

This practice improvement plan accomplished an ambitious goal.
- Diabetic foot ulcers are costly and challenging, but can improve with a team approach and close follow up.
- Multidisciplinary guidelines can aid 50% reduction in diabetic foot ulcer size.
- Engaging patients with diabetes in recognizing early changes in their feet helps detect wounds and prevent complications.
Foot ulcers continue to present a serious health concern for patients with diabetes. About 26 million people a year (6.3% of patients with diabetes globally) experience diabetic foot ulcers with an annual cost of between $9 billion and $13 billion. (See About diabetic foot ulcers.)
Wound care: Five evidence-based practices
Diabetic ketoacidosis and hyperglycemic hyperosmolar state
Obesity: Skin issues and skinfold management
Without early assessment, timely intervention, and adherence to a healing plan, diabetic foot ulcers can lead to hospitalization, amputation, or death. Sheehan and colleagues found that a 50% change in foot ulcer size (as measured by area) after 4 weeks suggests a strong indication of healing by 12 weeks. If wounds fail to achieve 50% reduction by 4 weeks, providers should reassess and consider advanced treatment modalities.
In 2018, patients with diabetic foot ulcers accounted for 10% of initial visits at our three tertiary ambulatory wound centers. Length of time for healing varied by provider. Tracking data in 2019, we used Sheehan and colleagues’ study to set a goal of achieving 50% wound closure by 4 weeks in 50% of patients with initial nonpalliative diabetic foot ulcers. Initial data collection of wound measurements (length x width) and visit dates showed that 37% of new diabetic wounds reduced by 50% within 4 weeks and that healing rates varied by providers. Knowing that diabetic foot ulcers typically take months to heal, often recur, and require a comprehensive approach for healing, our nursing team recognized the opportunity to improve outcomes for patients.
About diabetic foot ulcers
Understanding the pathophysiology of diabetic foot ulcers, as well as risk factors and care options, can help healthcare teams develop systematic and holistic strategies for improved patient outcomes.
Pathophysiology
A combination of peripheral arterial disease and diabetic peripheral neuropathies (motor, sensory, autonomic) can lead to diabetic foot ulcers. Initially, patients may experience tingling, burning, prickling, or numbness in the legs and feet from sensory nerve damage. This, in turn, can result in a loss of balance or coordination and difficulty walking on uneven surfaces. Structural foot changes contribute to gait changes, ill-fitting footwear, and callous formation. Autonomic changes disrupt blood flow to the skin and lead to dry skin and loss of sweating.
These changes and repeated trauma, friction, or pressure of callouses, fissures, and cracks cause subcutaneous bleeding and eventually ulceration, which can lead to a break in the skin’s protective barrier and increase the risk of micro-organisms entering the body. Ultimately, the patient experiences infection and thermal changes in the skin.
Risk factors
Patient risk factors for diabetic foot ulcers include the following:
- Chronic heart failure
- Coronary artery disease
- Gender (men generally have increased plantar peak foot pressure)
- Glycemic control
- Limited care access
- Longer duration of diabetes
- Obesity
- Race (Black, Hispanic, and other marginalized groups are less likely to receive early intervention)
- Smoking
- Socioeconomic status
- Stroke
Foot risk factors include tissue inflammation and structural and sensory changes as a result of peripheral neuropathy.
Treatment
Treatment guidelines for diabetic foot ulcers advocate multiple modalities. The International Working Group on the Diabetic Foot and other organizations recommend the following:
- Address systemic support.
- Assess feet regularly (including skin temperature).
- Ensure follow-up with a healthcare provider trained in recognizing and treating diabetic foot ulcers.
- Ensure glycemic control.
- Monitor and address risk factors.
- Offer pressure offloading devices and shoes with a wider toe box.
- Perform callous paring or wound debridement.
- Provide moist wound healing.
- Provide patient and caregiver education.
- Provide topical treatment.
