Learn how a high-reliability organization protected patient safety in a unique situation.
- High reliability organizations have a preoccupation with failure, are sensitive to operations, are reluctant to simplify interpretations, have a commitment to excellence, and defer to experts.
- This HRO hospital had to address unique patient identification issues for identical twins scheduled for the same surgery on the same day with the same surgeon in the same specialized postoperative unit.
A cardiology team scheduled a complex cardiothoracic surgery for identical young adult twins with the same life-limiting diagnosis. However, the twins insisted they undergo their surgeries on the same day with the same surgeon and recuperate in adjacent rooms. Because the surgeries were scheduled events, our medical center had time to plan additional layers of safety specific to patient identification concerns inherent to this situation.
According to Connor and colleagues, patient satisfaction has long been positively linked to patient safety and outcomes, so we made every effort to accommodate the twins’ reasonable requests. As a six-time American Nurses Credentialing Center (ANCC) Magnet® designated hospital and high-reliability organization (HRO), we prioritize patient safety, outcomes, and satisfaction. All medical center team members—those who provide direct patient care and those who don’t—remain committed to a goal of zero patient harm. (See HRO and healthcare)
HRO and healthcare
As procedures, technology, and patient care increase in complexity, healthcare benefits from applying attributes of high-reliability organizations (HROs) to improve patient safety and care quality. Hines and colleagues identified fundamental HRO characteristics that reflect exceptional patient care in health systems that participate in the Agency for Healthcare Research and Quality HRO Learning Network. They include the following:
- Initiate improvement in response to changing internal and external environments by applying current evidence.
- Identify opportunities for both improvement and threat mitigation.
- Study and measure change and rapidly initiate the findings.
- Apply established improvements across facilities and systems.
An HRO health system must consistently apply these attributes to all levels of patient care, professional engagement and development, leadership, and organizational culture.
On a daily basis, our health system practices these fundamental HRO principles. We address new opportunities and threats at all levels of patient care, staff needs, and leadership. Our culture of safety receives support and sustainment with daily interprofessional, collaborative safety huddles focused on harm prevention and threat response at the unit, department, and C-suite levels.
- Preoccupation with failure. Always be on the lookout for the smallest signal that a new (or existing) safety issue exists.
- Sensitivity to operations. Watch for deviations from standard work or best practices.
- Reluctance to simplify interpretations. Avoid broad, rationalized explanations when processes don’t go well; probe for root causes.
- Commitment to resilience. Learn from errors and put mechanisms in place to prevent future errors.
- Deference to expertise. If you don’t know the answer, don’t guess. Instead, find an expert. Sometimes that isn’t the person with the most seniority or the advanced degree.
Interprofessional collaboration
Senior nursing leaders representing cardiothoracic surgery and cardiac service lines managed the development of a comprehensive plan of identification and assessment of potential safety threats unique to the twins’ hospitalizations. They conducted a PubMed literature search using several keywords, including patient safety, wrong patient, twins, human error, cognitive errors, medication errors, nursing, and perioperative safety. They evaluated 216 articles for relevance by title and reviewed 26; however, none of the articles discussed this type of unique situation.
Patient safety regarding twins has long been a concern within obstetrics and during the peripartum hospitalization period due to nearly identical names. Reports of adverse events persist as a result of juxtaposition errors related to electronic health record and medication dispensation entry. We reviewed the safety protocols in place at our women’s health and obstetrics department and children’s hospital. The processes for pediatric patients, where parents are at the bedside, wouldn’t be sufficient for alert, oriented, and ambulatory young adult twins.
We recognized that identification at the point of patient encounter was most vulnerable, so we focused our safety plan on mitigating this threat. Our medical center has well-defined practices for establishing patient identification before any encounter. Usual care includes verifying two patient identifiers—patient name and date of birth or medical record number. We recognized that our challenge converged at this point of patient safety. These identical twins had the same last name, similar first names, medical record numbers that differed by only one digit, were scheduled for the same surgical procedure with the same surgeon on the same day, and would recover on the same specialized postoperative unit.
We identified the departments engaged in direct patient contact and included them in the safety planning. These departments met with nursing leadership to discuss and evaluate potential threats and develop additional safety measures. At these meetings, each department elaborated on their usual patient care, identified vulnerabilities in their practices relative to the twins, and proposed additional safety actions.
