Nurse knowledge of etiology, diagnostic tests, and treatment options can help ensure a good outcome.
- Chylothorax, a rare condition, can prove challenging to diagnose and manage.
- Chylomicrons or high triglyceride levels make a definitive diagnosis in the pleural fluid.
- Treatment should focus on reducing the flow of chylous fluid and preventing complications.
- Prognosis depends on the underlying cause, severity of leakage, treatment response, and comorbid condition.
Chylothorax, a rare complex medical condition characterized by the accumulation of chyle (a lymphatic fluid) in the pleural cavity, carries high morbidity and mortality with increased hospital stays and costs. The condition can occur as a result of trauma, surgical procedures, tumors, or an underlying disease. Chylothorax poses significant challenges in clinical management because of its potentially life-threatening complications. Severe impact on respiratory function and nutritional status can increase hospital stays and healthcare costs.
Clinical management of chylothorax varies, so implementing an organized stepwise approach to care can improve patient outcomes. Components of this approach include a thorough evaluation of the patient’s condition—including diagnostic tests and imaging—to understand the underlying cause and associated complications. Positive diagnosis requires a tailored management strategy aimed at alleviating symptoms, addressing the underlying cause, and preventing further complications. Treatment options may include conservative measures such as dietary modifications and nutritional support. Severe chylothorax may require invasive interventions such as thoracic duct ligation or embolization.
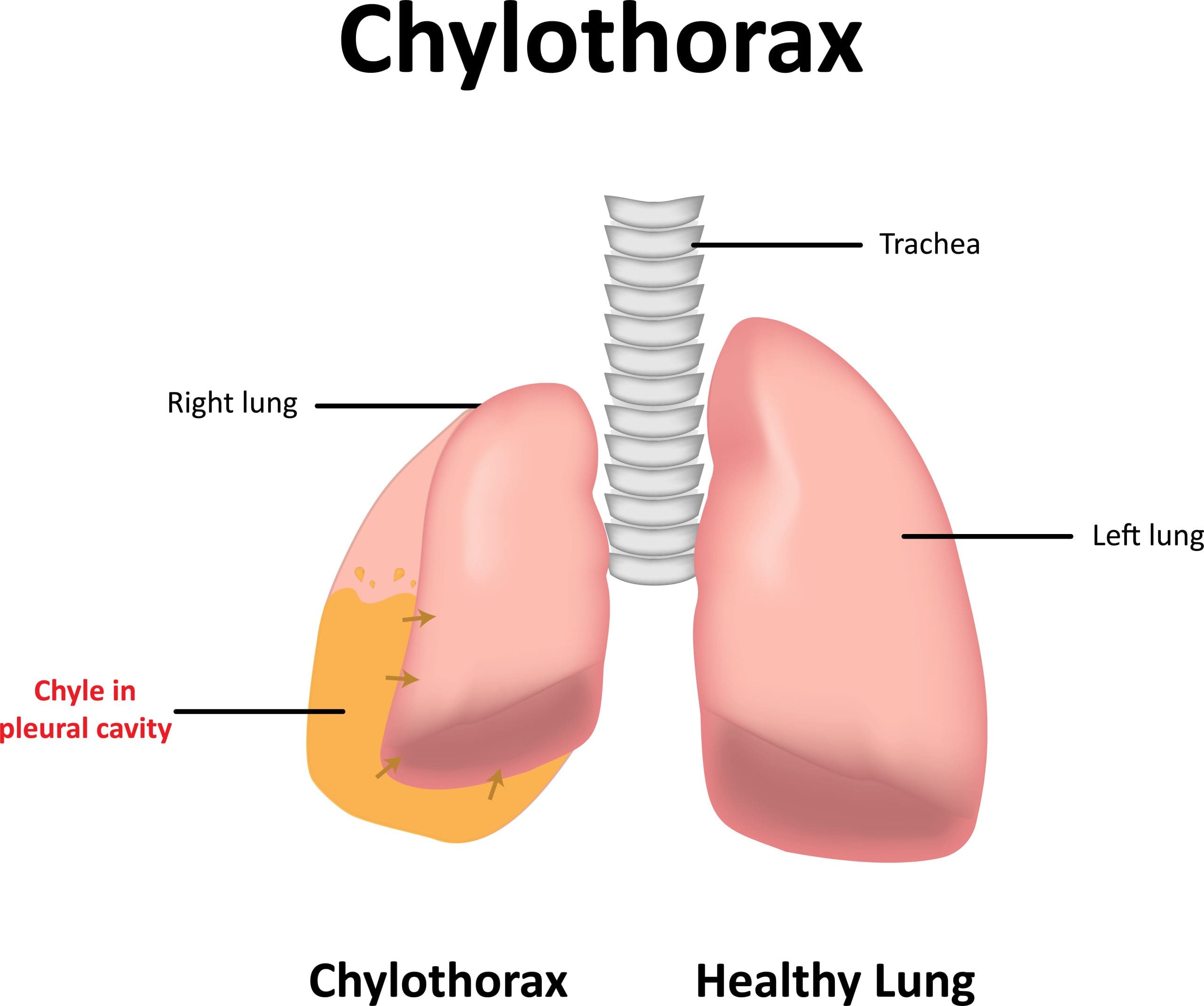
What is chylothorax?