- Restore or improve arterial flow.
- Treat infections.
Our approach
To ensure a positive impact on diabetic foot ulcers, our nursing teams worked to align acute care and ambulatory practice. The ambulatory Wound, Ostomy, Continence (WOC) nurses and RNs partnered with the acute care WOC nurses to support patient needs, educate patients on foot inspection and infection, collect and analyze data, and engage provider stakeholders. We researched diabetic foot ulcer healing rates and treatment modalities and used this information to guide practice and influence providers.
We began with retrospective chart reviews (June 2018 to July 2019) of new outpatients with diabetes. Next, we conducted a literature review and gap/opportunity analysis, which revealed the benefits of foot temperature for early infection identification and knee walkers as offloading devices for patients who can’t tolerate a total contact cast or below-knee immobilizers.
We collaborated with the nursing, surgery, podiatry, and medicine departments to develop a diabetic foot ulcer guideline, staff education, and an implementation plan. In addition, we partnered with the hospital retail pharmacy to provide patients with affordable infrared thermometers and knee walkers. We also developed standardized patient education and diabetic wound assessment and incorporated it into the electronic health record.
Throughout implementation of the new practice, we reviewed patients at risk for diabetic foot ulcers. Following implementation, the team evaluated the findings, updated and engaged with the team, and made modifications as needed.
Literature review findings
Commonalities found during the literature review included key steps for diabetic foot ulcer healing success, such as offloading, standard moist wound therapy, diabetes management, and debridement. These seemed routine in our practice. We needed to dig deeper to uncover interventions to complement our routine care and increase the number of patients who could achieve 50% closure in 4 weeks.
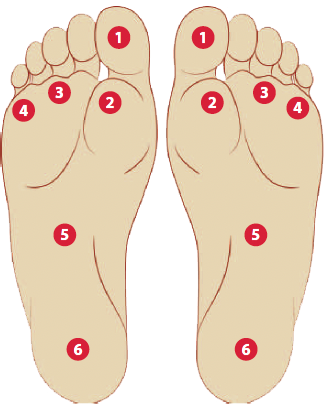
The literature review validated the importance of passive foot temperature surveillance. Lung and colleagues note that infrared thermography can aid early detection of plantar tissue inflammation, and the International Working Group on the Diabetic Foot suggests using an infrared thermometer at various points bilaterally during foot inspection to assess temperature variance. A 4° difference may indicate an underlying area of inflammation or infection. (See Foot temperature.)
Foot temperature
Best practice recommends taking foot temperatures at each visit of a patient with diabetes. Using an infrared thermometer, take bilateral temperatures at various points during foot inspection to assess variance. A 4°difference may suggest inflammation or infection.
