. Patients with chronic arterial insufficiency, edema, and cardiac conditions that cause decreased cardiac output may experience inaccurate or unobtainable SpO2 measurements. Critically ill patients experiencing hypotension or hypothermia and those receiving vasopressors may have impaired peripheral circulation.
In addition, motion in the tissue being monitored may create artifacts and potentially false readings. Short, intermittent movements shouldn’t present a problem, but you may find it difficult to obtain an accurate reading in patients with constant motion in the fingers or toes. Earlobes serve as a good alternative site when peripheral perfusion may be compromised and digits aren’t capturing accurate measurements.
Pulse oximetry can be measured in some non-pulsatile areas. The forehead probe uses a reflective sensor to measure PPG signals. Forehead probes display similar accuracy to peripheral sensors in most patients. However, you might obtain increased accuracy using forehead probes in patients with impaired peripheral circulation. Forehead probes also may be well-suited for long-term use, especially in critically ill patients.
Whichever location you choose, assess the patient’s skin integrity and rotate sensor placement. In rare instances, patients can develop burns from pulse oximetry sensors. Thermal, chemical, and electrical burns have been documented in patients receiving SpO2 monitoring. Impaired blood flow to an appendage can decrease sensation and increase the risk of thermal injury. The risk of burns also can increase if equipment is used inappropriately or when using sensors for more than 8 hours without rotating the monitored site.
In addition to equipment troubleshooting, such as moving or replacing the sensor in the setting of poor pleth, consider physical assessment findings when interpreting SpO2 validity. Your nursing physical exam should include assessing for signs of hypoxemia, regardless of the SpO2 value. Some symptoms of hypoxia include decreased level of consciousness, restlessness, confusion, and tachycardia. Also watch for cyanosis, increased respiratory effort, reports of dyspnea, and pale or mottled extremities. These findings may indicate insufficient oxygenation and warrant further assessment, regardless of the SpO2 value on the monitor. (See Pulse oximeter application.)
Pulse oximeter application
Take the following steps when applying a pulse oximeter probe:
- Identify the patient with two unique identifiers to ensure you’re assessing the correct patient.
- Gather the needed equipment.
- Discuss the reason for pulse oximeter monitoring with the patient and family, including application of the device. Answer any questions they have.
- Select an area to apply the probe based on available equipment. Avoid areas with impaired skin integrity.
- Perform hand hygiene and don the appropriate personal protective equipment (PPE).
- When using a finger, toe, or earlobe probe, assess the selected site for signs of adequate blood flow. This includes temperature, sensation, color, and capillary refill of the extremity.
- Assess the entire extremity for anything that may interfere with measuring oxygen saturation, including blood pressure cuffs or other equipment.
- If you can’t locate a peripheral site with adequate perfusion, consider using a forehead sensor.
- Apply the pulse oximetry probe to the selected site.
- Connect the appropriate patient cable or adaptor into the display monitor.
- Set the appropriate alarms for low pulse oximetry readings and begin monitoring.
- Assess the SpO2 pleth for the presence of a pulsatile waveform displaying waves of similar size and shape. Although mild variability in the SpO2 percentage is normal, assess for validity any large transient variations without an obvious reason.
- Ensure the SpO2 displayed is consistent with the patient’s clinical appearance and report any clinical concerns to the provider.
- After completing intermittent pulse oximetry measurement, remove and disinfect SpO2 supplies, discard PPE, and perform hand hygiene.
- If monitoring continuous pulse oximetry, periodically relocate the sensor to avoid skin damage or breakdown.
- Frequently assess skin condition under the device location.
- Document the SpO2 reading, any delivered oxygen therapy, and education provided to the patient and family in the patient’s electronic health record.
One piece of the puzzle
Consider pulse oximetry as only one piece of the patient’s oxygenation status. The convenient, quick, and noninvasive reading shouldn’t overshadow the fact that inaccuracy can occur in some clinical situations. In addition to properly using and troubleshooting equipment, waveform interpretation and nursing assessment can help to substantiate all noninvasive SpO2 readings. In the event of uncertainty, measure oxygen saturation via arterial blood draw.