Interprofessional collaboration within the team environment prevented the unintentional creation of new threats. Feedback during team meetings identified the potential for one department’s proposed safety actions to conflict with another department completing their tasks. Sustainability also presented a challenge due to frequent shift changes and 24-hour care, which meant an abundance of hospital staff required instruction regarding error potential and education about the additional safety measures. (See Interprofessional safety)
Interprofessional safety
In preparation for the twins’ surgeries, we identified all of the departments that would have direct patient contact and included them in the development of the safety plan.
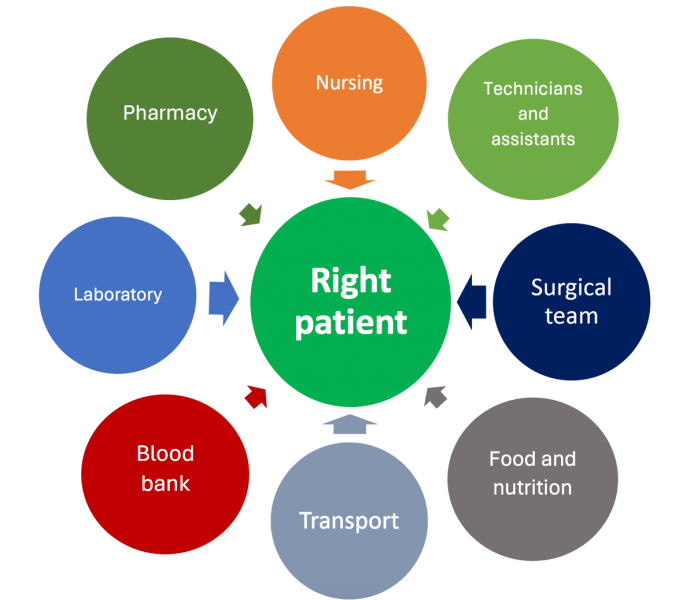
After formation of the safety plan, each department’s additional safety measures were emphasized in daily huddles for 2 weeks before the twins’ scheduled admissions and continued throughout their hospitalizations.
Safety plan
When the twins arrived on the morning of their surgeries, we assigned each a color (one red and one green) for the duration of their hospitalization to visually distinguish one from the other. We applied this color coding to their physical charts, name bands, and room assignments. We also adjusted the electronic health record to display red and green fonts for the respective twins. However, the green font proved difficult to read, so the green twin’s charting remained standard black. Other departmental safety measures included the following:
Nursing
- Each twin was assigned a different nurse and assistant on each shift.
- Each twin’s room entrance displayed a bold, color-coded label, red or green as appropriate, with the corresponding twin’s first name.
- At every shift change, the oncoming nurse and nursing assistant double-checked their assigned twin’s color-coded arm band for accuracy.
- All change-of-shift reporting emphasized the twins and the importance of following all of the extra safety measures.
- Daily huddles at the unit and leadership levels included a special focus on the twins so any team member encountering a twin was aware of the patient safety concerns and the additional measures in place to mitigate safety threats.
Surgery
- The surgery team scheduled prolonged preoperative timeouts to ensure accurate patient identification.
- They conducted an independent double-check of blood products when they arrived at the operating suite and before administration.
Pharmacy
- Independent double-checks occurred at the time of medication order fulfillment.
- The pharmacy structured locked medicine cabinets so that only one twin would appear on the access screen to avoid selecting the wrong one.
- Medications arrived on the unit distinctly separated and double-checked with the primary nurse when placed in each twin’s medication drawer.
Laboratory
- Before and after each blood draw, the nurse and phlebotomist performed independent double-checks to ensure placement of the right patient, right order, and right identifier on the vials.
- We performed two type and screen blood draws at two separate times on each twin with the same double-checks performed between the primary nurse and the phlebotomist.
Blood bank
- Before blood product order fulfillment, blood bank personnel double-checked type and screen results for correct patient identification.
- After order fulfillment, they performed another double-check and labeled the blood with the usual patient identifiers as well as the appropriate red or green label.
Technicians and assistants
- Before any encounter with a twin, the technician or assistant performed a double-check with the patient’s primary nurse.
- If the twin needed to leave the unit for a test, the twin’s primary nurse called the receiving department to confirm the test was for their twin patient.
Transport
- If either twin required transport to another part of the hospital, the transporter checked with the twin’s primary nurse to confirm the correct twin identification for the ordered test.