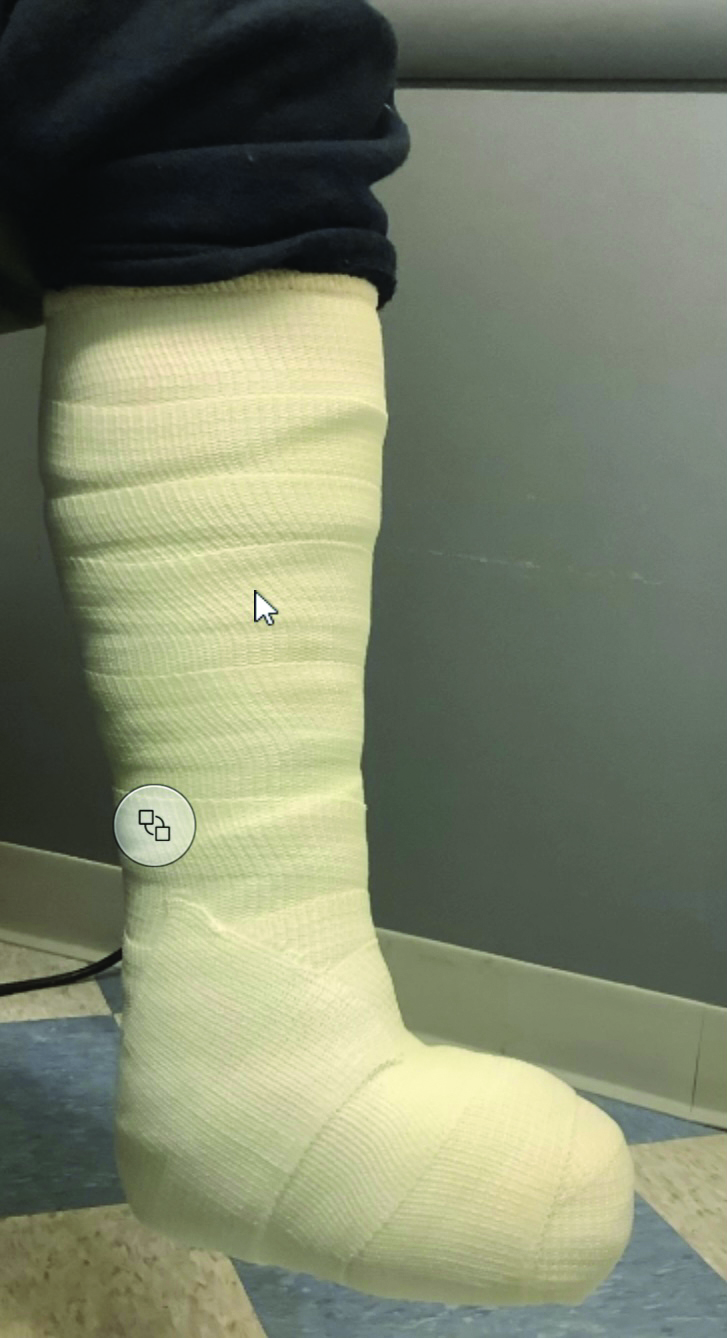
The literature also documents the reduction of plantar and toe pressure to accommodate structural changes as critical in preventing and addressing foot ulcers. Several methods can help reduce pressure and plantar tissue stress, such as casting, offloading devices, orthotics, and surgical procedures. However, Lazzarini and Jarl note that providers frequently don’t prescribe—and many patients don’t follow—best practice offloading treatments. Nonremovable knee-high offloading devices remain the gold standard for treating a plantar diabetic foot ulcer. Lack of access to these devices, as well as cost, patient stability, or patient adherence, may lead clinicians to opt for therapeutic footwear and offloading knee walkers instead.
The literature review also highlighted that wound management and goals of topical treatment should include debridement and moist wound healing. Serial weekly debridement (removing devitalized tissue and bacteria) for the first 4 weeks has been shown to reduce median wound area by as much as 54%. Moist wound healing maintains the wound bed pH, temperature, and growth factors, all of which increase collagen synthesis, cell proliferation, and closure. Treatments include topical dressings, skin substitutes, and hyperbaric oxygen therapy.
Practice in action
We identified several gaps and areas for practice modification, including scheduling all new patients with diabetic foot ulcers for weekly visits during the first 4 weeks of care. The COVID-19 pandemic forced us to adapt and develop at-home measuring guides and instructions so we could convert patients to telehealth visits and still achieve four visits in 4 weeks.
At each visit, we implemented foot temperature checks to assess for potential infection or risk of infection. We also measured wound change and alerted providers when a wound stabilized or stalled (<30% reduction in size). In addition, each visit included patient instructions for performing daily temperature and skin checks. To facilitate at-home temperature checks, we collaborated with the retail pharmacy to simplify patient purchases of infrared thermometers. This collaboration also included the purchase of knee walkers to aid offloading as well as topical treatments.
Acute care and ambulatory WOC nurses met weekly to review admitted patients with foot ulcers and determine the need for lab testing, studies, and vascular intervention as well as post-discharge advanced wound treatment (such as hyperbaric oxygen therapy, total contact casting, or skin substitutes).
