✓ TA temperature is real time temperature

- Just like pulmonary artery temperature, TA temperature identifies changes in your patient’s temperature sooner than axillary, oral, or rectal temperature
✓ Measure only exposed area
- Anything covering the area to be measured would insulate and prevent the heat from dissipating, resulting in falsely high readings. Brush the hair aside if covering the TA, or the area behind the ear.
- Measure only the up-side on a patient in a lateral position. The down-side will be insulated preventing the heat from dissipating, resulting in falsely high readings.
✓ Measure only the up-side

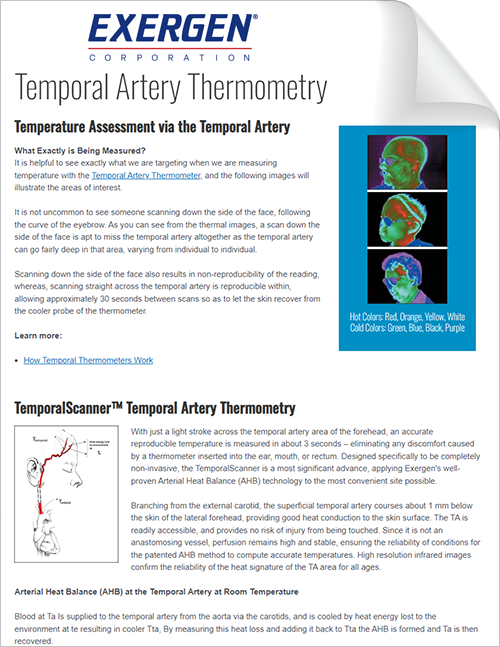
✓ Measure straight across the forehead, from the center to the hairline (or start at the hairline) ending with a touch on the neck behind the earlobe
- Slide the thermometer midline straight across the forehead (think of a sweatband), and not down the side of the face. Midline, the temporal artery is about 2mm below the surface, but can go deeply below the surface on the side of the face.
✓ Sequential Measurements Result in Variability
- Sequential measurements cool the tissue, resulting in variable temps. Wait 30 seconds or so for skin to recover, or use the opposite side if exposed.
✓ One Measurement TA Temperature on an Infant
- One measurement, preferably at the temporal artery area, is all that is required on an infant as the perfusion rate is normally strong…
- If visibly diaphoretic, push aside any clothing or blankets covering the neck area for ~30 seconds or so, and make the measurement on the neck behind the ear.
 Preferred site is the temporal artery area. Here, behind the ear could be alternate site, as both are exposed.
Preferred site is the temporal artery area. Here, behind the ear could be alternate site, as both are exposed. Temporal artery area is the only option here, as the neck area is not exposed.
Temporal artery area is the only option here, as the neck area is not exposed.✓ Low Readings Can be Caused by a Dirty Lens

- Biweekly cleaning of the lens is a good procedure. To clean, simply twirl a cotton tipped swab (Q-Tip) dampened in alcohol on the lens, deep in the center of the probe.
Questions? 617-923-9900 x202
Exergen Temporal Thermometry FAQ’s
Frequently Asked Questions by Nursing Staff

What should I do if I get an abnormally high reading?
- Repeat the reading with the same thermometer; a correct reading will be reproducible
- Repeat the reading with another Exergen TA Thermometer; 2 thermometers with the same reading will confirm the reading
What should I do if I get an abnormally low reading?
- Causes of a low or abnormally low reading are:

- Debris on the lens will cause a low reading. To resolve, dampen a Q-Tip with an alcohol prep pad. Gently twirl on lens, use another Q-Tip to dry. This should be done routinely on a biweekly basis.
- Premature release of the button.

- Measuring when an ice pack or wet compress is on the forehead
- Measuring a completely diaphoretic patient – but in this case, the temp is rapidly dropping and fever is not a concern. Wait until the patient is dry and repeat the measurement.

The green area is cool, as the temporal artery can go deep at that point. - Scanning down the side of the face where temporal artery could be embedded under fat or cartilage. Scan straight across forehead. The temporal artery is closest to skin in that area.
- If you had to remove your patient’s glasses, you incorrectly went down the side of the face.
- If none of the above applies, proceed as with high readings above to confirm the reading.



What are alternative sites because I cannot access the forehead?
- Femoral Artery Area
- Scan across the femoral artery in the crease of the groin, keeping button depressed until scan is completed.
- The femoral artery is a strong artery and has a long history as a temperature measurement site
- Femoral Artery Area

- Lateral Thoracic Artery Area
- Scan in a zigzag pattern about 4 inches wide from an imaginary line in between the axilla and the
nipple, scanning down to the waist and back up to the level of the nipple, keeping the button depressed until scan is completed.
- Scan in a zigzag pattern about 4 inches wide from an imaginary line in between the axilla and the
What are alternative sites because of diaphoresis?

(Green/Blue)
- Area on the Neck behind the Earlobe:
- If this area is dry, this site can be used alone on a diaphoretic patient or on a patient with head trauma
(surgical or accidental), as the neck area is certain to be vasodilated in these two conditions (red area designates heat). - We sweat first on the forehead, then the palms of the hands and soles of the feet, then the T-zone on the back,
and finally, everything is wet, but the neck area is one of the last places to get wet. - If the neck is not accessible, and if dry, the femoral or lateral thoracic artery areas can be used.
- If all sites are wet, the patient’s temperature will be rapidly dropping and fever is not an issue. Return in about 15 minutes when the patient should be dry and take a standard temporal artery temperature.
- Wiping the sweat will not work as the sweat glands secrete too quickly and the area will still show the effect of evaporative cooling
- If this area is dry, this site can be used alone on a diaphoretic patient or on a patient with head trauma
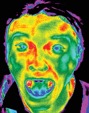
If it is alright to spot check behind one ear, why should I scan the forehead as well?