Food and nutrition
- Postoperatively, the twins’ diets advanced at different rates. Although they shared a common food allergy, their final diet orders differed.
- The primary nurse double-checked the meal delivery to ensure the correct twin received the correct meal.
Identification and mitigation
Sutcliffe as well as Vitale and Raman describe creating a culture of consistent communication via safety huddles with feedback and problem-solving as key components of an HRO. Preventable harm in the hospital setting can result from human or system errors or omissions. We identified human error as the focus of our mitigation strategies.
According to studies by Vitale and Raman, Wahr, and Suliburk and colleagues, as well as the World Health Organization, human error in healthcare occurs because of distraction from the task at hand, workarounds, fatigue, inadequate alarms or alerts, and other contributing factors, such as inattentiveness. According to Rodziewicz and colleagues, system error results from unforeseen design, educational, or cultural gaps. For example, when glucometer results upload slowly (system error) to the electronic health record, nurses may rely on nursing assistants to accurately verbalize (potential human error) blood sugar results when administering insulin before a patient begins a meal. Note that human error can play a key role in system error.
HRO success requires proactively identifying and sustainably mitigating potential patient safety threats. The nurses and care team members at our medical center initiated preemptive changes in preparation for this extraordinary situation, and they identified opportunities to enhance patient safety by mitigating threats.
The complex nature of cardiothoracic surgery and postoperative care demands interprofessional collaboration. Postoperatively, our cardiac nursing leaders managed the complex interaction of department and unit team members caring for these patients.
Error-free hospitalization
Our nurse-driven comprehensive safety plan realized optimal outcomes during a unique situation. Our care teams acknowledged the risks involved in caring for identical twins having the same surgery on the same day with the same surgeon and recovering on the same unit. By recognizing the opportunities to ensure patient safety, planning for successful threat mitigation, and consistently implementing our patient safety plan, the twins experienced error-free hospitalizations.
Maria Alcina Fonseca is a nurse manager in cardiac surgery at Morristown Medical Center in Morristown, New Jersey. Nancy Levy is director of cardiac services at Atlantic Health System and Morristown Medical Center. Lise Cooper
is a nurse researcher at Atlantic Health System.
American Nurse Journal. 2024; 19(9). Doi: 10.51256/ANJ092440
References
Connor L, Beckett C, Zadvinskis I, et al. The association between Magnet® recognition and patient outcomes: A scoping review. J Nurs Adm. 2023;53(10):500-7. doi:10.1097/NNA.0000000000001325
World Health Organization. Global Patient Safety Action Plan 2021–2030: Towards eliminating avoidable harm in health care. 2021. who.int/publications/i/item/9789240032705
Hines S, Luna K, Lofthus J. Becoming a high reliability organization: Operational advice for hospital leaders. AHRQ Publication No. 08-0022. Rockville, MD: Agency for Healthcare Research and Quality. April 2008.
Lal MM. Introducing Magnet® with Distinction. J Nurs Adm. 2023;53(3):125-6. doi:10.1097/NNA.0000000000001255
Rodziewicz TL, Houseman B, Vaqar S, Hipskind JE. Medical error reduction and prevention. February 12, 2024. StatPearls. ncbi.nlm.nih.gov/books/NBK499956
Suliburk JW, Buck QM, Pirko CJ, et al. Analysis of human performance deficiencies associated with surgical adverse events. JAMA Netw Open. 2019;2(7):e198067. doi:10.1001/jamanetworkopen.2019.8067
Sutcliffe KM. Building cultures of high reliability: Lessons from the high reliability organization paradigm. Anesthesiol Clin. 2023;41(4):707-7. doi:10.1016/j.anclin.2023.03.012
Vitale MG, Raman DL. Safety does not happen by accident: Preventing human error through high-reliability practices. J Pediatr Orthop. 2022;42(suppl 1):s35-8. doi:10.1097/BPO.0000000000002067
Wahr JA. The cognitive basis for human error and the best practices to reduce error. Anesthesiol Clin. 2023;41(4):719-30. doi:10.1016/j.anclin.2023.06.003
Weick KE, Sutcliffe KM. Managing the Unexpected: Sustained Performance in a Complex World. 3rd ed. San Francisco, CA: Jossey-Bass; 2015.
Key words: hospitalized twins, patient safety, patient identification