All patient visits included data collection of wound size, blood-sugar level, foot temperature, and relevant labs and studies. At monthly manager meetings, the WOC nurses analyzed healing changes and shared findings with providers and the rest of the nursing team.
We included all practice changes in the diabetic foot ulcer guideline and implemented them into clinical care and patient education. These interventions and regular communication with providers increased awareness of our team goal to reduce wound size by 50% within the first 4 weeks of caring for a new diabetic foot ulcer.
The project facilitated increased communication between nurses and providers. Ambulatory and acute care nurses guided providers in best practices and suggested labs, studies, or advanced wound treatments that might hasten healing and transition a stable or stalled wound into a healing wound. Daily ambulatory nurse huddles and monthly team acute care WOC nurse and ambulatory RN meetings helped increase team accountability and assessment skills for early identification of diabetic foot ulcers.
Outcomes and goals met
 Since 2018, we’ve improved early identification of diabetic foot ulcers and increased the number that reduced 50% in size during the first 4 weeks of treatment. In 2018, we identified 54 new diabetic foot ulcers; 20 reduced 50% during the first 4 weeks of treatment. In 2019, we identified 99 ulcers; 51 met the goal. In 2020, of the 121 identified foot ulcers, 76 reduced 50% during the first 4 weeks. In 2021 and 2022, respectively, 137 of 196 and 107 of 137 new diabetic foot ulcers met the goal. (See Wound closure goals.)
Since 2018, we’ve improved early identification of diabetic foot ulcers and increased the number that reduced 50% in size during the first 4 weeks of treatment. In 2018, we identified 54 new diabetic foot ulcers; 20 reduced 50% during the first 4 weeks of treatment. In 2019, we identified 99 ulcers; 51 met the goal. In 2020, of the 121 identified foot ulcers, 76 reduced 50% during the first 4 weeks. In 2021 and 2022, respectively, 137 of 196 and 107 of 137 new diabetic foot ulcers met the goal. (See Wound closure goals.)
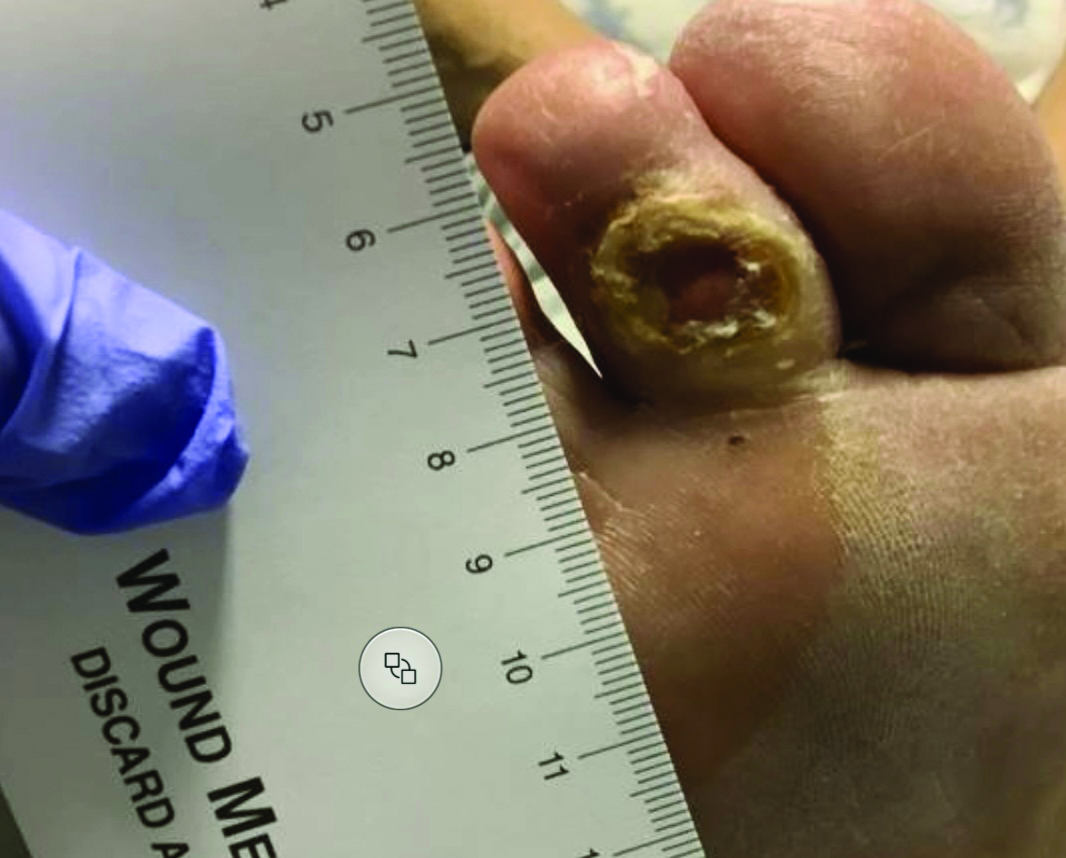
Diabetic foot ulcers vary in presentation and tissue damage, as well as modalities used to aid healing. Examples of patients with diabetic foot ulcers that reduced in size by 50% within 4 weeks include a 60-year-old man with a history of diabetes, hypertension, and vitamin B12 deficiency; a 68-year-old man with a history of diabetes, atrial fibrillation, peripheral vascular disease, hypertension, and foot cellulitis; and a 53-year-old woman with a history of diabetes, hypertension, Barret’s esophagus, and osteomyelitis of the right toe. (See Healing wounds.)