- The area behind the ear only works as a sole site if there is 100% vasodilation. In the absence of diaphoresis or
head trauma, vasodilation in the neck area is uncertain, making this area too variable to be reliable as a sole site. - The woman at the right has normal, constant blood flow in the temporal artery, but she is vasoconstricted in her neck area, which makes it cool (green).
How long should I wait if the scanable area is covered or patient lying on that side?
- About 30 seconds will be sufficient for the area to equilibrate to the environment
How long should I wait between readings?
- Sequential readings on the same patient in rapid succession will cool the skin, it is best to wait 30 seconds for the skin to recover from the cold probe.
How do oral temperatures differ from arterial?
- Oral temperatures are affected by patient activity such as mouth breathing, coughing, snoring, eating, drinking, etc.
- Oral temperatures can vary 2-3 degrees depending on the placement of the probe (blue/green = cold, red/yellow = hot).
- Oral temperatures can seriously mislead the clinician because of the resulting artifactual errors.
- Temporal artery temperature is not affected by any of these activities.
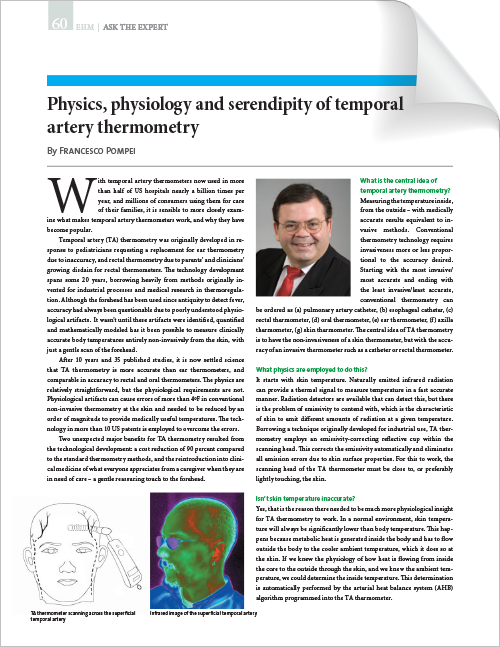
How does this technology work, i.e. how does the device measure heat?
- The instrument uses an infrared sensor in the center of the probe head to measure the heat naturally emitting from the body
- The instrument also uses a thermistor (like the electronic thermometers) that is embedded in the back of the probe to automatically measure ambient temperature. This controls for any affect on the skin from ambient temperature.
- The computer in the instrument then synthesizes the two temperatures to provide a core temperature as accurate as a temperature measured by a pulmonary artery or esophageal catheter.
How does this relate to core temperature?
- Temporal artery temperature, because it has been demonstrated as accurate as the temperature measured by a pulmonary artery and esophageal catheter, and as accurate as a rectal temperature on a stable patient, is considered a core temperature.
- Rule of thumb: Rectal temperature is about 1F (0.5C) higher than an oral temperature and 2F (1C) higher than an axillary temperature. It will be easy to remember if you think of core temperature as a rectal temperature, and apply the
same protocol you would use for a rectal temperature.
What makes my patient feel hot yet get a “normal” temperature?
- Body heat is produced in the deeper core tissues of the body, which is insulated by the subcutaneous tissues and skin to protect against heat loss.
- Vasoconstriction decreases the transport of core heat to the skin surface, and vasodilation increases transport.
- During vasodilation, circulating blood transports heat to the skin surface, where it dissipates into the surrounding environment. This is the body’s way of maintaining a normal temperature, but the skin can feel warm to the touch, especially if the hand is cool.
- If no heat is dissipated, body temperature would rise about 1.8°F (1°C) per hour
- Vasoconstriction does the opposite by decreasing the transport of core heat to the skin surface, keeping it within the deeper core tissues of the body. This allows a fever to increase, but the skin will feel cold to the touch even though
the fever is present.
Why shouldn’t I compare this to an oral with our old devices?
- The first reason is because your old devices measuring oral temperature are subject to all the patient activities mentioned above.
- The second reason is because your old thermometers are not measuring an actual temperature but are predicting what the temperature should be if the probe remained in position several minutes.
- The temporal artery thermometer is measuring an actual temperature. It has been proven in peer-reviewed published studies to be as accurate as temperatures measured by pulmonary artery and esophageal catheters, and as accurate as a rectal temperature on a stable patient. It has also been proven to identify changes in temperature long before rectal temperature, even on infants.
Should I use this device with radiant warmers?
- No, not unless the temporal artery thermometer has been left under the radiant warmer for 30 minutes so it equilibrates to that environment. When equilibrated, the warmer can either be turned off for the short time the temperature is taken, or the temperature can be taken in an area not exposed to the radiant warmer.
- In the Neonatal Intensive Care Unit, because of all the radiant warmers, nursing staff sometimes prefer to use the Exergen instant axillary thermometer.
What about use of bair-huggers or other warming devices? How should we take temperatures?
- As long as the warming devices are not covering the area being measured, they will not interfere with the use of the temporal artery thermometer.
Do I need to take the temperature of an infant at both the temporal artery area and on the neck behind the earlobe?
- No, one measurement, preferably at the TA, is all that is required
- Measurement site must be exposed, push hat up if present
- Do not use if infant is under a radiant warmer*
Left, preferred site is the temporal artery area. Behind the ear could be alternate site, as both are exposed.Left, the temporal artery area is the only option, as the neck area is not exposed.*Use Exergen Neonatal Instant Axillary Thermometer (LXN) under the warmer