Chylothorax occurs as a result of a thoracic duct disruption, which causes the leak of chyle (a milky-white fluid composed of lipids, proteins, and lymphocytes usually transported through the lymphatic system) into the pleural cavity (the space between the lungs and the chest wall). The thoracic duct, a major lymphatic vessel, drains lymphatic fluid from the lower half and the upper left side of the body into the bloodstream. The lymphatic system plays a role in transporting dietary fats, removing waste products, and supporting the immune system.
Anatomy and pathophysiology
The lymphatic system, a network of vessels, lymph nodes, and organs, has three primary functions: transport lipids and fat-soluble vitamins to the systemic circulation, collect excess fluid from the interstitial cavity and extravasated and return them to the circulation, and return lymphocytes to the systemic circulation. A healthy adult circulates 1.5 L to 4 L of lymphatic fluid per day.
Lymph drainage starts from the lower extremities, liver, and intestine and joins the thoracic duct (the primary channel of thoracic drainage) at the cisterna chyli in T12. It crosses from the right side of the body to the left around T4/T5, ascends to the dorsal area of the aortic arch to the anterior of the subclavian artery, and ends in the left side of the neck at the junctions of the subclavian and the internal jugular veins.
The thoracic duct contains numerous valves that prevent the backflow of chyle. Normal respiration pumps chyle toward venous circulation. The lymphatic duct, which has no chyle, drains lymphatic flow from the right side of the head, neck, thorax, right upper extremity, and the right side of the heart.
Causes and risk factors
Chylothorax can occur through various causes, including trauma, a tumor compressing the thoracic duct, congenital conditions, and a number of syndromes. In some cases, no underlying cause can be identified. (See Etiology.)
Etiology
Chylothorax in adults and children can result from various causes and conditions.
- Congenital
- Atresia of thoracic duct
- Lymphangiectasia
- Lymphangiomatosis
- Lymphatic malformation
- Various syndromes and diseases (for example, Gorham-Stout, hydrops fetalis, Noonan, Turner)
- Heart failure
- High central venous pressure
- After Fontan surgery
- Thrombus of superior vena cava or subclavian vein
- Infection (adults only)
- Histoplasmosis
- Tuberculosis
- Malignancies
- Lymphoma
- Neuroblastoma
- Sarcoma
- Teratoma
- Postoperative complications
- Cardiothoracic surgery
- Pulmonary resection
- Radical neck dissection
- Other (adults only)
- Benign tumor
- Cirrhosis
- Sarcoidosis
The presentation of chylothorax varies depending on the underlying cause. For example, chylothorax caused by trauma or iatrogenic injury may present acutely with symptoms such as shortness of breath and chest pain. If the condition occurs as a result of cancer, the patient may experience more gradual symptoms, such as persistent cough, fatigue, and weight loss. Children and infants may experience feeding difficulties, failure to thrive, and swelling of the limbs or face. Some patients may have no symptoms, and identification occurs incidentally in imaging studies. (See Signs & symptoms.)
Signs & symptoms
Symptoms of chylothorax can affect various systems based on the underlying condition.
- Cardiovascular
- Chest pain
- Hypotension or signs of shock in extreme cases
- Tachycardia or palpitations
- GI
- Malnutrition
- Reduced appetite
- Weight loss
- Respiratory
- Decreasing breath sounds on the affected side of the lung
- Dry or persistent cough
- Dyspnea
- Shortness of breath
- Skin/musculoskeletal
- Edema of the limbs, fact, or neck
- Fatigue
- Weakness
In the event of infection, a patient may experience, chills, fever, and night sweats.
How is chylothorax diagnosed?
Confirmation of chylothorax diagnosis occurs via analysis of fluid obtained from a thoracentesis or chest tube drainage. In 50% of cases, the fluid will have a milky appearance due to the high lipid content. Providers make a definitive diagnosis if the pleural fluid has triglyceride levels greater than 110 mg/dL or contains chylomicrons (protein and lipid complexes synthesized in the jejunum and transported to the circulation by the thoracic duct). Identifying the underlying cause of chylothorax may require imaging studies, such as an ultrasound, computed tomography scan, or magnetic resonance imaging. (See Lab values).