Healing wounds
The following photos illustrate wound closure using different modalities in patients with various presentations.





Systematic, holistic strategy
Developing a foot ulcer may signal serious disease and comorbidities, and treatment can prove complex and costly. Without early and optimal intervention, the wound can rapidly deteriorate, leading to amputation of the affected limb.
Our findings support the need for a systematic and holistic approach to diabetic foot ulcer care, as well as the need for easy patient access to tools, such as rolling offloading walkers, infrared thermometers, and topical treatment. Healthcare professionals should follow a standardized and consistent strategy for evaluating foot ulcers and involve the patient in education to encourage accountability and adherence.
Lisa Hill is regional director of wound healing at Jefferson Methodist Hospital in Philadelphia, Pennsylvania, and Jefferson Lansdale Hospital in Lansdale, Pennsylvania. Kathleen Petrillo is program coordinator of wound care ambulatory setting at Jefferson Lansdale Hospital. Amy Buchanan is a certified wound, ostomy continence nurse (CWOCN) at Jefferson Lansdale Hospital. Ayana Brown is a CWOCN at Jefferson Methodist Hospital. Connor Hill is senior associate at Point 72 in Stamford, Connecticut. Mercedes Monari is a CWOCN at Jefferson Lansdale Hospital. Jacqueline Harris is program coordinator at Jefferson Methodist Hospital. Kathleen Rose is an ambulatory staff nurse at Jefferson Methodist Hospital.
American Nurse Journal. 2024; 19(7). Doi: 10.51256/ANJ072437
References
Armstrong DG, Swerdlow MA, Armstrong AA, Conte MS, Padula WV, Bus SA. Five year mortality and direct costs of care for people with diabetic foot complications are comparable to cancer. J Foot Ankle Res. 2020;13(1):16. doi:10.1186/s13047-020-00383-2
Bonham P, Brunette G, Crestodina L, et al. 2021 Guideline for management of patients with lower-extremity wounds due to diabetes mellitus and/or neuropathic disease: An executive summary. J Wound Ostomy Continence Nurs. 2022;49(3):267-85. doi:10.1097/won.0000000000000860
Bryant R, Nix D. Acute and Chronic Wounds. 6th ed. Philadelphia, PA: Elsevier Health Sciences; 2023.