The authors are clinical practice leads at the Hospital of the University of Pennsylvania in Philadelphia
References
Aoki KC, Barrant M, Gai MJ, Handal M, Xu V, Mayrovitz HN. Impacts of skin color and hypoxemia on noninvasive assessment of peripheral blood oxygen saturation: A scoping review. Cureus. 2023;15(9):e46078. doi:10.7759/cureus.46078
Bickler PE, Feiner JR, Severinghaus JW. Effects of skin pigmentation on pulse oximeter accuracy at low saturation. Anesthesiology. 2005;102(4):715-9. doi:10.1097/00000542-200504000-00004
Cabanas AM, Fuentes-Guajardo M, Latorre K, León D, Martín-Escudero P. Skin pigmentation influence on pulse oximetry accuracy: A systematic review and bibliometric analysis. Sensors. 2022;22(9):3402. doi:10.3390/s22093402
Desai K, Taksande A, Meshram RJ. Second-degree burns in neonates: A rare case report of saturation probe injury in neonates. Cureus. 2023;15(10):e47761. doi:10.7759/cureus.47761
Jubran A. Pulse oximetry. Crit Care. 2015;19(1):272. doi:10.1186/s13054-015-0984-8
Kelly KL, Carlson AR, Allison TG, Johnson BD. A comparison of finger and forehead pulse oximeters in heart failure patients during maximal exercise. Heart Lung. 2020;49(3):259-64. doi:10.1016/j.hrtlng.2019.10.012
Tekin K, Karadogan M, Gunaydin S, Kismet K. Everything about pulse oximetry—Part 1: History, principles, advantages, limitations, inaccuracies, cost analysis, the level of knowledge about pulse oximeter among clinicians, and pulse oximetry versus tissue oximetry. J Intensive Care Med. 2023;39(3):775-84. doi:10.1177/08850666231185752.
Liu SH, Liu HC, Chen W, Tan TH. Evaluating quality of photoplethymographic signal on wearable forehead pulse oximeter with supervised classification approaches. IEEE Access. 2020;8:185121-35. doi:10.1109/ACCESS.2020.3029842
Martin D, Johns C, Sorrell L, et al. Effect of skin tone on the accuracy of the estimation of arterial oxygen saturation by pulse oximetry: A systematic review. Br J Anaesth. 2024;132(5):945-56. doi:10.1016/j.bja.2024.01.023
National Health Service. Guidelines on oxygen and oximetry. handbook.ggcmedicines.org.uk/guidelines/respiratory-system/guidelines-on-oxygen-and-oximetry. September 2022.
U.K. Okoji, S.C. Taylor, J.B. Lipoff, Equity in skin typing: why it is time to replace the Fitzpatrick scale, British Journal of Dermatology, Volume 185, Issue 1, 1 July 2021, Pages 198–199, https://doi.org/10.1111/bjd.19932
Parr, N.J., Beech, E.H., Young, S. et al. Racial and Ethnic Disparities in Occult Hypoxemia Prevalence and Clinical Outcomes Among Hospitalized Patients: A Systematic Review and Meta-analysis. J GEN INTERN MED (2024). https://doi.org/10.1007/s11606-024-08852-1
Poorzargar K, Pham C, Ariaratnam J, et al. Accuracy of pulse oximeters in measuring oxygen saturation in patients with poor peripheral perfusion: A systematic review. J Clin Monit Comput. 2022;36(4):961-73. doi:10.1007/s10877-021-00797-8
Saunders NA, Powles AC, Rebuck AS. Ear oximetry: Accuracy and practicability in the assessment of arterial oxygenation. Am Rev Respir Dis. 1976;
113(6):745-9. doi:10.1164/arrd.1976.113.6.745
Sjoding MW, Dickson RP, Iwashyna TJ, Gay SE, Valley TS. Racial bias in pulse oximetry measurement. N Engl J Med. 2020;383(25):2477-8. doi:10.1056/nejmc2029240

