Lab values
The following laboratory criteria indicate chylothorax:
- Cholesterol: <200 mg/dL
- Cholesterol crystals: Absent
- Chylomicrons: Present
- Lymphocyte: >80%
- Triglyceride: >110 mg/dL
Prognosis
Chylothorax can prove life-threatening if not managed promptly and effectively, especially if it leads to respiratory compromise and significant electrolyte imbalance. According to Ahn and Hoseok and Bhatnagar and colleagues, treatment has a reported resolution rate ranging from 16% to 75%; however, that rate can be lower in patients with high-volume chylous output (>1,000 mL/day). Surgical interventions show a success rate of approximately 90%, with complications occurring in up to 38.3% of patients. Refractory cases may require thoracic duct ligation, chemical pleurodesis, or embolization; the success rate of these procedures ranges from 60% to 90%. Conservative management with dietary modifications, chest tube drainage, and medical therapy can resolve chylothorax in up to 80% of cases. Overall, patients have a good prognosis if the condition is identified early and treated promptly and effectively.
Several factors—underlying cause, chyle leakage severity, treatment response, and complications and comorbidities—influence chylothorax prognosis.
Underlying cause. Chylothorax after cardiac surgery or associated with cancer may have a higher mortality rate than chylothorax caused by trauma or iatrogenic injury.
Chyle leakage severity. Significant or persistent chyle leaks may lead to respiratory distress, electrolyte imbalances, nutritional deficiencies, and other complications. Prompt identification and management of chylothorax can help improve outcomes.
Treatment response. Treatment success plays a crucial role in chylothorax prognosis. Conservative management, which includes dietary modifications (such as a low-fat diet or medium-chain triglyceride supplementation), chest tube drainage, and medical therapy (such as somatostatin analogs), can lead to the resolution of chylothorax in many cases. However, to achieve successful outcomes, refractory cases may require surgical interventions, such as thoracic duct ligation, chemical pleurodesis, or embolization.
Complications and comorbidities. Chylothorax and its treatment can result in various complications, such as infections, pleural adhesions, or recurrence of chyle leakage. The presence of underlying comorbidities or complications related to the existing medical condition also can impact overall prognosis.
What are the treatment options?
Best practice management of chylothorax depends on the underlying cause and severity of the condition. Nursing care aims to reduce chyle flow while waiting for the resolution of chylous effusion or healing. An organized, stepwise approach, which begins with diagnosis confirmation and ends with complication prevention, supports treatment efficacy.
1. Diagnosis confirmation
Diagnostic tests require aspiration of fluid. Effusion size that compromises breathing or significant fluid collection require chest tube placement and continuous drainage monitoring. Repeat thoracentesis can be performed as needed based on thoracic ultrasound-guided studies. (See Diagnostic tests.)
Diagnostic tests
The following steps and corresponding diagnostic procedures ensure confirmation of chylothorax.
2. Dietary modification
A trial of an oral low-fat diet or a medium-chain triglyceride diet via feeding tube can aid the reduction of chyle flow. If the patient can’t tolerate enteral feeding, total parenteral nutrition can be administered.
3. Medical management
Some patients will require treatment with octreotide, a synthetic long-acting somatostatin analog that decreases intestinal chyle production and reduces chyle flow to the lymphatic system. Octreotide also reduces intestinal motility, thereby decreasing gastric, pancreatic, and biliary secretions and reducing the thoracic duct’s lymphatic flow.
4. Surgery
In rare cases, a patient may require surgery to repair or bypass the thoracic duct or to remove a compressive tumor. If medical management fails to reduce chyle flow and thoracic duct healing, the provider may order chemical pleurodesis (obliterate the pleural space by adhering the visceral pleura to the parietal pleura). Many experts advocate for 4 weeks of medical therapy before surgical management.
5. Prevention and treatment of complications
Known complications of chylothorax include malnutrition, hypovolemia, hyponatremia, fluid imbalance, respiratory distress, increased thrombosis, and immune deficiency. A collaborative approach involving various healthcare professionals, such as pulmonologists, surgeons, and dietitians, can help effectively manage and prevent debilitating chylothorax complications. Patient and family education also aids optimal outcomes.
Nursing care
Nurses play a vital role in the management of patients with chylothorax. Assess patients with chylothorax frequently during each shift, and monitor vital signs, oxygen saturation, and cardio-respiratory status. Quantifying chest tube drainage will provide data to assess improvement and guide the care team regarding fluid and electrolyte status. Watch the patient for signs of infection, such as fever or increased white blood cell count, monitor the chest tube insertion site, and provide wound care as necessary. Assess and accurately record chest tube drainage every hour. Notify the provider immediately in the event of profuse output (>500 mL/day).
Educate patients and their families about chylothorax and its management. Provide information about the underlying cause, treatment options, dietary modifications, and the importance of adherence to therapy.