Bus SA, Armstrong DG, Gooday C, et al. Guidelines on offloading foot ulcers in persons with diabetes (IWGDF 2019 update). Diabetes Metab Res Rev. 2020;36(suppl 1):e3274. doi:10.1002/dmrr.3274
Chen H, Cai C, Xie J. The effect of an intensive patients’ education program on anxiety, depression and patient global assessment in diabetic foot ulcer patients with Wagner grade ½: A randomized, controlled study. Medicine. 2020;99(6):e18480. doi:10.1097/md.0000000000018480
Edmonds M, Manu C, Vas P. The current burden of diabetic foot disease. J Clin Orthop Trauma. 2021;17:88-93. doi:10.1016/j.jcot.2021.01.017
Jeffcoate WJ, Vileikyte L, Boyko EJ, Armstrong DG, Boulton AJM. Current challenges and opportunities in the prevention and management of diabetic foot ulcers. Diabetes Care. 41(4):645-52. doi:10.2337/dc17-1836
Lazzarini PA, Jarl G. Knee-high devices are gold in closing the foot ulcer gap: A review of offloading treatments to heal diabetic foot ulcers. Medicina. 2021;57(8):941. doi:10.3390/medicina57090941
Lung CW, Wu FL, Liao F, Pu F, Fan Y, Jan YK. Emerging technologies for the prevention and management of diabetic foot ulcers. J Tissue Viability. 2020;29(2):61-8. doi:10.1016/j.jtv.2020.03.003
McDermott KM, Fang M, Boulton AJM, Selvin E, Hicks CW. Etiology, epidemiology, and disparities in the burden of diabetic foot ulcers. Diabetes Care. 2023;46(1):209-21. doi:10.2337/dci22-0043
McNichol L, Ratliff C, Yates S. Wound, Ostomy, and Continence Nurses Society Core Curriculum: Wound Management. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2021.
Oliver TI, Mutluoglu M. Diabetic foot ulcer. StatPearls. August 8, 2023. ncbi.nlm.nih.gov/books/NBK537328
Pop-Busui R, Boulton AJ, Feldman EL, et al. Diabetic neuropathy: A position statement by the American Diabetes Association. Diabetes Care. 2017;40(1):136-54. doi:10.2337/dc16-2042
Schaper NC, Netten JJ, Apelqvist, J, Bus SA, Hinchliffe FJ, Lipsky BA. Practical guidelines on the prevention and management of diabetic foot disease (IWGDF 2019 update) Diabetes Metab Res Rev. 2020;36(suppl 1):e3266. doi:10.1002/dmrr.3266
Sheehan P, Jones P, Caselli A, Giurini JM, Veves A. Percent change in wound area of diabetic foot ulcers over a 4-week period is a robust predictor of complete healing in a 12-week prospective trial. Diabetes Care. 2003;26(6):1879-82. doi:10.2337/diacare.26.6.1879
Snyder RJ, Frykberg RG, Rogers LC, et al. The management of diabetic foot ulcers through optimal off-loading: building consensus guidelines and practical recommendations to improve outcomes. J Am Podiatr Med Assoc. 2014;104(6):555-67. doi:10.7547/8750-7315-104.6.555
Ugwu E, Adeleye O, Gezawa I, Okpe I, Enamino M, Ezeani I. Predictors of lower extremity amputation in patients with diabetic foot ulcer: Findings from MEDFUN, a multi-center observational study. J Foot Ankle Res. 2019;12:34. doi:10.1186/s13047-019-0345-y
Key words: diabetes, diabetic foot ulcer, diabetic ulcer healing, diabetic education, wound healing

















1 Comment. Leave new
Valuable information that is quick and easy to read and easily apply to improve patient care