Work collaboratively with the healthcare team to provide nutritional support. Monitor the patient’s weight, fluid, and electrolyte balance and provide appropriate nutritional supplements. Take advantage of nutritionist or dietitian consultations to ensure good outcomes. Administer medications as prescribed to reduce the production and flow of chyle, and monitor the patient for any adverse drug reactions and provide appropriate interventions.
Patients and their families will require emotional support while the healthcare team works to manage the chylothorax. Listen to their concerns, provide information, and refer them to appropriate resources.
Work collaboratively
Chylothorax, with its varying etiologies, requires an interprofessional care approach to address the underlying cause and minimize complications. Working collaboratively can aid the development of a comprehensive plan of care to address the patient’s physical, psychological, and social needs. With appropriate management, most patients with chylothorax can achieve positive outcomes and improve their quality of life.
Ninotchka Brydges is a critical care advanced practice provider at the University of Texas Medical Branch in Webster. Riza V. Mauricio is an assistant professor at the University of Texas Health Science Center in Houston.
American Nurse Journal. 2024; 19(6). Doi: 10.51256/ANJ062420
References
Agrawal A, Chaddha U, Kaul V, Desai A, Gillaspie E, Maldonado F. Multidisciplinary management of chylothorax. Chest. 2022;162(6):1402-12. doi:10.1016/j.chest.2022.06.012
Ahn HY, I Hoseok. Non-conservative management of chylothorax. J Chest Surg. 2021;54(4):325-9. doi:10.5090/jcs.21.056
Bhatnagar M, Fisher A, Ramsaroop S, Carter A, Pippard B. Chylothorax: Pathophysiology, diagnosis, and management—A comprehensive review. J Thorac Dis. 2024;16(2):1645-61. doi:10.21037/jtd-23-1636
Bender B, Murthy V, Chamberlain RS. The changing management of chylothorax in the modern era. Eur J Cardiothorac Surg. 2016;49(1):18-24. doi:10.1093/ejcts/ezv041
Büyükşahin HN, Emiralioğlu N, Özcan HN, et al. Evaluation of clinical findings in children with chylothorax: A descriptive study. Turk Arch Pediatr. 2023;58(1):28-33. doi:10.5152/TurkArchPediatr.2022.22182
Cheng L, Huang M, Wei J, Xu H, Zhou M, Jiang L. Complete resolution of chylothorax with ibrutinib in chronic lymphocytic leukemia: A case report. Ann Palliat Med. 2022;11(5):1833-7. doi: 10.21037/apm-21-989
Cholet C, Delalandre C, Monnier-Cholley, Le Pimpec-Barthes F, El Mouhadi S, Arrivé L. Nontraumatic chylothorax: Nonenhanced MR lymphography. Radiographics, 2020;40(6):1554-73. doi:10.1148/rg.2020200044
Gary P, Gianniosis M, Ryu J, Flynn S. Chylothorax as a complication of Waldenström macroglobulinaemia with a patient’s perspective. BMJ Case Rep. 2021;14(5):e241707. doi:10.1136/bcr-2021-241707
Heffner, JE. Etiology, clinical presentation, and diagnosis of chylothorax. UpToDate. May 20, 2022. uptodate.com/contents/etiology-clinical-presentation-and-diagnosis-of-chylothorax
Hermon M, Tenner E, Burda G, Strohmaier W, Schlager G, Golej J. Chylothorax and chylous-like diseases in children: Clinical management. Front Pediatr. 2029;7:258. doi: 10.3389/fped.2019.00258
Mierzejewski M, Korczynski P, Krenke R, Janssen JP. Chemical pleurodesis–—A review of mechanisms involved in pleural space obliteration. Respir Res. 2019;20(1):247. doi:10.1186/s12931-019-1204-x
Otoupalova E, Meka SG, Dogra S, Dalal B. Recurrent chylothorax: A clinical mystery. BMJ Case Rep. 2017. doi:10.1136/bcr-2017-220750
Reisenauer JS, Puig CA, Reisenauer CJ, et al. Treatment of postsurgical chylothorax. Ann Thorac Surg. 2018;105(1):254-262. doi:10.1016/j.athoracsur.2017.07.021
Riley LE, Ataya A. Clinical approach and review of causes of a chylothorax. Respir Med. 2019;157(1):7-13. doi:10.1016/j.rmed.2019.08.014
Sholz GA, Sirbu H, Semrau S, Anders K, Mackensen A, Spriewald BM. Persisting right-sided chylothorax in a patient with chronic lymphocytic leukemia: A case report. J Med Care Rep. 2011;5:492. doi:10.1186/1752-1947-5-492
Wiesner S, Loch E, Uller W, et al. Evaluation of treatment options for postoperative and spontaneous chylothorax in adults. Interact Cardiovasc Thorac Surg. 2021;33(4):527-33. doi:10.1093/icvts/ivab127
Key words: Chylothorax, lymphatic system, chest tube drainage